Let G be a complex classical group, and let V be its defining representation (possibly plus a copy of the dual). A foundational problem in classical invariant theory is to write down generators and relations for the ring of G-invariant polynomial functions on the space  $\mathcal P^m(V)$ of degree-m homogeneous polynomial functions on V. In this paper, we replace
$\mathcal P^m(V)$ of degree-m homogeneous polynomial functions on V. In this paper, we replace  $\mathcal P^m(V)$ with the full polynomial algebra
$\mathcal P^m(V)$ with the full polynomial algebra  $\mathcal P(V)$. As a result, the invariant ring is no longer finitely generated. Hence, instead of seeking generators, we aim to write down linear bases for bigraded components. Indeed, when G is of sufficiently high rank, we realize these bases as sets of graphs with prescribed number of vertices and edges. When the rank of G is small, there arise complicated linear dependencies among the graphs, but we remedy this setback via representation theory: in particular, we determine the dimension of an arbitrary component in terms of branching multiplicities from the general linear group to the symmetric group. We thereby obtain an expression for the bigraded Hilbert series of the ring of invariants on
$\mathcal P(V)$. As a result, the invariant ring is no longer finitely generated. Hence, instead of seeking generators, we aim to write down linear bases for bigraded components. Indeed, when G is of sufficiently high rank, we realize these bases as sets of graphs with prescribed number of vertices and edges. When the rank of G is small, there arise complicated linear dependencies among the graphs, but we remedy this setback via representation theory: in particular, we determine the dimension of an arbitrary component in terms of branching multiplicities from the general linear group to the symmetric group. We thereby obtain an expression for the bigraded Hilbert series of the ring of invariants on  $\mathcal P(V)$. We conclude with examples using our graphical notation, several of which recover classical results.
$\mathcal P(V)$. We conclude with examples using our graphical notation, several of which recover classical results.
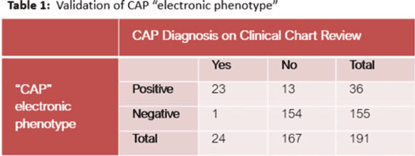
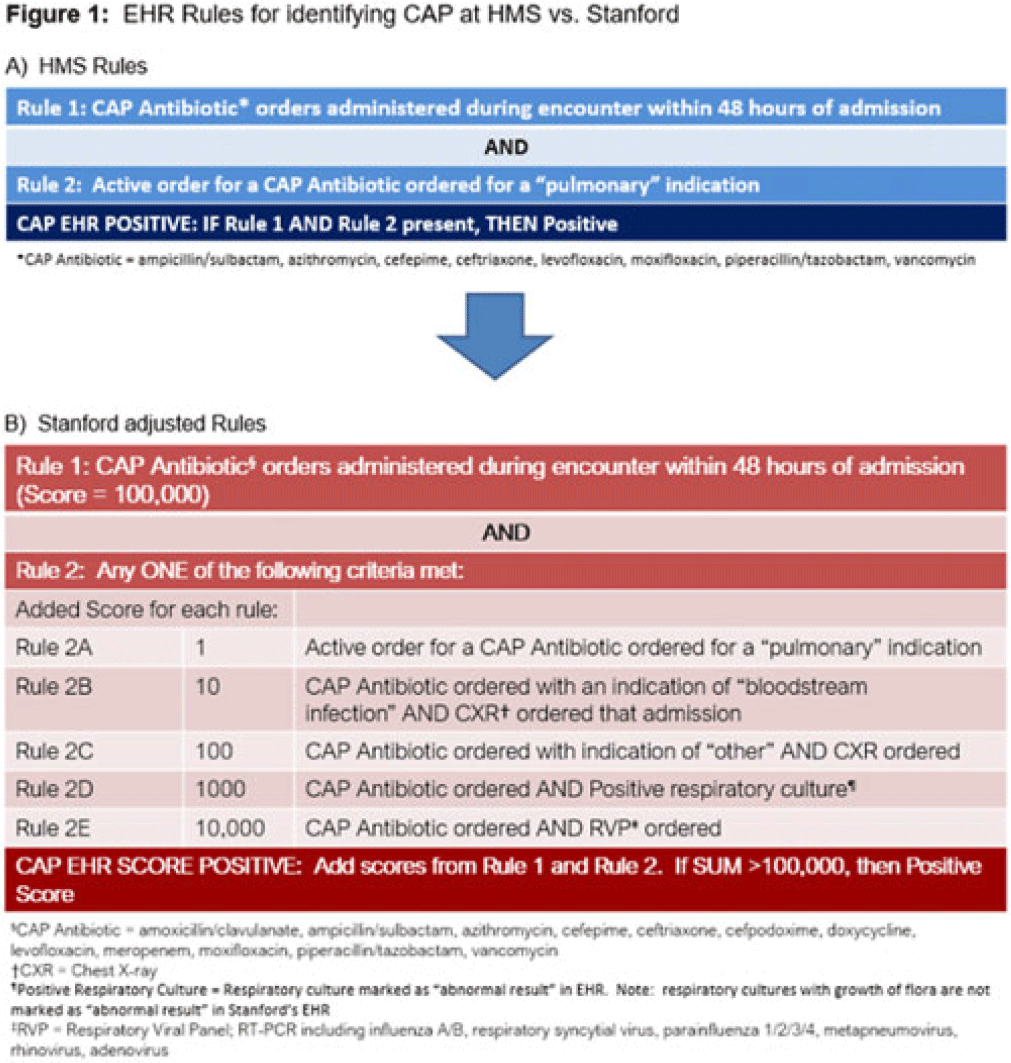
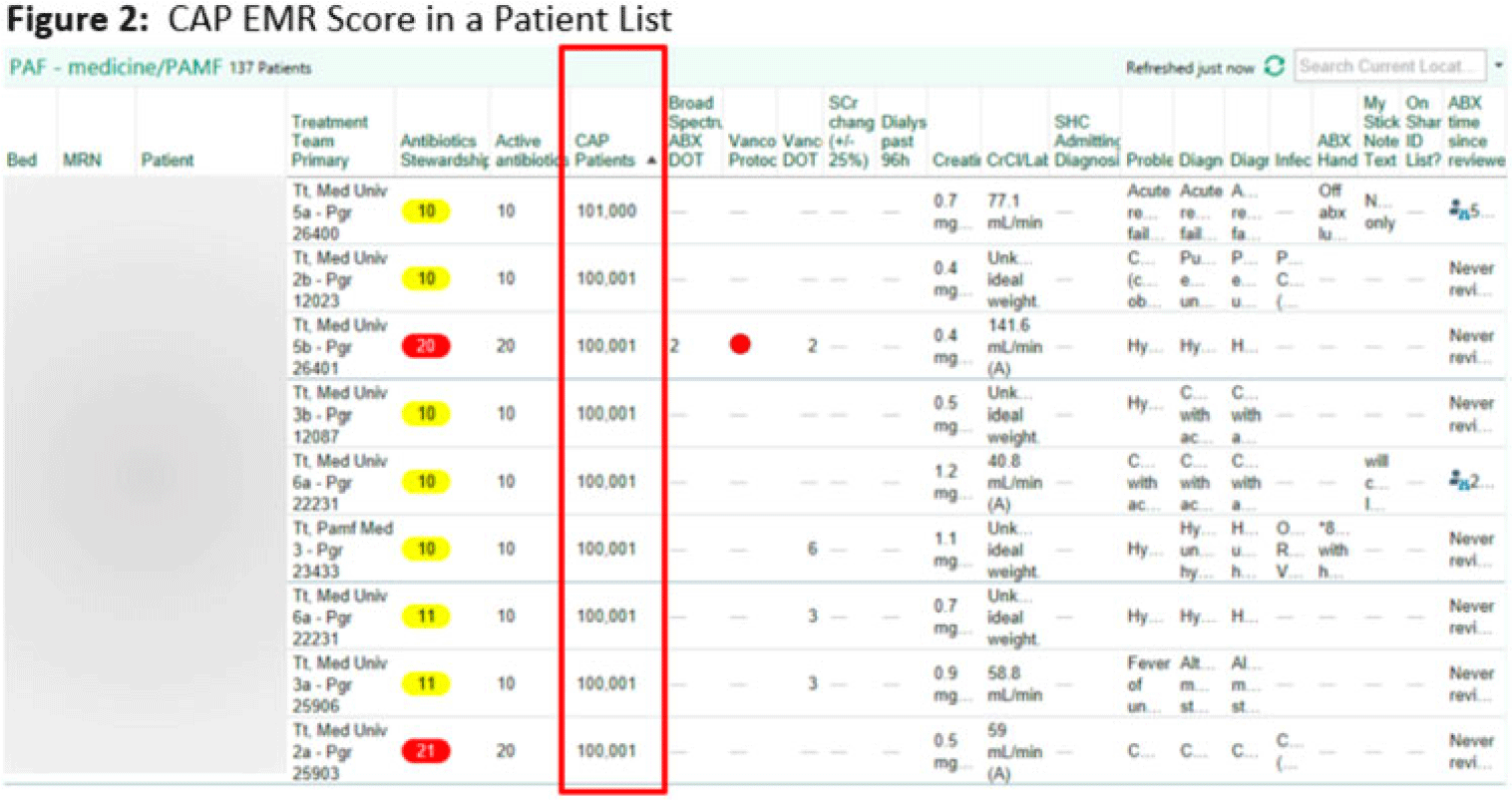
Background: Using patient data from the electronic health record (EHR) and computer logic, an “electronic phenotype” can be created to identify patients with community-acquired pneumonia (CAP) in real time to assist with syndrome-specific antimicrobial stewardship efforts.1 We adapted and validated the performance of an inpatient CAP electronic phenotype for antimicrobial stewardship interventions. Methods: An automated scoring system was created within the EHR (Epic Systems) to identify hospitalized patients with CAP based on the variables and logic listed in Fig. 1B. We adapted a score used by the Michigan Hospital Medicine Safety Consortium (HMS) to identify patients with CAP, with additions made to improve sensitivity (Fig. 1).1 The score can be displayed in a column within the EHR patient list (Fig. 2). We validated the electronic phenotype via chart review of all hospitalized patients on systemic antimicrobials admitted to a medicine team consecutively between November 8 and 18, 2021. Patients who were readmitted within the validation time frame were excluded. We assessed the performance of the electronic phenotype by comparing the score to manual chart review, where “CAP diagnosis” was defined as (1) mention of “pneumonia” or “CAP” as part of the differential diagnosis in the admission documentation, (2) antimicrobials were started within 48 hours of admission, and (3) radiographic findings were suggestive of pneumonia. After initial evaluation, the scoring system was adjusted, and performance was re-evaluated during prospective audit and feedback performed on EHR CAP–positive patients over 13 days between July 2022 and December 2022. Results: We included 191 patients in our initial validation cohort. The CAP score had high sensitivity (95.83%), specificity (92.2%), and negative predictive value (99.35%), though lower positive predictive value (63.89%) was noted (Table 2). The rules were further refined to include bloodstream infection only with Haemophilus influenza or Streptococcus pneumoniae in rule 2B, and azithromycin was removed from “CAP antibiotics.” After these changes, repeated evaluation of 88 patients with positive CAP EHR score was performed, and only 20 (23%) were considered false-positive results. Conclusions: Electronic phenotypes can be used to create automated tools to identify patients with CAP with reasonable performance. Data from this tool can be used to guide more focused antimicrobial stewardship interventions and clinical decision support in the future. Reference: Vaughn VM, et al. A statewide collaborative quality initiative to improve antibiotic duration and outcomes in patients hospitalized with uncomplicated community-acquired pneumonia. Clin Infect Dis 2022;75:460–467.
Disclosures: None

