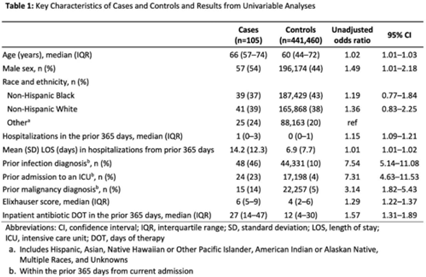
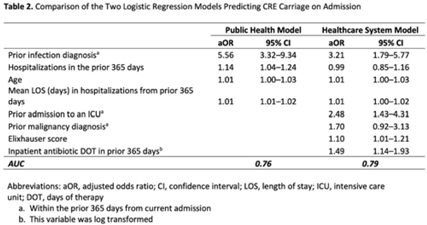
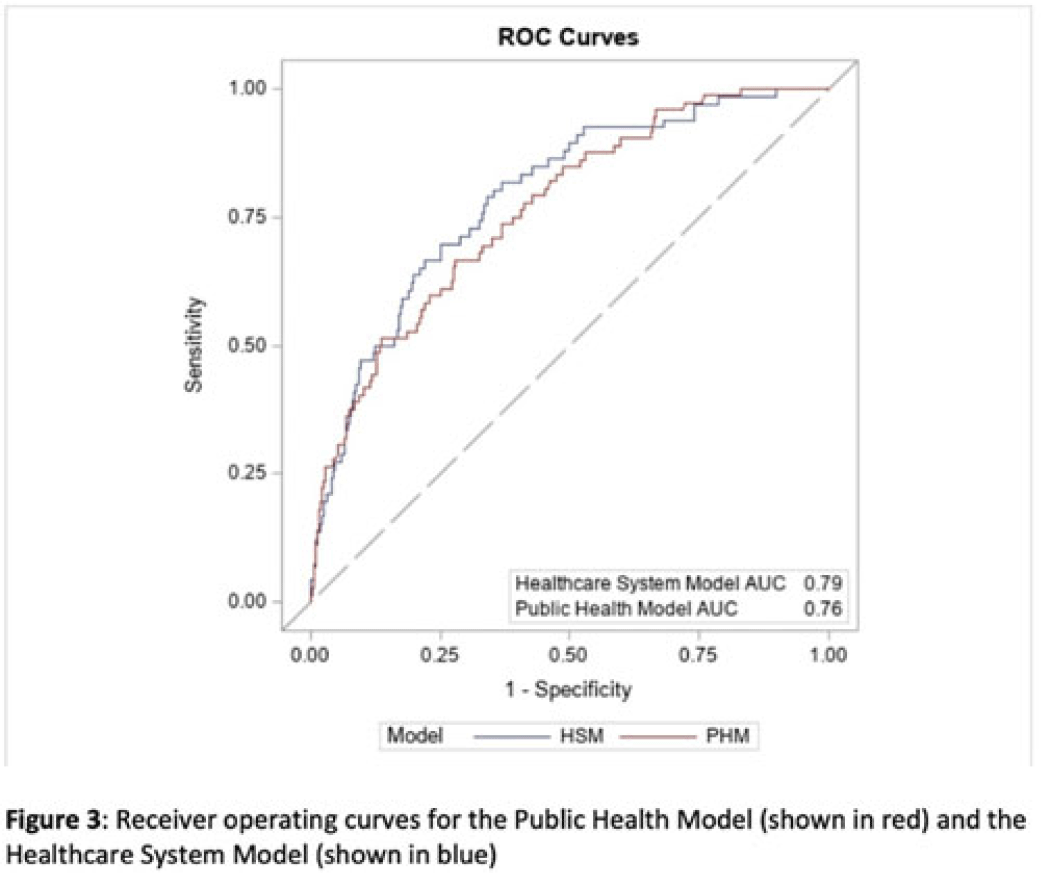
Background: Prompt identification of patients colonized or infected with carbapenem-resistant Enterobacterales (CRE) upon admission can help ensure rapid initiation of infection prevention measures and may reduce intrafacility transmission of CRE. The Chicago CDC Prevention Epicenters Program previously created a CRE prediction model using state-wide public health data (doi: 10.1093/ofid/ofz483). We evaluated how well a similar model performed using data from a single academic healthcare system in Atlanta, Georgia, and we sought to determine whether including additional variables improved performance. Methods: We performed a case–control study using electronic medical record data. We defined cases as adult encounters to acute-care hospitals in a 4-hospital academic healthcare system from January 1, 2014, to December 31, 2021, with CRE identified from a clinical culture within the first 3 hospital days. Only the first qualifying encounter per patient was included. We frequency matched cases to control admissions (no CRE identified) from the same hospital and year. Using multivariable logistic regression, we compared 2 models. The “public health model” included 4 variables from the Chicago Epicenters model (age, number of hospitalizations in the prior 365 days, mean length of stay in hospitalizations in the prior 365 days, and hospital admission with an infection diagnosis in the prior 365 days). The “healthcare system model” added 4 additional variables (admission to the ICU in the prior 365 days, malignancy diagnosis, Elixhauser score and inpatient antibiotic days of therapy in the prior 365 days) to the public health model. We used billing codes to determine Elixhauser score, malignancy status, and recent infection diagnoses. We compared model performance using the area under the receiver operating curve (AUC). Results: We identified 105 cases and 441,460 controls (Table 1). CRE was most frequently identified in urine cultures (46%). All 4 variables included in the public health model and the 4 additional variables in the healthcare system model were all significantly associated with being a case in unadjusted analyses (Table 1). The AUC for the public health model was 0.76, and the AUC for the healthcare system model was 0.79 (Table 2; Fig. 1). In both models, a prior admission with an infection diagnosis was the most significant risk factor. Conclusions: A modified CRE prediction model developed using public health data and focused on prior healthcare exposures performed reasonably well when applied to a different academic healthcare system. The addition of variables accessible in large healthcare networks did not meaningfully improve model discrimination.
Disclosures: None
Background: Effective inpatient stewardship initiatives can improve antibiotic prescribing, but impact on outcomes like Clostridioides difficile infections (CDIs) is less apparent. However, the effect of inpatient stewardship efforts may extend to the postdischarge setting. We evaluated whether an intervention targeting inpatient fluoroquinolone (FQ) use in a large healthcare system reduced incidence of postdischarge CDI. Methods: In August 2019, 4 acute-care hospitals in a large healthcare system replaced standalone FQ orders with order sets containing decision support. Order sets redirected prescribers to syndrome order sets that prioritize alternative antibiotics. Monthly patient days (PDs) and antibiotic days of therapy (DOT) administered for FQs and NHSN-defined broad-spectrum hospital-onset (BS-HO) antibiotics were calculated using patient encounter data for the 23 months before and 13 months after the intervention (COVID-19 admissions in the previous 7 months). We evaluated hospital-onset CDI (HO-CDI) per 1,000 PD (defined as any positive test after hospital day 3) and 12-week postdischarge (PDC- CDI) per 100 discharges (any positive test within healthcare system <12 weeks after discharge). Interrupted time-series analysis using generalized estimating equation models with negative binomial link function was conducted; a sensitivity analysis with Medicare case-mix index (CMI) adjustment was also performed to control for differences after start of the COVID-19 pandemic. Results: Among 163,117 admissions, there were 683 HO-CDIs and 1,009 PDC-CDIs. Overall, FQ DOT per 1,000 PD decreased by 21% immediately after the intervention (level change; P < .05) and decreased at a consistent rate throughout the entire study period (−2% per month; P < .01) (Fig. 1). There was a nonsignificant 5% increase in BS-HO antibiotic use immediately after intervention and a continued increase in use after the intervention (0.3% per month; P = .37). HO-CDI rates were stable throughout the study period, with a nonsignificant level change decrease of 10% after the intervention. In contrast, there was a reversal in the trend in PDC-CDI rates from a 0.4% per month increase in the preintervention period to a 3% per month decrease in the postintervention period (P < .01). Sensitivity analysis with adjustment for facility-specific CMI produced similar results but with wider confidence intervals, as did an analysis with a distinct COVID-19 time point. Conclusion: Our systemwide intervention using order sets with decision support reduced inpatient FQ use by 21%. The intervention did not significantly reduce HO-CDI but significantly decreased the incidence of CDI within 12 weeks after discharge. Relying on outcome measures limited to inpatient setting may not reflect the full impact of inpatient stewardship efforts and incorporating postdischarge outcomes, such as CDI, should increasingly be considered.
Funding: No
Disclosures: None
Figure 1.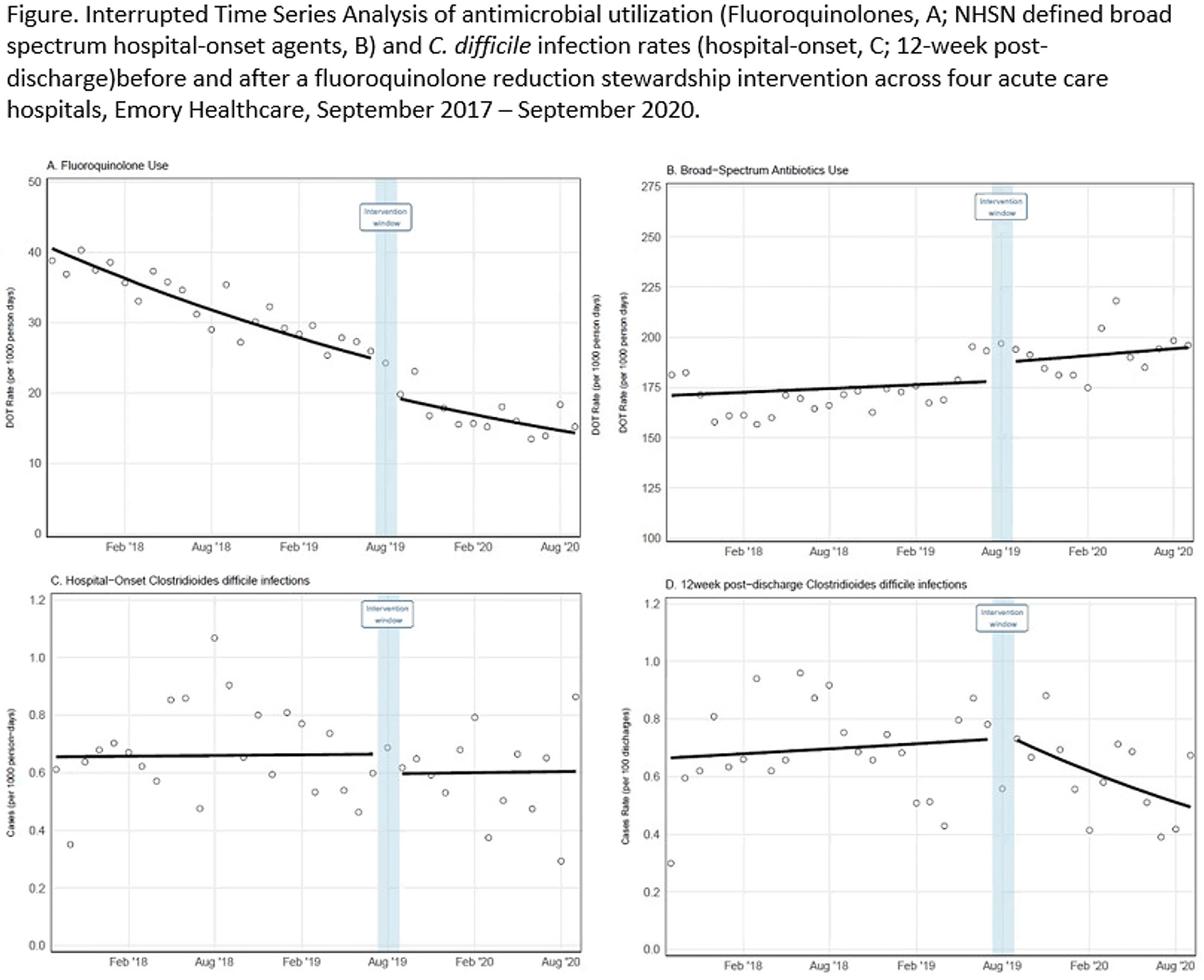
The SPARC tokamak is a critical next step towards commercial fusion energy. SPARC is designed as a high-field ( $B_0 = 12.2$ T), compact (
$B_0 = 12.2$ T), compact ( $R_0 = 1.85$ m,
$R_0 = 1.85$ m,  $a = 0.57$ m), superconducting, D-T tokamak with the goal of producing fusion gain
$a = 0.57$ m), superconducting, D-T tokamak with the goal of producing fusion gain  $Q>2$ from a magnetically confined fusion plasma for the first time. Currently under design, SPARC will continue the high-field path of the Alcator series of tokamaks, utilizing new magnets based on rare earth barium copper oxide high-temperature superconductors to achieve high performance in a compact device. The goal of
$Q>2$ from a magnetically confined fusion plasma for the first time. Currently under design, SPARC will continue the high-field path of the Alcator series of tokamaks, utilizing new magnets based on rare earth barium copper oxide high-temperature superconductors to achieve high performance in a compact device. The goal of  $Q>2$ is achievable with conservative physics assumptions (
$Q>2$ is achievable with conservative physics assumptions ( $H_{98,y2} = 0.7$) and, with the nominal assumption of
$H_{98,y2} = 0.7$) and, with the nominal assumption of  $H_{98,y2} = 1$, SPARC is projected to attain
$H_{98,y2} = 1$, SPARC is projected to attain  $Q \approx 11$ and
$Q \approx 11$ and  $P_{\textrm {fusion}} \approx 140$ MW. SPARC will therefore constitute a unique platform for burning plasma physics research with high density (
$P_{\textrm {fusion}} \approx 140$ MW. SPARC will therefore constitute a unique platform for burning plasma physics research with high density ( $\langle n_{e} \rangle \approx 3 \times 10^{20}\ \textrm {m}^{-3}$), high temperature (
$\langle n_{e} \rangle \approx 3 \times 10^{20}\ \textrm {m}^{-3}$), high temperature ( $\langle T_e \rangle \approx 7$ keV) and high power density (
$\langle T_e \rangle \approx 7$ keV) and high power density ( $P_{\textrm {fusion}}/V_{\textrm {plasma}} \approx 7\ \textrm {MW}\,\textrm {m}^{-3}$) relevant to fusion power plants. SPARC's place in the path to commercial fusion energy, its parameters and the current status of SPARC design work are presented. This work also describes the basis for global performance projections and summarizes some of the physics analysis that is presented in greater detail in the companion articles of this collection.
$P_{\textrm {fusion}}/V_{\textrm {plasma}} \approx 7\ \textrm {MW}\,\textrm {m}^{-3}$) relevant to fusion power plants. SPARC's place in the path to commercial fusion energy, its parameters and the current status of SPARC design work are presented. This work also describes the basis for global performance projections and summarizes some of the physics analysis that is presented in greater detail in the companion articles of this collection.

