Refine listing
Actions for selected content:
142351 results in Open Access
Exhalation
-
- Journal:
- Palliative & Supportive Care / Volume 22 / Issue 5 / October 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. 1533
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Community-associated Carbapenem-Resistant Organism Case Investigations in New York City, December 2020-May 2023
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s147
-
- Article
-
- You have access
- Open access
- Export citation
Assessing chlorhexidine resistance in MRSA isolates from hospitals in Cleveland, OH and Detroit, MI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s114
-
- Article
-
- You have access
- Open access
- Export citation
Trends in Hospital Antibacterial Consumption in Belgium (2017-2021): Evaluating the Impact of the COVID-19 Pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s149-s150
-
- Article
-
- You have access
- Open access
- Export citation
-
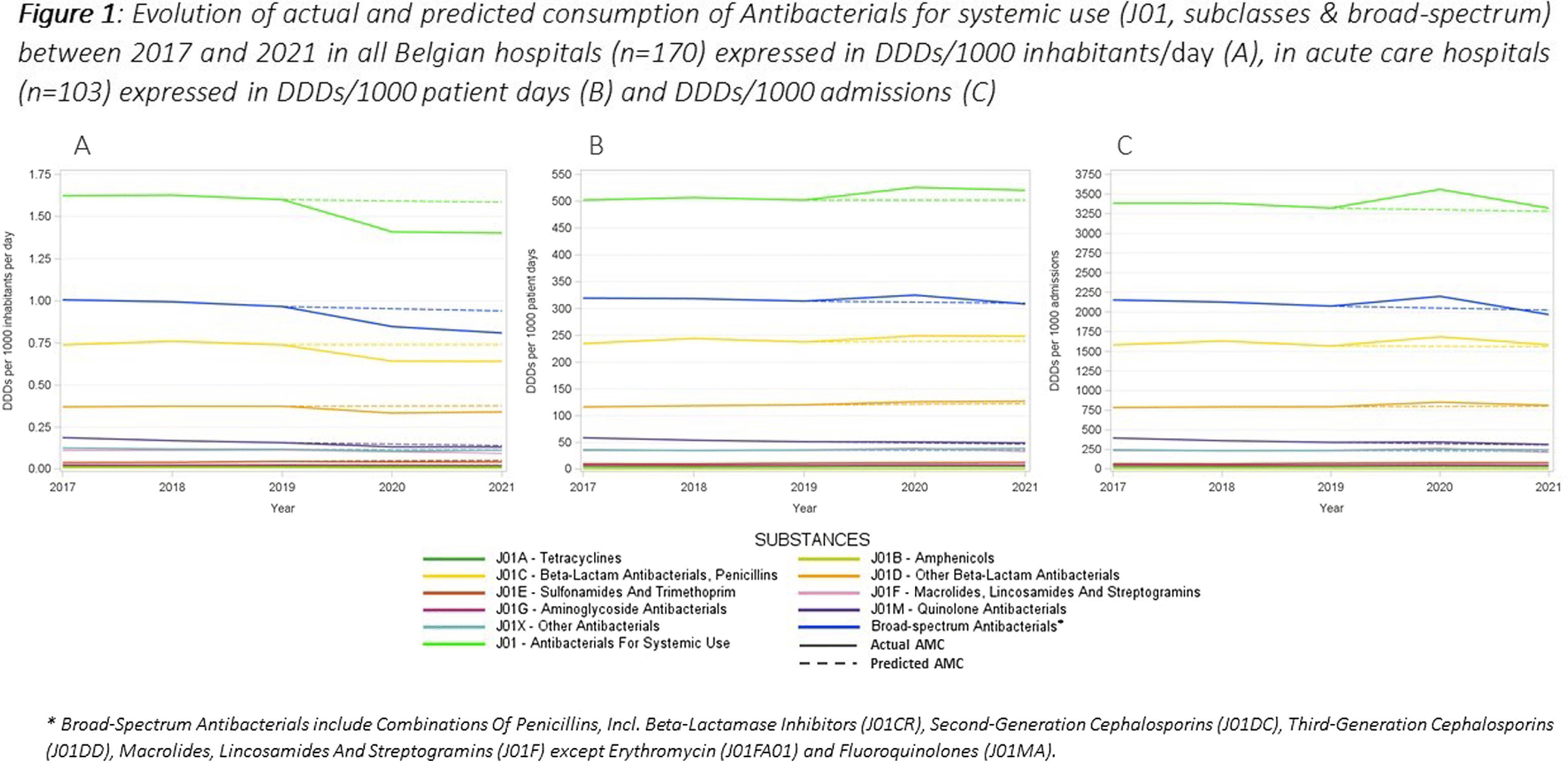
This study aimed to evaluate the impact of the COVID-19 pandemic on antimicrobial consumption (AMC) in Belgian hospitals from 2017 to 2021, using data from the European Surveillance of Antimicrobial Consumption Network (ESAC-Net) and the Belgian Hospitals Surveillance of Antimicrobial Consumption (BeH-SAC). Antimicrobial volume was quantified in Defined Daily Doses (DDDs), and AMC was expressed in DDDs/1000 inhabitants/day (DIDs), DDDs/1000 patient days and DDDs/1000 admissions. Linear regressions were employed to analyze 5-year trends for the ATC J01 group, at the ATC-3 level and for broad-spectrum antimicrobials. Broad-spectrum antibiotics included combinations of penicillins, incl. beta-lactamase inhibitors (J01CR), second-generation cephalosporins (J01DC), third-generation cephalosporins (J01DD), macrolides, lincosamides and streptogramins (J01F, excluding erythromycin J01FA01), and fluoroquinolones (J01MA). The compound annual growth rate (CAGR) calculated for the years preceding the pandemic was used to forecast 2020 and 2021 AMC, enabling a comparison with the actual use. Hospital AMC measured as DIDs decreased by 12% from 2019 to 2020. In contrast, when expressed as DDDs/1000 patient days and DDDs/1000 admissions, a 5% and 7% increase was observed, respectively. Antibacterials for systemic use (J01) showed a significant decrease over the 5 years only when expressed in DIDs. Notable trends included a negative trend for quinolone antibacterials (J01M) when expressed in the three incidence units, as for amphenicols (J01B) when using hospital denominators only. Positive trends were observed for sulfonamides and trimethoprim (J01E) using hospital denominators and for other beta-lactam antibacterials (J01D) with the ‘patient days’ denominator. While the consumption of all J01 antimicrobial subclasses deviated negatively from predicted use both in 2020 and 2021 when expressed in DIDs, positive deviations were recorded using hospital denominators, except for macrolides (J01F). The use of broad-spectrum antimicrobials showed a notable decrease between 2017 and 2021 when expressed in DIDs. However, when using hospital denominators, the observed use of broad-spectrum antimicrobials exceeded the forecasted values in 2020, to regress below the forecasted levels in 2021 (Figure 1). Contrary to results obtained using the widely applied country’s population as the denominator, a notable surge in AMC, particularly for broad-spectrum antimicrobials, was observed in 2020 when using hospital-specific denominators. This increase coincided with the onset of the COVID-19 crisis. These findings emphasize the need for a national hospital surveillance system that uses denominators that accurately represent the specific population being monitored. Implementing robust hospital-specific surveillance mechanisms would improve the precision of evaluations and facilitate targeted interventions aimed at optimizing antimicrobial utilization.

Assessing the quality of Hand Hygiene data produced by Alberta Health Services using a time-in-motion study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s100
-
- Article
-
- You have access
- Open access
- Export citation
Underlying Conditions in Community-associated Clostridioides difficile Infections in Davidson County, Tennessee
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s65
-
- Article
-
- You have access
- Open access
- Export citation
The Impact of COVID-19 on Healthcare-Associated Infections: A Survey of Acute Care Hospitals
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s11-s12
-
- Article
-
- You have access
- Open access
- Export citation
-
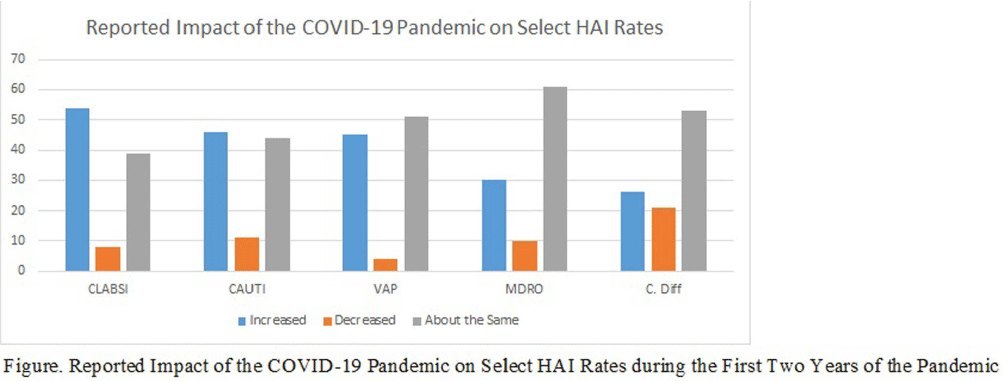
Background: The COVID-19 pandemic has placed an enormous strain on the healthcare system, including infection prevention and control. The response to the COVID-19 pandemic required extraordinary resources, which were often diverted from routine infection prevention and control activities and may have contributed to increased rates of HAI in the acute care setting. However, the impact of the COVID-19 pandemic on infection prevention and control departments, including staffing and resources, and on routine infection prevention and control activities is not well-described. The objective of this study was to describe the impact of the COVID-19 pandemic on IPC departments and department response to the pandemic. Methods: Between August and December of 2023, we conducted an electronic survey of all acute care facilities participating in the National Healthcare Safety Network. Survey data were analyzed using descriptive statistics. Results: Over 594 infection control departments participated in the survey, representing 1,400 NHSN facilities (20% response rate based on number of eligible NHSN facilities). Half of the respondents reported that their hospital experienced increases in the following HAI rates during the first two years of the pandemic: central-line associated bloodstream infections (54%), catheter-associated urinary tract infections (46%) and ventilator associated pneumonia (45%). When asked to identify the top three contributors to increased HAI rates in their facility, respondents cited the following factors: staffing shortages (70%), patient acuity (69%), use of travel nurses (48%), increased device utilization (37%), and reduced bedside acuity (31%). Respondents reported that their department utilized the following actions to decrease these HAI rates: increased rounding and monitoring of IPC procedures (81%), reeducation of frontline staff on IPC policies and procedures (77%), environmental care rounds (69%), monitoring of isolation compliance (66%), HAI Task Force/Committee (57%), nurse-driven catheter removal protocols (53%), and insertion prevention protocols (53%). When asked if the department experienced applied pressure or attempts to influence HAI reporting due to the increase in HAI rates in the facility experienced in the wake of the pandemic, 19% of respondents reported increased pressure from management/C-suite and 7% reported increased pressure from providers. Conclusion: The COVID-19 pandemic had a substantial impact on IPC departments in acute care hospitals and had a profound effect on IPC staffing, resources and routine IPC activities. Future work needs to identify best practices and lessons learned from the pandemic to inform future pandemic preparedness.

The Next Target for Readmission Reporting? Exploring Readmission Rates of Patients with CLABSI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s71
-
- Article
-
- You have access
- Open access
- Export citation
Epidemiology of Extrapulmonary Nontuberculous Mycobacterial Disease – 4 Emerging Infection Program Sites, 2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s90-s91
-
- Article
-
- You have access
- Open access
- Export citation
-
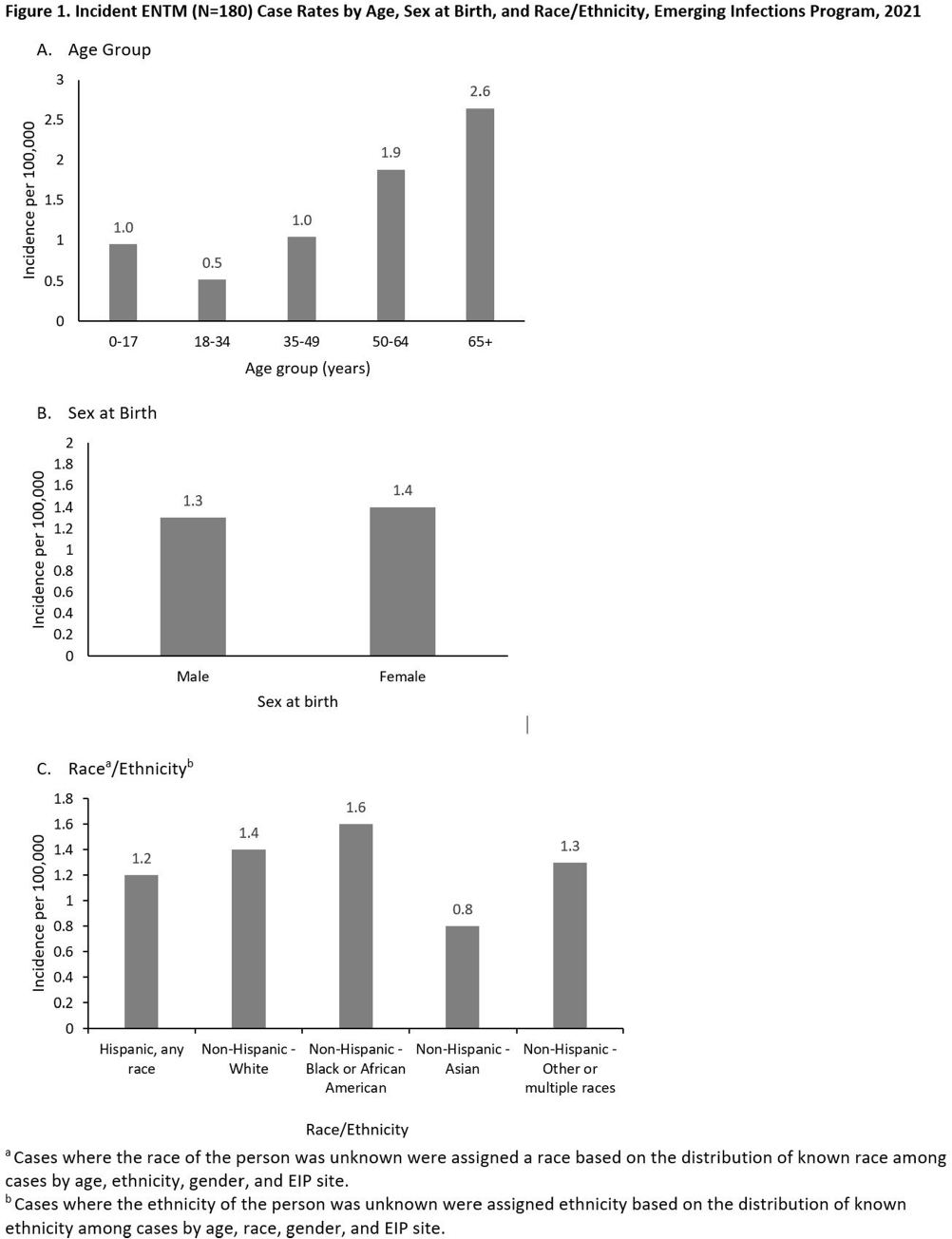
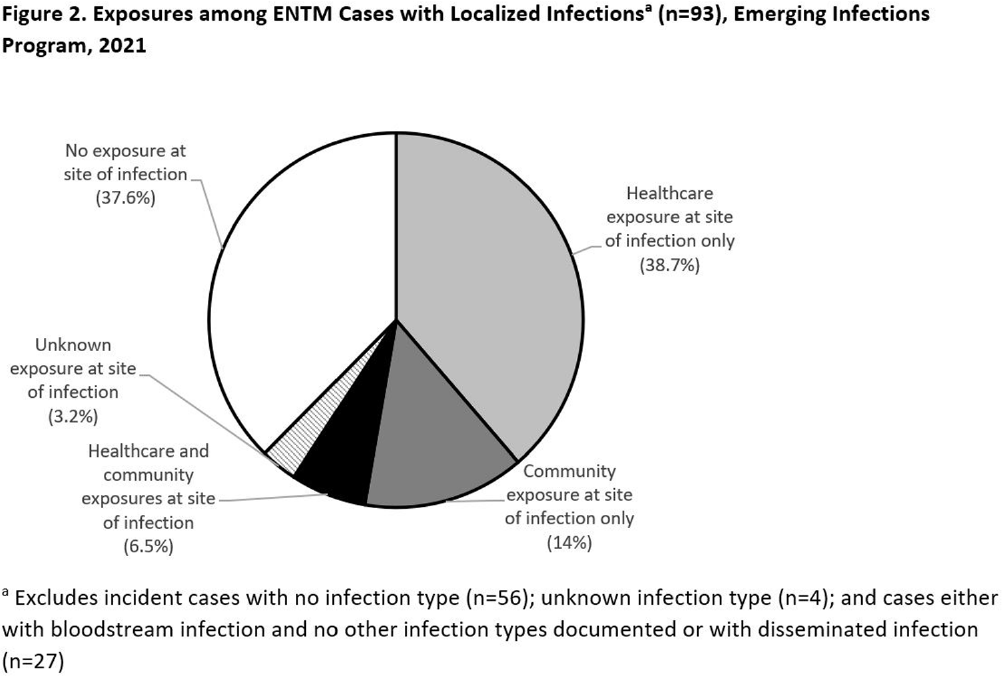
Background: Extrapulmonary nontuberculous mycobacteria (ENTM) infections are difficult to treat and often require prolonged therapy or surgery. Few population-based studies describe ENTM epidemiology, though well-known healthcare-associated outbreaks have occurred. Using the first year of multi-site ENTM surveillance, we characterized rates and how frequently ENTM infections may be related to healthcare. Methods: CDC’s Emerging Infections Program conducted active, laboratory- and population-based surveillance for ENTM cases in 4 sites (Colorado [5 counties], Minnesota [statewide], New York [1 county], and Oregon [statewide]) in 2021. An incident ENTM case was NTM isolation from a non-pulmonary specimen, excluding stool or rectal swabs, in a resident of the surveillance area without either medical record documentation of prior ENTM infection or isolation of ENTM in the prior 12 months. Demographic, clinical, information on selected healthcare and community exposures, and laboratory data were collected via medical record review. We calculated incidence per 100,000 population using U.S. Census population estimates and performed descriptive analyses. Results: A total of 180 incident ENTM cases were reported in 2021. The crude annual incidence rate was 1.3 per 100,000 persons. Incidence increased with age (from 0.95 per 100,000 among 0–17 year-olds to 2.65 per 100,000 among persons ≥65), ranged from 0.8 among non-Hispanic Asian persons to 1.6 per 100,000 in non-Hispanic Black persons, and was similar among males (1.3 per 100,000) and females (1.4 per 100,000; Figure 1). Mycobacterium avium complex (64 [35.6%]) was the most frequently isolated species group, followed by Mycobacterium chelonae complex (31 [17.2%]). Skin and soft tissue infections were the most frequent infection type (37 [20.6%]); 27 cases (15.0%) were associated with disseminated and/or only bloodstream infection, and 56 cases (31.1%) had no infection type documented. Among 93 cases with localized ENTM infections (i.e., infections that were not disseminated and/or only bloodstream infections), 38.7% had only healthcare-related exposures, 14% had only community-related exposures and 6.5% had both exposure types at the site of infection (Figure 2). Healthcare-related exposures at the infection site included surgery (23.7%), injection/infusion (21.5%), and medical devices (18.3%). The most frequent community-related exposure at the infection site was trauma (17.2%). Only one case was part of a known outbreak, which was healthcare-associated. Conclusions: ENTM infections are relatively rare, but nearly half of patients with localized ENTM infections had prior healthcare-related exposures. This indicates that the burden of ENTM infections related to healthcare may be much larger than what has been suggested from reported outbreaks.


Quantity versus Quality: Chlorhexidine Bathing Adequacy Assessments in 3 High-Risk Units
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s30
-
- Article
-
- You have access
- Open access
- Export citation
Investigation of Healthcare-Associated Infection Risks from Ice: Summary of CDC Consultations 2016-2023
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s29
-
- Article
-
- You have access
- Open access
- Export citation
Antibiotic Prescribing Practices on Hospital Discharge for Management of Urinary Tract Infections: A Single Center Study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s36-s37
-
- Article
-
- You have access
- Open access
- Export citation
-
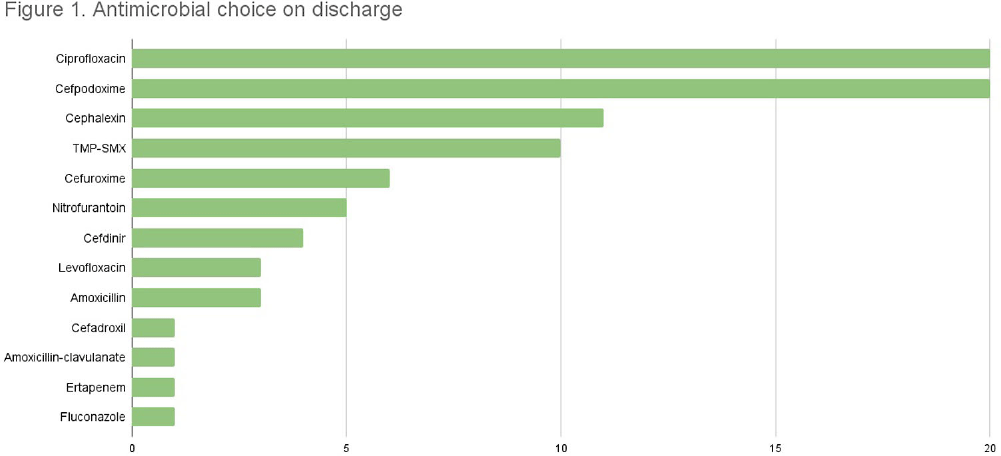
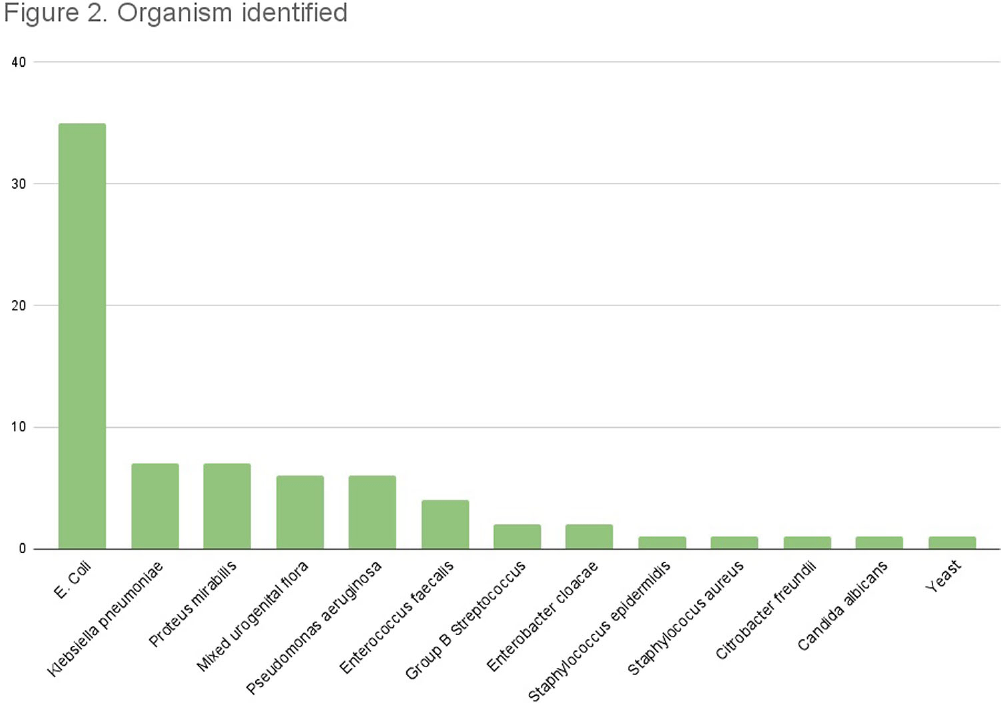
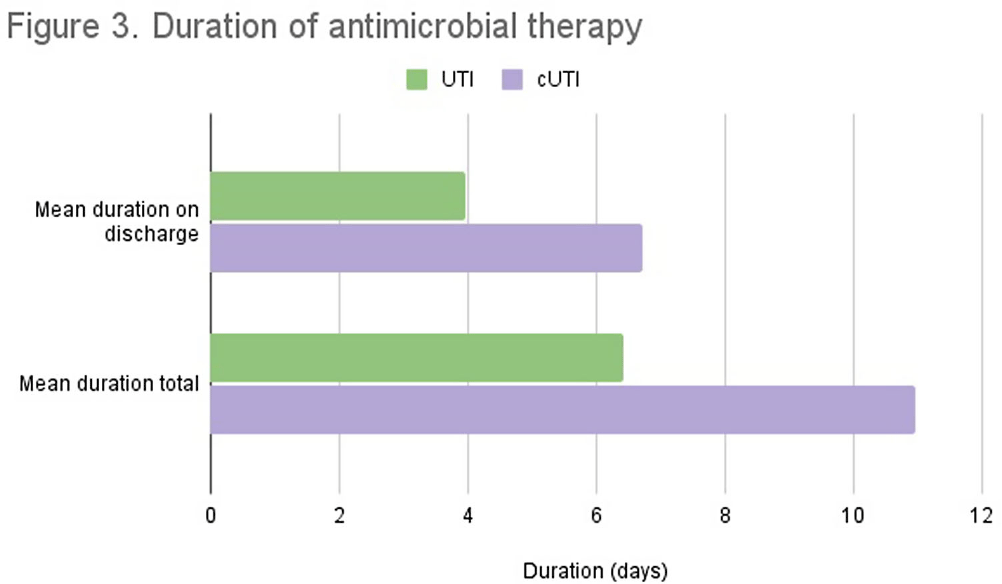
Background: Appropriate antibiotic use has been described as one of the key strategies in tackling antibiotic resistance. Although the majority of antimicrobial therapy is completed following discharge, there lacks clear guidance in addressing antibiotic stewardship in the outpatient setting. Particularly, broader coverage as well as longer durations of therapy are often encountered following hospitalization. In our study we examine the various antibiotic prescribing practices on hospital discharge for management of urinary tract infections (UTI). Methods: We conducted a single-center, retrospective observational chart review of patients discharged from St. Francis Hospital and Medical Center in Hartford between May and July 2022. Medical records were reviewed for patients who were prescribed antibiotic therapy for management of UTI and met inclusion criteria. Variables of interest included type of UTI treated, antibiotic used, duration of antibiotics during and following hospitalization, fluoroquinolone use, as well reported adverse events. Total duration of therapy was defined as days on susceptible antimicrobials with appropriate source control. Results: A total of 84 patients met inclusion criteria. 44 received treatment for simple UTI (sUTI) and 40 for complicated UTI (cUTI). Figure 1 shows the various organisms identified on culture. The most common antimicrobials prescribed on discharge were cefpodoxime and ciprofloxacin [figure 2]. Quinolones were prescribed in 11.4% of sUTIs and 39.1% of cUTIs on hospital discharge. Of those, only one patient had no alternative to quinolone use due to drug allergies. The mean duration of therapy for treatment of sUTI was 6.4 days total (SD 2.40) with 3.9 days outpatient (SD 1.78). The mean duration of therapy for treatment of cUTI was 10.9 days total (SD 3.62) with 6.7 days outpatient (SD 2.99). Comparison of mean durations is shown in figure 3. In 49% of all cases (including both sUTI and cUTI) patients received greater than 7 days of antimicrobial therapy. Conclusion: There is increased evidence favoring shorter courses of antimicrobial therapy for management of both simple and complicated UTIs. A 7-day course has been shown as effective duration of therapy for cUTI with appropriate source control, regardless of presence of bacteremia. Results from our single center-study show both sUTI and cUTI are subject to unnecessarily prolonged durations of therapy on hospital discharge. In addition we noted a significant use of fluoroquinolones in cUTI treatment. We believe stewardship interventions at time of discharge may particularly benefit shorter courses of therapy for cUTI as well as reduced quinolone use.



The Difference We Make at Home: Impact of Infection Prevention and Control in Pediatric Homecare Tracheitis Reduction
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s130
-
- Article
-
- You have access
- Open access
- Export citation
-
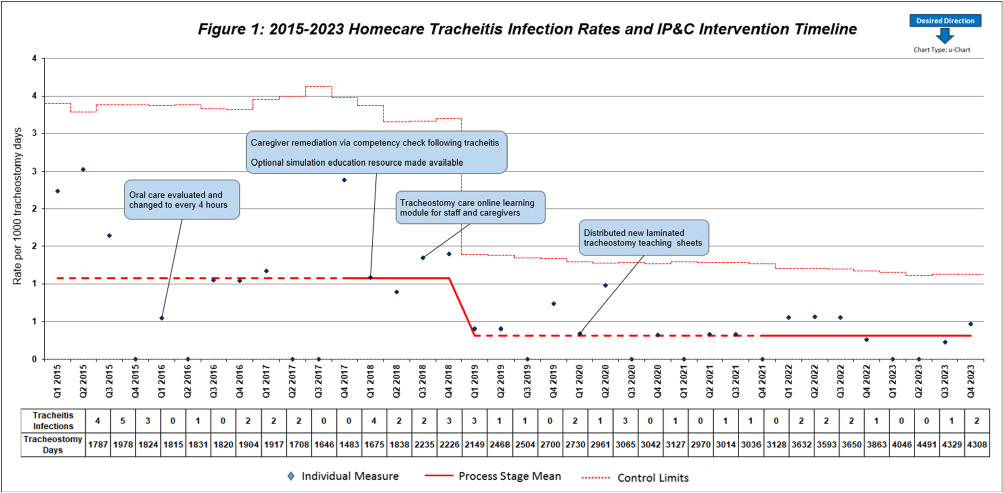
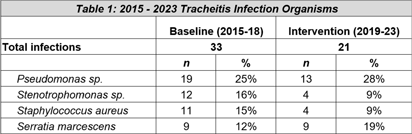
Background: Quality improvement (QI) efforts within Infection prevention and control (IP&C) programs to reduce risk of device-related infections in the acute care setting are well described. However, less focus has been placed on continued prevention in the homecare setting. This QI project illustrates the benefits of IP&C involvement in reducing tracheitis in pediatric homecare patients. Methods: The homecare multidisciplinary IP&C team implemented a series of QI initiatives aimed at reducing incidence of tracheitis beginning in 2016. Initial interventions included increasing oral care frequency to every four hours, inpatient training for new tracheostomy patients and families before discharge, and an optional inpatient simulation training resource to provide hands-on practice. Enhanced educational interventions included caregiver learning modules and competencies completed with their primary nurse in the home every ninety days and following a tracheitis infection. Practice changes and education efforts were further sustained with the creation and distribution of laminated tracheostomy care teaching sheets to patient homes. Quarterly tracheitis infection rates were tracked using a U-chart. Organism distribution in tracheitis cases were compared across the baseline (2015-2018) and post-intervention periods (2019-2023) using the Chi square test. Analyses were performed using Stata Statistical Software: Release 18 (College Station, TX: StataCorp, LLC) with two-tailed alpha level of 0.05. Results: Quarterly tracheitis infection rates from 2015 through 2023 are displayed in the Figure. Notably, the baseline period, established Q1 2015 through Q4 2017, revealed a consistent rate of 1.08 tracheitis infections per 1000 tracheostomy days. During this initial phase, changes in oral care frequency and enhanced educational resources were implemented to decrease rates. Following these interventions, a significant shift was observed in Q1 2019, with the new baseline rate drastically reduced to 0.32 infections per 1000 tracheostomy days. This denotes a remarkable 70% improvement from the prior average infection rate which has been sustained through Q4 2023 with the laminated teaching sheets. The most frequently identified organisms across both time periods are displayed in the Table. Pathogen distribution was similar following QI interventions (p = 0.50). Conclusions: Tracheitis infections were reduced by 70% through implementation of multidisciplinary homecare IP&C QI efforts. IP&C programs are integral to pediatric homecare.


Antimicrobial use among under-five hospitalized children in Bangladesh: Findings from a Point Prevalence Survey
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s50
-
- Article
-
- You have access
- Open access
- Export citation
Mitigating SSIs: focus on physical operation rooms environmental factors
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s96-s97
-
- Article
-
- You have access
- Open access
- Export citation
Intervention Targets to Optimize Antibiotic Prescribing on Discharge from the Hospital to Nursing Homes
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s23
-
- Article
-
- You have access
- Open access
- Export citation
Nevertheless
-
- Journal:
- Palliative & Supportive Care / Volume 22 / Issue 6 / December 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. 2247
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Inpatient clinicians’ approach to diagnosis of urinary tract infections in older adults using the COM-B model: a qualitative assessment
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e134
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Mentoring up: How mentorship training influences mentee intent to change behavior
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e119
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Whole Genome Sequencing for the Identification of a Streptococcus agalactiae Outbreak in Neonatal Intensive Care Unit
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s124-s125
-
- Article
-
- You have access
- Open access
- Export citation
-
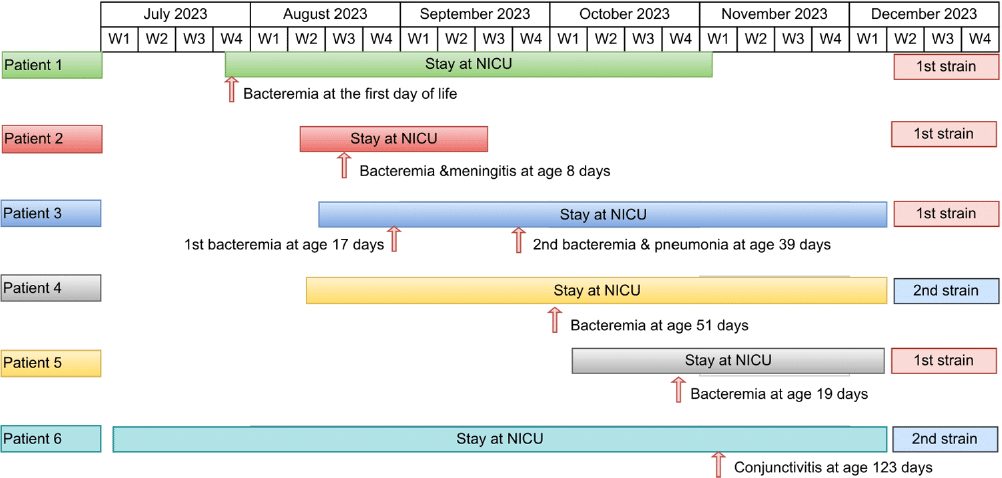
Background: While Streptococcus agalactiae (Group B Streptococcus [GBS]) infections in infants usually result from maternal transmission, healthcare-associated cases, particularly in the neonatal intensive care unit (NICU), can occur. Whole genome sequencing (WGS) can aid in investigating GBS outbreaks among infants in hospital settings. The aim of the study is to describe the investigation of GBS infections in NICU using WGS. Methods: Infection prevention and control (IPAC) at our hospital monitors the occurrence of late-onset GBS disease (LOD) in our 57-bed NICU, which consists of all private rooms. The occurrence of 2 cases of LOD within 2 weeks triggered an investigation, including WGS of the two isolates and isolates causing invasive GBS during the last 6 months in the unit. GBS isolates underwent WGS using Illumina at Canada’s National Microbiology Laboratory. All affected patients underwent chart-review. Outbreak description and investigation: In August 2023, two NICU neonates (patients 2,3) experienced LOD two weeks apart, one with bacteremic meningitis and the other with two bacteremic episodes three weeks apart. While WGS was pending two additional cases of late-onset GBS bacteremia (patients 4,5) occurred. Isolates from Pts 2,3 and 5 were indistinguishable from each other and from an isolate from an infant admitted to the NICU with early onset bacteremia on July 27, 2023 (day 1 of life) (patient 1). Weekly point prevalence for throat and rectal colonization over 3 weeks identified five infants colonized with unrelated strains. An additional long-stay infant (patient 6) developed GBS conjunctivitis due to a strain indistinguishable from (patient 4) by pulse field gel electrophoresis, WGS for the second cluster is pending. IPAC interventions: Lapses in IPAC practices were observed, with no commonalities among cases other than similar geographic location within the unit. We hypothesized transmission was due to horizontal transmission between babies due to these lapses. Basic IPAC measures, including hand hygiene and environmental cleaning, were reinforced; Additional Precautions were not used due to private rooms’ unit structure. No environmental samples were taken due to lack of an obvious environmental point or common source. Point prevalence monitoring persisted until no new cases related to the outbreak strains were further identified in three consecutive weekly point prevalence. Conclusions: Increased awareness of healthcare-associated transmission is crucial in NICU as LOD GBS emerges. WGS plays a key role in identifying transmission. Detecting a multi-strain outbreak can appropriately redirect investigations. Legend: Figure 1: Timeline of stay at NICU and infection timing for patients 1-6