Refine listing
Actions for selected content:
142351 results in Open Access
Empowering Patient Hand Hygiene and Reducing Infection in the Oncology Population
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s102
-
- Article
-
- You have access
- Open access
- Export citation
-
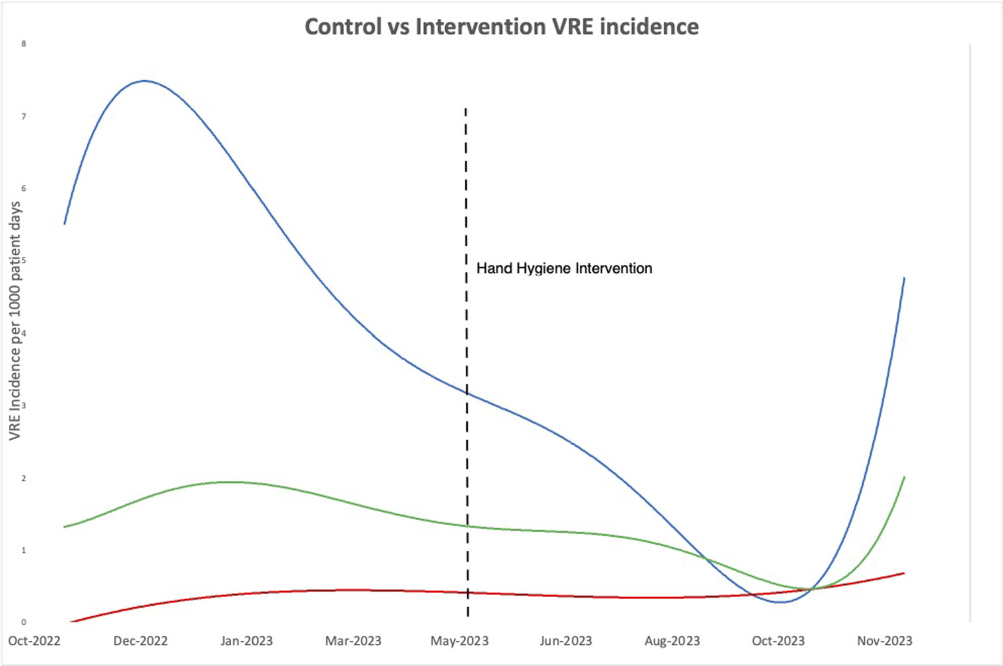
Background: Significant focus has been placed on healthcare worker hand hygiene, but little attention is has been assigned to the role of patient hand hygiene (HH) in reducing hospital acquired infections. Therefore, in this quality improvement study, we examined the impact of providing patients with hand hygiene products around mealtime on increasing patient HH adherence and on reducing acquisition of nosocomial antibiotic resistant organisms. Methods: Patients on two inpatient leukemia units at a tertiary oncologic center were provided with a single use pre-packaged alcohol wipe on their meal trays prior to every meal (three times daily). Additionally, an information card explaining to patients how and when to use the alcohol wipe was provided on the meal trays three times a week. Both the wipe and instructions were designed with input from patient representatives at the hospital. Two oncologic control units were selected where no specific intervention for patient hand hygiene was conducted. Patient hand hygiene adherence on the control and intervention units were measured through once monthly patient interviews conducted after meals where patients were asked to recall whether they washed their hands prior to eating (using any product). Vancomycin Resistant Enterococcus (VRE) incidence was compared on the intervention and control units during the 7 months prior and 7 months following initiating the intervention. Results: During the seven-month intervention period, more than 15 000 wipes were dispensed to patients on the intervention units. Through interview, 91% of 87 patients on the intervention units reported cleaning their hands before eating a meal using any cleaning product compared to 72% of 68 patients on the control units (X2 = 9.32, p = 0.002). Furthermore, on the intervention units, 30 (38%) patients endorsed using the provided hand hygiene product. During intervention period, the combined incidence rate of VRE the intervention units was 1.85 case/1000 patient-days compared to 5.35 cases/1000 patient-days during the 7 months prior to intervention (t = 3.24, p=0.007)(Figure 1). Conclusions: This patient-centered quality improvement intervention increased patient hand hygiene and potentially reduced VRE incidence in a vulnerable oncologic population. This practical intervention that incorporated the patient perspective provided accessible hand hygiene products with simple instruction and reminders required minimal participation of unit staff. Further application of the intervention in non-oncologic populations is needed to further establish the relationship between patient hand hygiene and the acquisition of nosocomial infections.

Two Novel Antibiotic Use Metrics for Facilities and Individual Prescribers in Post-Acute and Long-Term Care Settings
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s25-s26
-
- Article
-
- You have access
- Open access
- Export citation
-
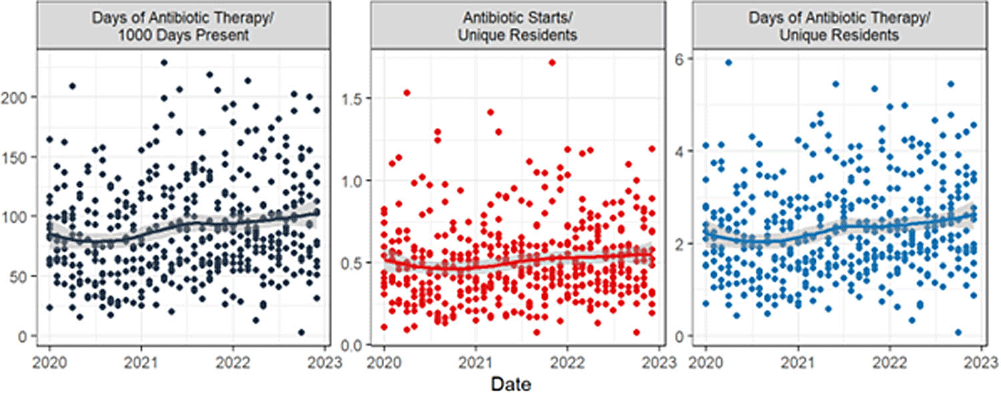
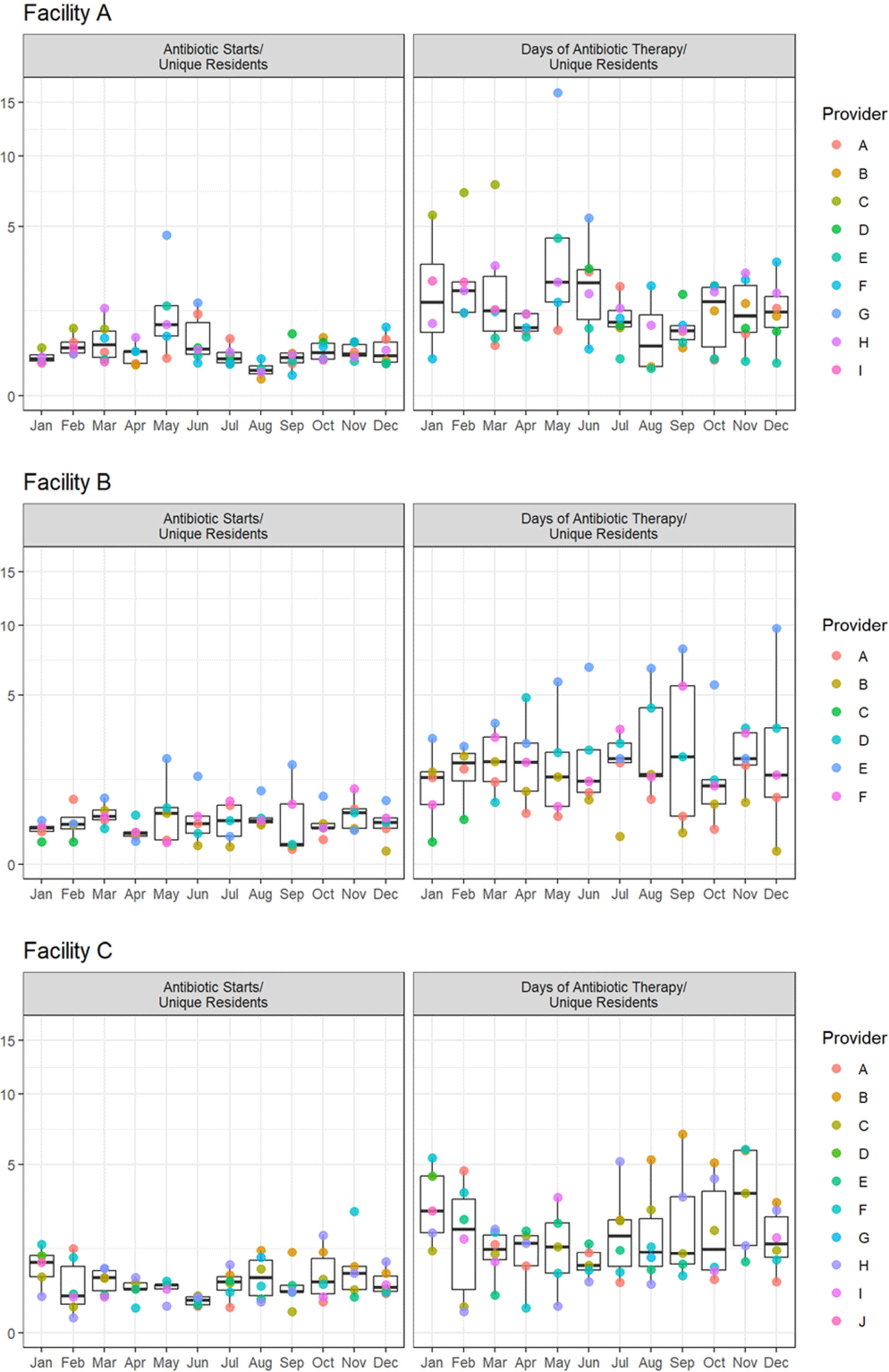
Background: Measuring and reporting antibiotic use are essential to antimicrobial stewardship activities. The most common metric to assess facility-level use is days of antibiotic therapy per 1000 days of care (DOT/1000 DOC). This metric may be difficult to calculate, not be readily comparable, or not provide actionable data to individual prescribers, particularly those that work in post-acute and long-term care (PALTC) settings. Here we use data from a centralized dispensing pharmacy to develop antibiotic use metrics suitable for offering individualized feedback to prescribers working in PALTC settings. Methods: We obtained medication dispensing data and resident census data for 13 PALTC settings within the same network. After omitting non-pharmacologic items and limiting the data to medications dispensed from 1/2020 – 12/2022, we determined the following metrics by month: days of antibiotic therapy (DOT), number of medications prescribed, number of antibiotic courses prescribed (antibiotic starts), and the number of individual residents issued a prescription for any medication (unique residents). These metrics were assessed for each facility (2020 – 2022) and for prescribers responsible for > 1% of prescriptions within that facility (2022 only). Prescriber-level unique residents was the number of residents issued a prescription by the given provider. We obtained facility-level census data to calculate antibiotic DOT/1000 resident days of care (DOC) as a standard to which we compared novel metrics. Results: During the 3-year study period, 1718 prescribers at 13 PALTC settings wrote for 672256 medications, including 31087 antibiotic courses. At the facility level, the correlation between monthly antibiotic starts (courses)/unique residents and antibiotic DOT/1000 DOC was 0.83 (p < 0 .0001). The correlation between monthly antibiotic DOT/unique residents and antibiotic DOT/1000 DOC was 0.98 (p < 0 .0001). Trends in monthly values of both novel metrics and DOT/1000 DOC were consistent across the examined period (Figure 1). For individual prescribers, both novel metrics permit assessment and comparison of antibiotic prescription rates over time (Figure 2). Conclusions: Pharmacy dispensing data can be used to determine antibiotic DOT/unique residents and antibiotic starts/unique residents at the facility level and for individual providers. The novel metric antibiotic DOT/unique residents demonstrated strong correlation with antibiotic DOT/1000 DOC at the facility level. In addition to supporting tracking and reporting of antibiotic use among PALTC settings, these new metrics permit visualization of the antibiotic prescribing rates of individuals prescribers, as well as peer comparison, which in turn can lead to actionable feedback that helps improve antibiotic use in the care of PALTC.


A Machine Learning Exploration of Social Determinants of Health and Hospital-Onset Bacteremia, Northern California, 2019–2023
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s132-s133
-
- Article
-
- You have access
- Open access
- Export citation
-
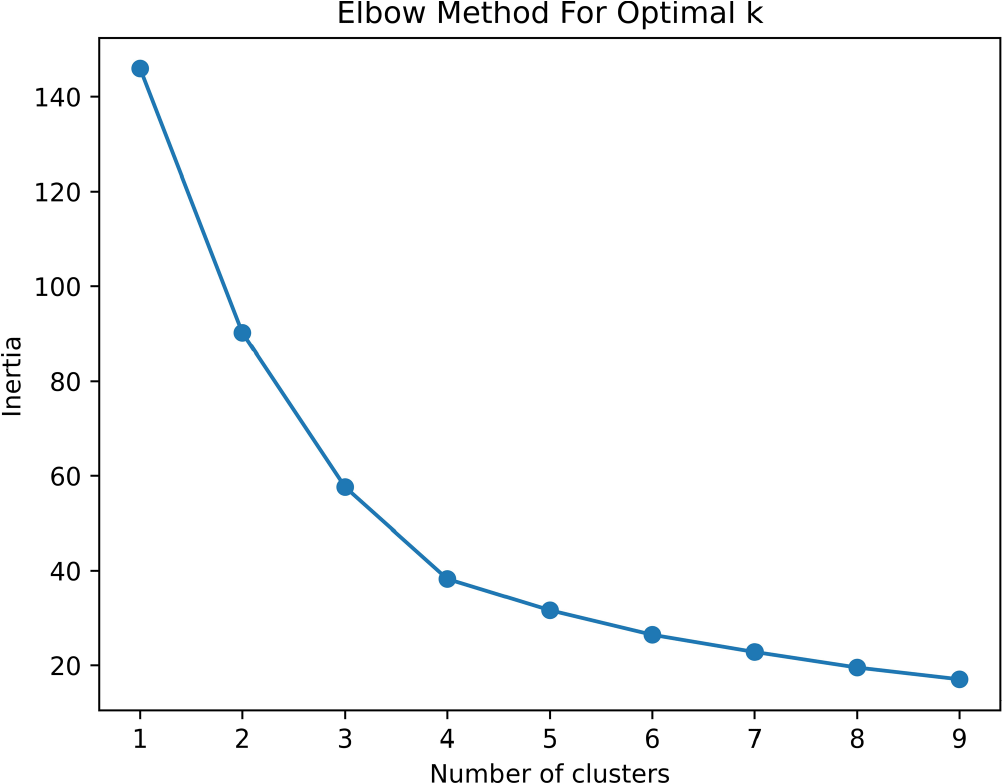
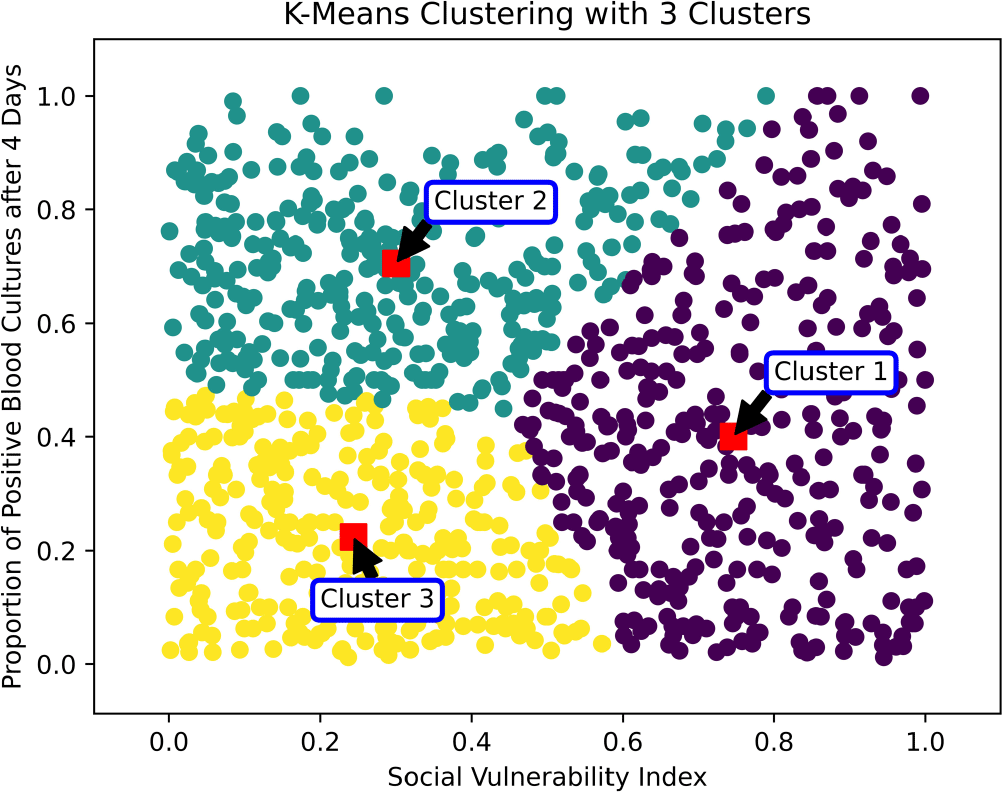
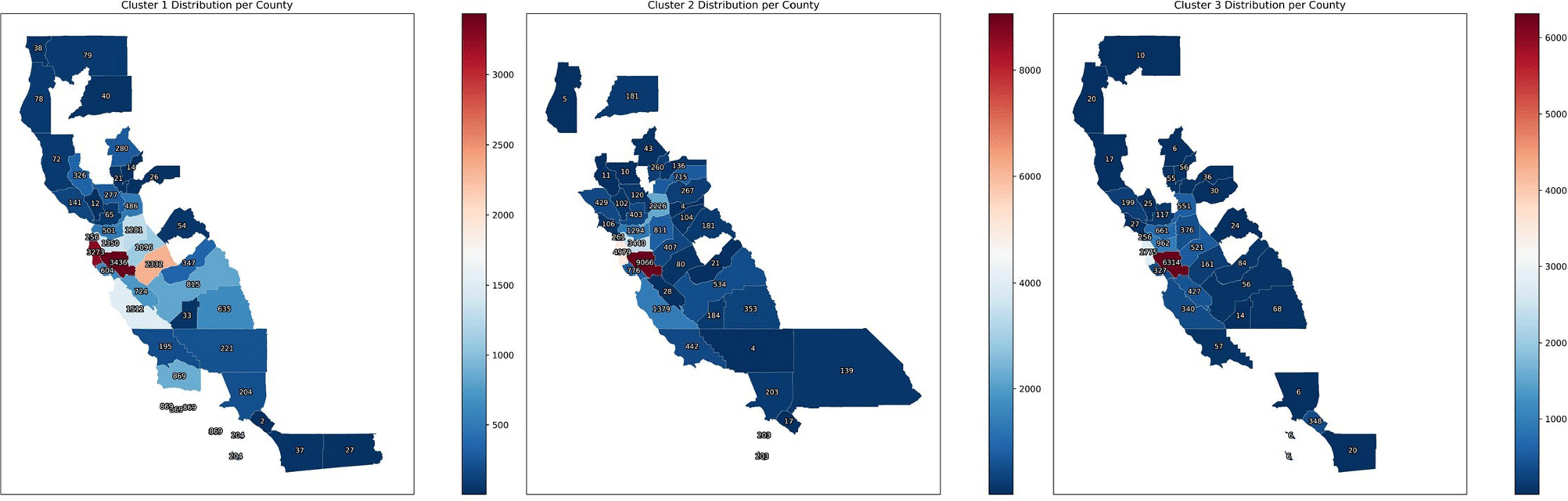
Introduction: Social determinants of health can impact healthcare-associated infections. Hospital-onset bacteremia (HOB) may lead to poor outcomes, increased length of stay, and increased cost of care. We explored the association of social determinants of health and HOB. Methods: We retrieved blood culture data at Stanford Health Care from May 2019 to October 2023. We identified blood cultures ordered ≥4 days of admission. To evaluate the association between social determinants of health and HOB, we employed an unsupervised machine learning approach (K-Means clustering) to discern patterns in HOB rates based on the Social Vulnerability Index (SVI). The SVI indicates the relative vulnerability of every U.S. Census tract. It ranks the tracts on 16 measures of vulnerability across 4 themes: socioeconomic factors, household characteristics, racial and ethnic minority status, and housing/transportation aspects. The number of clusters was determined using the Elbow Method (Figure 1). Results: Out of 209,947 blood cultures from 23,938 unique patients with a California address, we identified 81,653 blood cultures collected after 4 days (40%). The K-Means clustering algorithm identified 3 distinct clusters within the Californian census tracts, suggesting heterogeneity in the relationship between SVI and HOB (Figure 2). Cluster 1 had a higher SVI (median 0.73, range 0.46 – 0.99), with logistic regression indicating a positive SVI-HOB association (OR 4.84, 95% CI 4.02 – 4.81, p <.001). Cluster 2, had a median SVI of 0.29 (range 0.0009 – 0.78), also showed a positive association between SVI and HOB (OR 1.67, 95% CI 1.4 – 1.89, p <.001), aligning with trends of higher infection risks in more vulnerable groups. In contrast, Cluster 3 had a median SVI of 0.22 (range 0.002 –0.84). In this cluster, the SVI showed a negative association with HOB (OR 0.24, 95% CI 0.18 – 0.31, p <.001). Cluster 3 was the cluster with the least number of subjects (15,000, versus 21,761 for Cluster 1 and 29,762 for Cluster 2). Most subjects in Cluster 3 resided in Santa Clara County, whereas those in Clusters 1 and 2 were spread across Santa Clara, San Mateo, Alameda, Merced, and Sacramento Counties (Figure 3). Conclusions: Advanced techniques can be used to explore the complex interplay between social determinants of health and healthcare-associated infections and could guide the development of community-specific strategies to improve outcomes.



Immediate Use Steam Sterilization and the Effect on Surgical Site Infections in an Acute Care Facility
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s143
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Immediate use steam sterilization (IUSS) shortens the time from sterilization to the aseptic transfer onto the surgical sterile field. Published data incompletely defines the extent to which IUSS increases risk of surgical site infection (SSI), compared to standard sterile reprocessing methods. We aimed to measure the association between IUSS use for surgical instrument reprocessing and SSI risk in a facility where IUSS use increased due to staffing constraints and case volumes. Methods: In this retrospective observational study at a tertiary care hospital with a diverse mix of surgery types, we used sterile reprocessing logs and SSI outcomes defined using National Health and Safety Network definitions to compare SSI rates among surgeries using surgical devices sterilized using IUSS compared to standard terminal sterilization methods. We calculated a risk ratio (RR) and 95% confidence interval (95%CI), including stratification by eleven high-volume service lines. Results: Among 23,919 surgical procedures, 416 (1.74%) developed SSIs. IUSS was used to sterilize instruments prior to 1,524 (6.37%) surgical procedures, and of these procedures 39 (2.56%) developed an SSI, compared to 1.68% of non-IUSS procedures (377 SSI in 22,395 procedures; risk ratio [RR] 1.52, 95% confidence interval [95%CI] 1.10-2.11). Two surgical services had statistically significant RRs for SSI development after IUSS: transplant surgery (RR 2.47, 95%CI 1.32-4.60] and plastic surgery (RR 3.64, 95%CI 1.13-11.74; Figure). Conclusion: IUSS is associated with a significant increase in SSIs, including among varied surgery types. IUSS utilization should be minimized.


Patient and Community Perspectives on Antibiotics and Antimicrobial Resistance: Fertile Grounds for Antimicrobial Stewardship
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s41-s42
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Antimicrobial resistance is a serious public health threat. Overuse of antibiotics leads to the development and spread of antibiotic resistant pathogens. Antibiotics are also responsible for a high percentage of emergency department visits for adverse drug events. Despite this, ambulatory and urgent care providers often cite patient expectations as a reason for inappropriate antibiotic prescribing practices. We investigated patient and community understanding of antibiotics and antimicrobial resistance to inform how they can be engaged as partners in combating antimicrobial resistance in our southwestern Virginia community. Methods: From July to September 2023, we conducted an online survey of patients and community members within the footprint of a large healthcare system in Southwest Virginia. Electronic medical records were used to randomly select and directly email the survey link to a representative sample of ambulatory patients who met criteria. Respondents were also recruited through the health system’s social media channels and through posters with quick response (QR) codes in outpatient offices. The survey used Likert scales and multiple-choice questions to understand experiences with and perceptions about antibiotics and antimicrobial resistance. We conducted a descriptive analysis of survey responses. Results: In total, 2,021 individuals completed the survey. Nearly 16% of respondents agreed with the statement “antibiotics can kill viruses” and almost 12% more were unsure. Thirty percent of respondents either agreed with or were unsure about the statement “antibiotics work on most coughs and colds”. When asked more directly about antimicrobial resistance, almost a quarter (25%) of respondents agreed with or were unsure about the statement “there is no connection between taking antibiotics and the development of resistant bacteria”. Responding to questions about possible negative effects of antibiotics, over 9% disagreed with the statement “antibiotics can kill the 'good' bacteria that normally live on the skin and in the gut” and another 19% were unsure. Similarly, over 20% disagreed with or were unsure about the statement “bacteria that do not respond to antibiotics could infect me or my family”. Reflecting on their own providers, nearly 83% of respondents trusted their doctor’s or nurse’s advice about antibiotic necessity. Conclusions: There are opportunities for patient and community engagement around antibiotic effectiveness for common viral illnesses and about the negative effects of overuse of antibiotics. Our data suggests most patients trust their providers as it relates to antibiotic prescribing and may be receptive to discussions and strategies that promote antimicrobial stewardship.


Connecting Pathogen Transmission and Performance of the WHO’s ‘My 5 Moments of Hand Hygiene’ in a High-Fidelity Simulation
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s98-s99
-
- Article
-
- You have access
- Open access
- Export citation
-
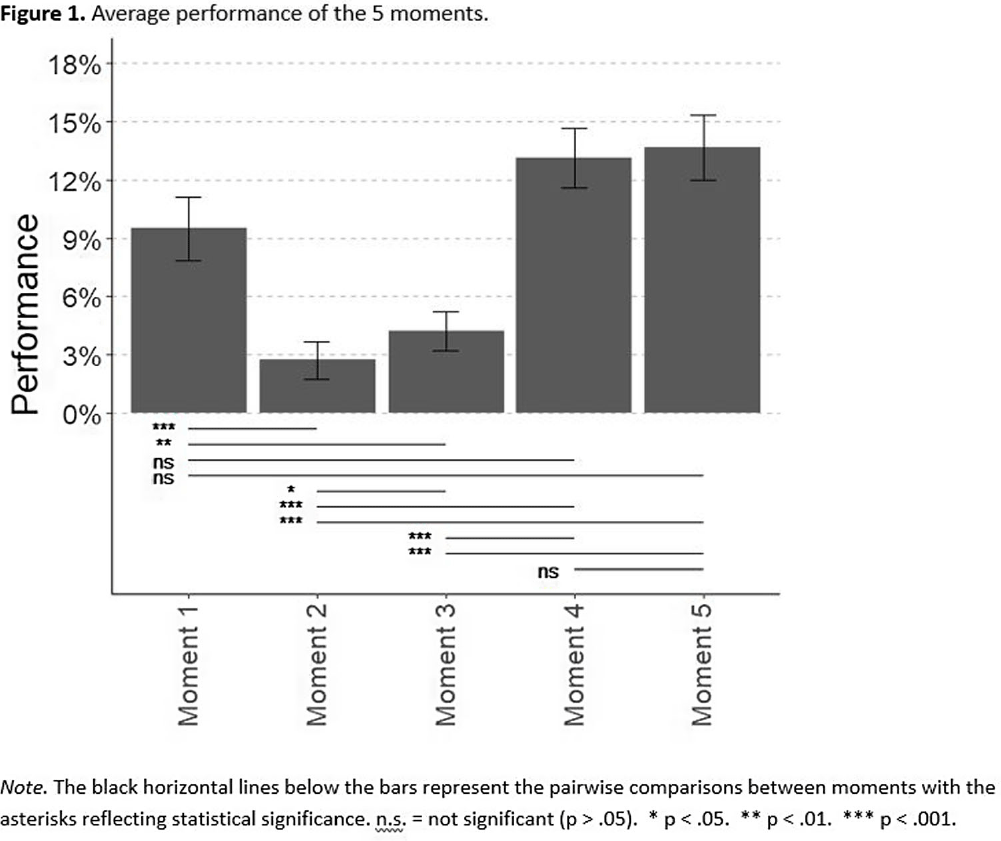
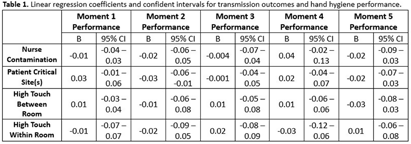
Background: The World Health Organization launched ‘Your 5 moments for hand hygiene’ to identify when healthcare workers should perform hand hygiene to reduce healthcare-associated infections (HAIs). Performing hand hygiene correctly is necessary to decrease pathogen transfer, though little research has assessed the effectiveness of all 5 moments. Methods: Registered nurses (n=42) participated in a standardized, one-hour high-fidelity patient care simulation that were recorded via a head-mounted camera. The simulation involved two patients, each requiring four clinical care tasks (e.g., indwelling Foley catheter insertion, stool sample collection). Transmission data was obtained from the simulations using four genetic variants of bacteriophage λ. Before each simulation, variants were applied to unique locations on two manikins: patient A’s wound, patient A’s stool, patient B’s groin, and patient B’s stool. After each simulation, we sampled the patients, nurse, and high-touch environmental surfaces to determined bacteriophage identity of positive samples. For each moment, hand hygiene performance was the total time the nurse practiced hand hygiene across opportunities over the total recommended time (15 seconds per opportunity). Positive samples were categorized as 1) nurse contamination, 2) patient critical site(s) contamination, 3) high touch surface contamination from the same patient, or 4) high touch surface contamination from the other patient. To compare nurse’s performance of each of the 5 moments, we used a Friedman test and then a Wilcoxon test for pairwise comparisons. To assess the relationship between the four types of transmission outcomes and hand hygiene performance of the 5 moments, we performed linear regressions and calculated 95% confidence intervals by bootstrapping the original cases. Results: Performance of moments 1 (Before patient contact: 9.49%), 4 (After patient contact: 13.11%), and 5 (After contact with patient’s surroundings: 13.66%) were significantly higher than moments 2 (Before clean or aseptic task: 2.72%) and 3 (After bodily fluid exposure: 4.22%; p < 0 .05). Moment 2 perfomance, furthermore, was significantly lower than moment 3 (Figure 1). Only moment 2’s performance was significantly related to transmission; specifically, performance was negatively related to critical site contamination (B= -0.03, CI 95%: -0.06 – -0.01); Table 1. Conclusions: Moment 2performance was the lowest of all 5 moments and was the only moment that demonstrated evidence of relationship with pathogen transmission, specifically critical site contamination. Of all the 5 moments, this moment is most directly related to HAIs. Further research should investigate why moment 2 performance is so low.


Can an animal welfare risk assessment tool identify livestock at risk of poor welfare outcomes?
-
- Journal:
- Animal Welfare / Volume 33 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e32
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Beyond the Prescription Pad—Finding a Window of Opportunity to Prevent Antibiotic Diversion and Non-Prescription Use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s44
-
- Article
-
- You have access
- Open access
- Export citation
-
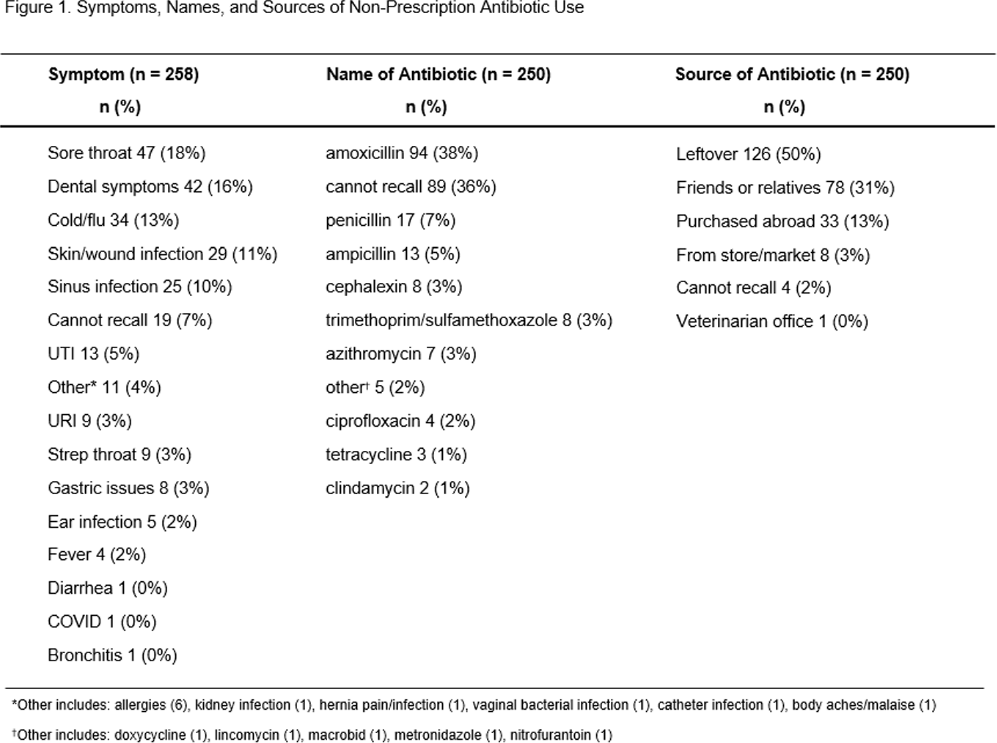
Background: Non-prescription antibiotic use is defined as taking antibiotics without medical guidance, which includes using leftover antibiotics, obtaining antibiotics from friends or relatives, or purchasing antibiotics without a prescription. This study aimed to (1) determine the symptoms prompting individuals to use non-prescription antibiotics, identify their sources of acquisition, and document the types of antibiotics utilized, (2) identify any associated side effects, and (3) gain insights into antibiotic storage practices, including whether antibiotics were used beyond their expiration date. Methods: A cross-sectional quantitative survey was conducted from January 2020-June 2021 in waiting rooms of six safety-net primary care clinics and two private emergency departments in Houston, Texas. Participants were read survey questions in English or Spanish by a bilingual research coordinator, and their responses to five questions about antibiotic use were recorded. Descriptive analysis was performed. Results: Among the 564 patients surveyed, the median age was 51 (range 19-92). The majority identified as female (72%), Hispanic/Latinx (47%), Black/African American (33%), held a college education (44%), and received public health insurance, such as Medicaid or County Financial Assistance (56%). Of all patients surveyed, 44% (246) reported taking an antibiotic without a prescription and answered questions about associated symptoms. Of all symptoms/illnesses associated with non-prescription use, the most common were sore throat (18%), dental symptoms (16%), and cold/flu (13%). The most common sources for non-prescribed antibiotics were leftover antibiotics (50%), from friends or relatives (31%), and purchased abroad (13%), although 3% had purchased non-prescription antibiotics from a local store or market (Figure 1). The most common antibiotics used were amoxicillin (38%) and penicillin (7%). The reported side effects were stomach pain/upset (24%), nausea and vomiting (19%), allergic reaction (e.g., rash) (14%), and diarrhea (14%). Among 246 participants reporting antibiotic use, 63% reported that the antibiotic they took had been previously prescribed for the same symptom/illness, and 93% had acquired antibiotics in a container, of which 90% reported that the container had an expiration date. Conclusions: Our survey reveals that 63% of individuals who use non-prescription antibiotics were motivated by having received prescribed antibiotics for similar symptoms previously. Leftover antibiotics were the source for half of all non-prescription use. These observations suggest that outpatient antibiotic stewardship campaigns have a window of opportunity at the time of the initial prescription of antibiotics, to focus on providing the shortest course possible, and to deliver antibiotic safe use information at that time. Acknowledgments: Financial Support AHRQ R01HS026901
Disclosure: Barbara Trautner: Stock: Abbvie--sold in December 2023; Abbott Laboratories--sold in December 2023; -Bristol Myers Squibb--sold in December 2023; Pfizer--sold in December 2023; Consultant--Phiogen—consultant. Contracted research through NIAID for STRIVE trial, currently testing Shionogi product; Contracted research--Peptilogics; Contracted research—Genentech

epiXact-ONT: Long-read whole genome sequencing for rapid outbreak detection and comprehensive plasmid transmission analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s155
-
- Article
-
- You have access
- Open access
- Export citation
Improving Cleaning Validation Utilizing Adenosine Triphosphate Technology
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s95-s96
-
- Article
-
- You have access
- Open access
- Export citation
-
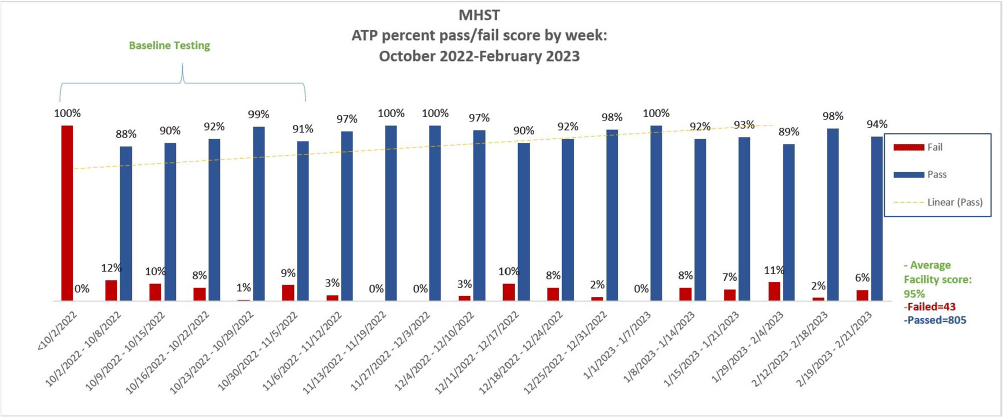
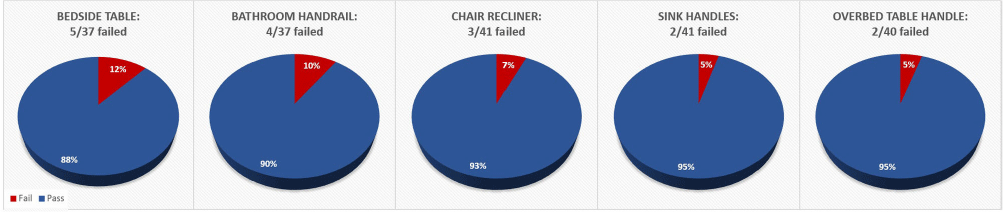
Background: Thorough cleaning and disinfection of high-touch surface areas in hospital inpatient rooms remain vital parts of effective strategies in reducing hospital-acquired infections (HAIs). Currently, Methodist Specialty & Transplant Hospital (MHST) inconsistently utilizes fluorescent marking for terminal cleaning validation. Without quantitative results, it’s difficult to measure the effectiveness of cleaning. To ensure MHST is maintaining a safe and clean environment for patients & staff, MHST implemented a comprehensive cleaning verification program to include adenosine triphosphate (ATP) technology. We aimed to establish the program with baseline readings, and an overall weekly passing score of 95% for all tested inpatient rooms. Methods: To achieve sustained improvement, we needed to monitor, educate, and have periodic performance feedback to individuals and stakeholders. Key stakeholders (IP, EVS, Operations Leadership, Nursing Leadership representative) were identified, and a weekly meeting was established to discuss the planning and implementation of the ATP program. Some key actions included: standardization of brand of luminometer- device to measure ATP for microbial contamination; establishment of 16 high surface touch points to be tested; partnership with IT to create a database & dashboard for ATP results & data analysis; training of ATP device to all personnel who will be utilizing ATP device; establishment of a threshold for a “pass” clean (relative light unit [RLU] less than or equal to 45). Summary of Results: After baseline testing, the average weekly pass score met goal at 95 percent for all tested rooms. The bedside table located on the 2W floor was the location that failed the most (3 instances). Conclusions: Our program implementation project aimed to improve terminal cleaning validation utilizing ATP technology in inpatient rooms, was successfully implemented. Equipped with quantitative results, the MHST team, was able to verify cleaning quickly and efficiently without any confusion, as it may have been with the previous verification method of fluorescent marking. The partnership between Infection Prevention (IP) & Environmental Services (EVS) was crucial in the implementation of this process improvement- from participating in training together to understanding and sharing ATP pass/fail score data.


Impact of Streptococcus pneumoniae Urinary Antigen Testing in a Large Academic Medical Center
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s77-s78
-
- Article
-
- You have access
- Open access
- Export citation
-
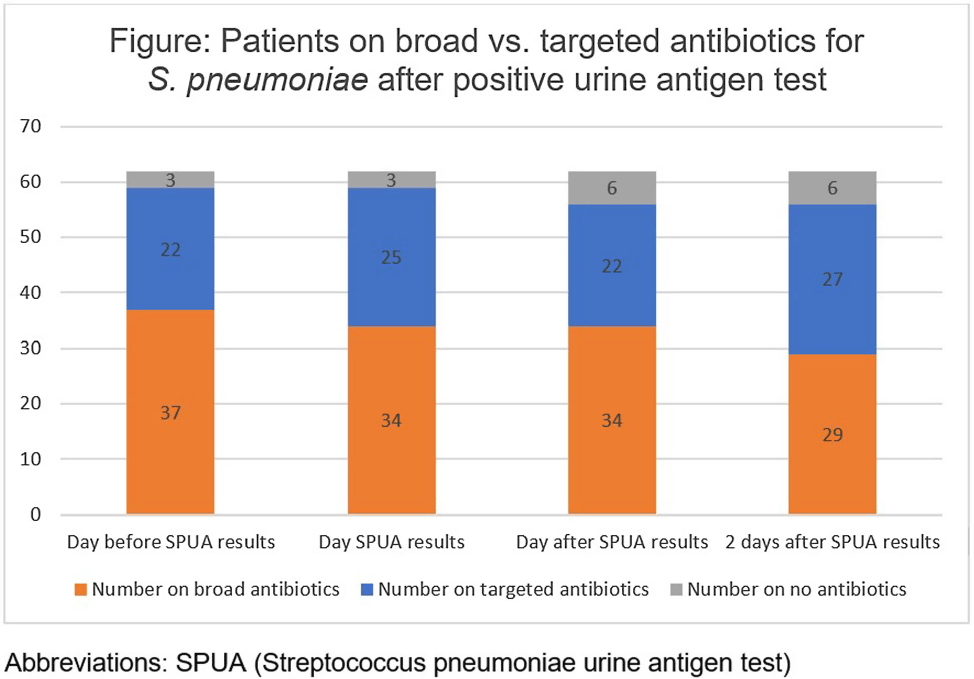
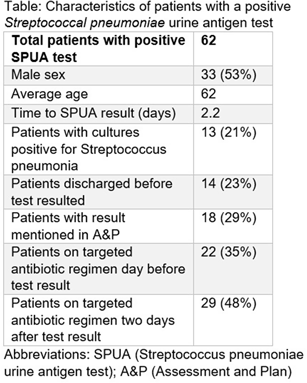
Background: The Streptococcal pneumoniae urine antigen (SPUA) test was developed to increase microbiologic diagnosis of pneumonia. Concerns have been raised about the test’s low sensitivity and failure to alter outcomes by de-escalating antibiotics (PMID:31956656). However, the cost-effectiveness and real-world clinical utility of the test remain unclear. Methods: From June 1, 2022 - May 31, 2023, all patients with a SPUA test in the MUSC Health System were identified via Epic SlicerDicer. Those with a positive test underwent chart review. Antibiotics were classified as a “broad” or “targeted” regimen for S. pneumoniae. Targeted regimens included penicillins without beta-lactamase inhibitors, 1st-3rd generation cephalosporins, doxycycline, levofloxacin or moxifloxacin (with or without azithromycin), as well as azithromycin monotherapy. Broad regimens included 4th generation or higher cephalosporins, carbapenems, penicillins with beta-lactamase inhibitors, and vancomycin. Results: In one year, 1,518 patients had a SPUA test ordered. 62 (4%) patients had a positive test. Of those 62 patients, 14 patients were discharged before the test resulted (Table). The average turnaround time for the test was 2.2 days. When comparing antibiotic therapy on the day before the SPUA test resulted to two days after the test resulted, only 7 additional patients were switched to a targeted regimen (Figure). Conclusion: Of 1,518 SPUA tests ordered in a year, most (1,456 or 96%) were negative, with minimal changes to antibiotic therapy based on positive Results: These results are similar to other real-world studies, which showed a positive test prevalence between 4-8% (PMID:30265290) with 15-30% of patients changed to targeted antibiotics following a positive result (PMID:23111919, PMID: 28053969). The SPUA test cost approximately $44,022 (based on $29 test price) but has limited utility in a real-world setting.
Disclosure: Krutika Hornback: Speaker’s Bureau - Cepheid Diagnostics


Candida auris in the Healthcare Environment: Prevalence, Anti-Fungal Resistance, and Survival on Porous & Non-Porous Surfaces
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s90
-
- Article
-
- You have access
- Open access
- Export citation
Evaluation of minimum inhibitory concentration data in National Healthcare Safety Network’s Antimicrobial Resistance Option
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s31-s32
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Clinical laboratories perform antimicrobial susceptibility testing (AST) primarily by determining the minimum inhibitory concentration (MIC) for an organism–antimicrobial combination and comparing it with established breakpoints to generate interpretations. The Antimicrobial Resistance (AR) Option of CDC’s National Healthcare Safety Network (NHSN) permits hospitals to submit clinical isolate AST data, including test values and interpretations (Figure 1). The Clinical and Laboratory Standards Institute (CLSI) periodically revises breakpoints, but their adoption by clinical laboratories can be delayed, potentially affecting national AR surveillance data accuracy. Using MIC values, instead of clinical laboratory interpretations, can improve surveillance data accuracy and overcome misclassification due to delayed uptake of revised breakpoints. We evaluated the completeness and consistency of MIC data submitted to the AR Option for fluoroquinolone-resistant Escherichia coli and methicillin-resistant Staphylococcus aureus (MRSA). Methods: We included data on (1) E. coli isolates tested for ciprofloxacin or levofloxacin susceptibility and (2) S. aureus isolates tested for oxacillin or cefoxitin susceptibility in 2022 and reported by October 1, 2023. We evaluated completeness among isolates reporting a final AST interpretation as the proportion of isolates reporting both an MIC value and interpretation. We evaluated consistency using percent agreement comparing the laboratory’s MIC interpretation (classified as resistant or not resistant) with the interpretation derived by applying 2021 CLSI M100 breakpoints to the MIC values reported for the same isolate. Results: Across 974 hospitals, fluoroquinolone MICs and interpretations were reported for 172,012/393,359 E. coli isolates (43.7%), and oxacillin or cefoxitin MICs and interpretations were reported for 38,519/79,372 S. aureus isolates (48.5%). Of isolates with both MIC values and interpretations, 157,902 (91.8%) E. coli and 7,808(79.7%) S. aureus isolates had MICs that could be classified as resistant or non-resistant (i.e., intermediate or susceptible) per CLSI breakpoints (Figure 2). The remaining MICs were unclassifiable (reported as intervals spanning CLSI breakpoints, e.g., ≤1 μg/ml ciprofloxacin for E. coli). Among isolates with classifiable MICs, the agreement between the clinical laboratory and CLSI-based interpretation was 99.5% for E. coli and 99.7% for S. aureus. Conclusion: MIC values and interpretations were available for




Twilight blooms
-
- Journal:
- Palliative & Supportive Care / Volume 22 / Issue 6 / December 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. 2228
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Longitudinal Follow Up of Patients Colonized with Clostridioides difficile: a Retrospective Cohort Study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s66-s67
-
- Article
-
- You have access
- Open access
- Export citation
Heterogeneity in Pre-operative Staphylococcus aureus Screening and Decolonization Strategies among Healthcare Institutions
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s75
-
- Article
-
- You have access
- Open access
- Export citation
-
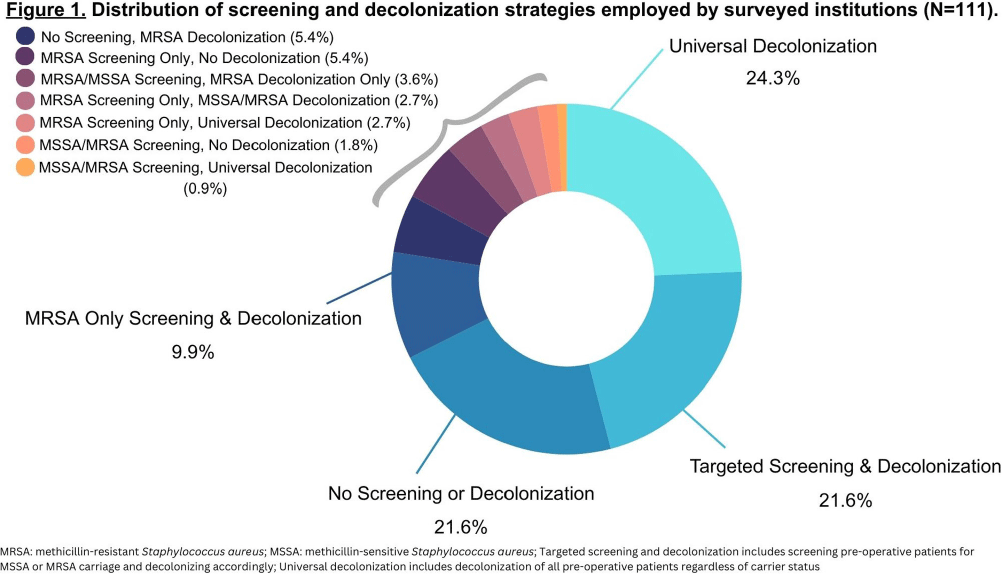
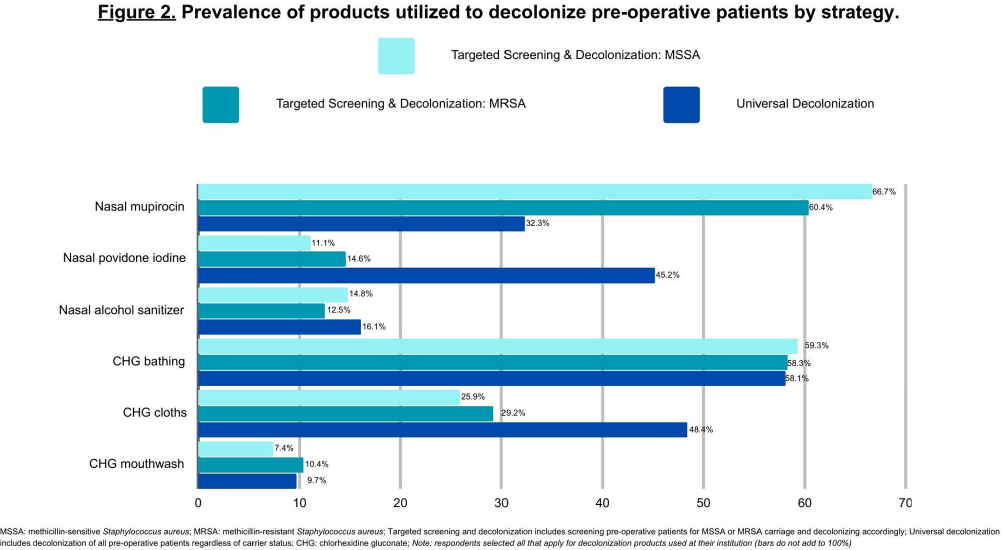
Background: Staphylococcus aureus (SA) is the most common pathogen causing surgical site infections (SSIs). In the past decade, strategies incorporating new SA decolonization products have been implemented to prevent SSIs in surgical patients. The objective of this cross-sectional study was to determine which pre-operative screening and decolonization strategies are currently utilized in healthcare institutions. Methods: A survey was programmed in REDCap and emailed to members of the Society for Healthcare Epidemiology of America Research Network, the Minnesota chapter of the Association of Practitioners in Infection Control and Epidemiology, and the Minnesota Hospital Association between May-August 2023. We report the prevalence of institutional screening and decolonization strategies and decolonization products used for the prevention of SA SSIs. Results: A total of 153 unique institutions initiated the survey and 111 provided complete data on their institutional screening and decolonization strategies. The most commonly reported strategies included universal decolonization (decolonization of pre-operative patients without screening for carrier status) (n=31, 27.9%), no screening or decolonization (n=24, 21.6%), targeted screening for methicillin-sensitive Staphylococcus aureus (MSSA) or methicillin-resistant Staphylococcus aureus (MRSA) and decolonization based on carrier status (n=24, 21.6%), or MRSA only screening and decolonization (n=11, 9.9%) (Figure 1). Institutions that utilized targeted screening and decolonization strategies frequently reported using nasal mupirocin (n=18, 66.7%MSSA, n=29, 60.4%MRSA), chlorhexidine gluconate (CHG) bathing (n=16, 59.3%MSSA, n=28, 58.3%MRSA), and CHG cloths (n=7, 25.9%MSSA, n=14, 29.2%MRSA) (Figure 2). Among the 31 institutions that reported implementing the universal decolonization strategy, CHG bathing (n=18, 58.1%), CHG cloths (n=15, 48.4%), and nasal povidone iodine (n=14, 45.2%) were the most prevalent decolonization products. Additionally, a smaller percentage of institutions used nasal alcohol gel (n=5, 16.1%) for universal decolonization. Conclusion: Compared to the survey we conducted in 2012, we report a new shift towards universal decolonization and a small increase in targeted SA screening and decolonization.1 In the 2012 survey we reported 37% of respondents’ institutions screened pre-operative patients for SA carriage and the majority of those institutions decolonized carriers.1 Universal decolonization was not reported in the 2012 survey.1 We highlight the continued heterogeneity in practice at this time, which may reflect the ongoing uncertainty in optimal decolonization practices and emphasizes the need for future research. References: 1. Kline, S. et al. Infect Control Hosp Epidemiol 2014;35(7):880-882.


Relationship between Hand Hygiene and MDRO Acquisition after Implementation of an Electronic Hand Hygiene Monitoring System
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s100-s102
-
- Article
-
- You have access
- Open access
- Export citation
-
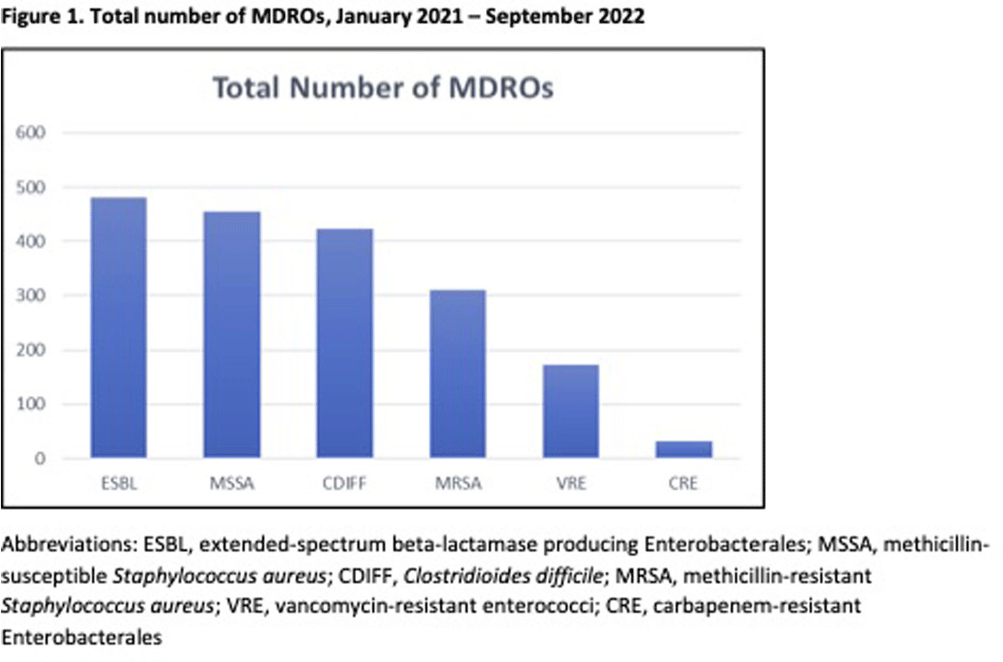
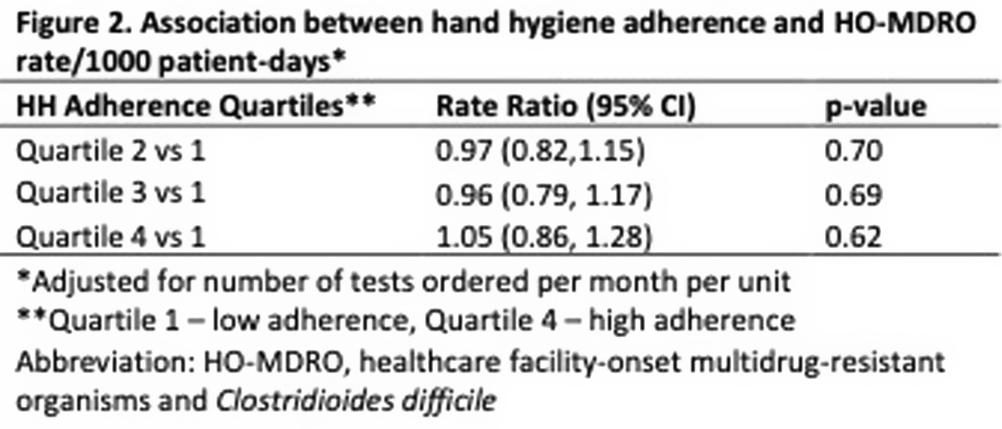
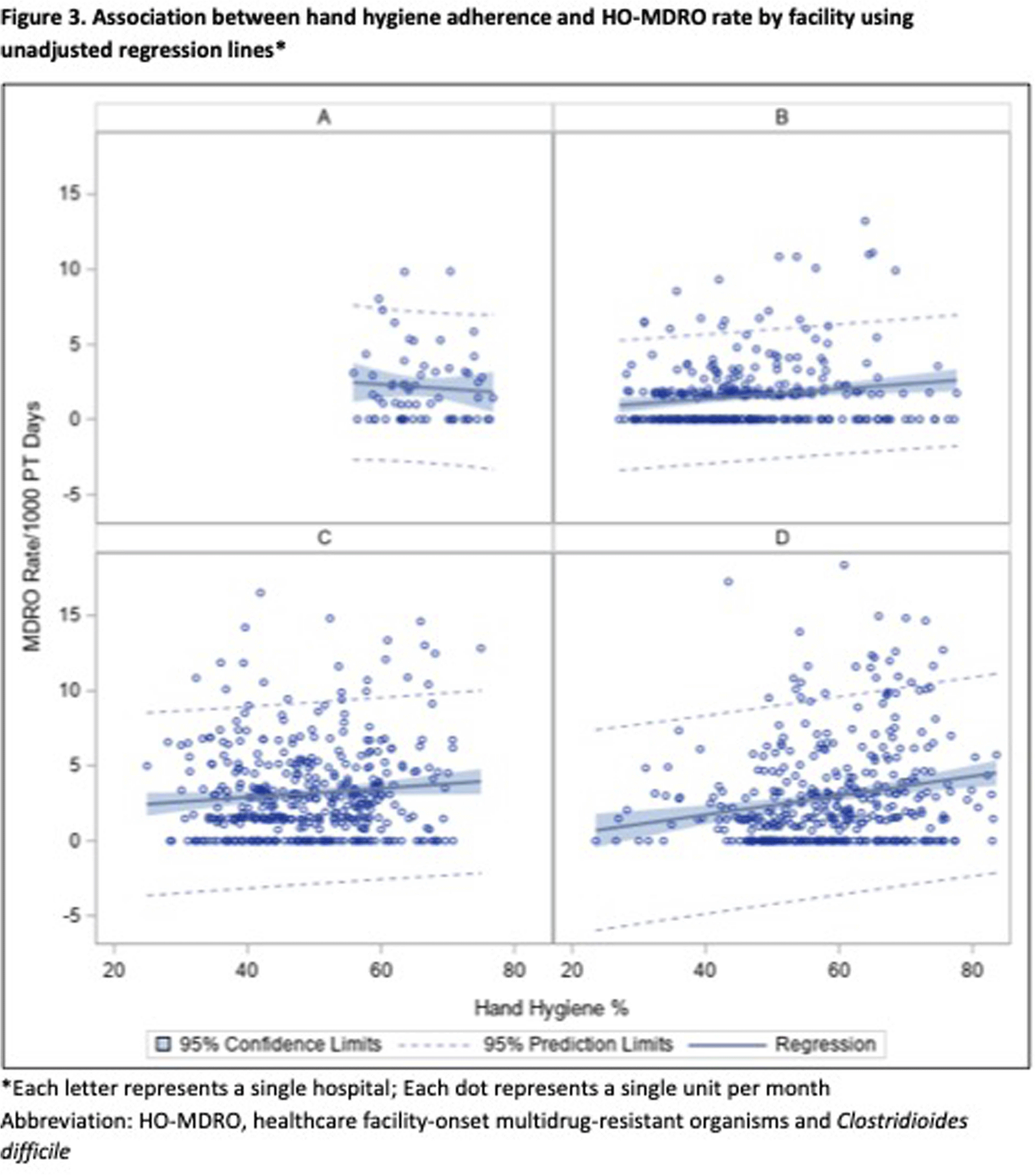
Background: Hand hygiene (HH) is fundamental to preventing the transmission of pathogens between patients. Unfortunately, adherence to HH is suboptimal and monitoring adherence is challenging. Electronic HH monitoring systems (EHHMS) are emerging potential solutions to increase the number of HH observations and eliminate the potential for observation bias. This aim of this study is to assess the impact of improved HH adherence after the introduction of an EHHMS on the rates of healthcare facility-onset multidrug-resistant organisms and Clostridioides difficile (HO-MDRO). Methods: We performed a retrospective, quasi-experimental study to evaluate the impact of HH on HO-MDROs across 4 acute care facilities (59 hospital units, 14 of which were ICUs) from January 2021 - September 2022 after implementing an EHHMS in a large academic healthcare system. Clinical cultures from all sources were included; routine surveillance cultures were not collected during this period. HO determination was made using National Healthcare Safety Network (NHSN) definitions. The association between monthly unit-level HH adherence (%) and HO-MDRO rate per 1000 patient-days was assessed using mixed-effects Poisson regression using rate ratios (RR), which accounts for unobserved heterogeneity between units while controlling for number of tests ordered per month per hospital unit. HH adherence was stratified in quartiles (Q1: 24-43%, Q2: 43-51%, Q3: 52-61%, Q4: 61-84%). Results: During the study period, there were 23 million HH opportunities and 1875 MDROs in 772,930 patient-days. HH adherence increased from 41% January 2021 to 57% September 2022. ESBL, MSSA, and CDIFF accounted for most MDROs (Figure 1). The mean monthly HH adherence rate was 52% per unit, with a median of 1.66 (IQR: 0-3.5) MDROs/1000 patient-days. Mixed-effects Poisson regression suggested no significant overall relationship between HH adherence and MDRO rate (Figure 2). A close to null association was observed when comparing quartile two to quartile one (RR: 0.97, 95% CI: 0.82, 1.15), quartile three to quartile one (RR: 0.96, 95% CI: 0.79, 1.17), and quartile four to quartile one (RR: 1.05, 95% CI: 0.86, 1.28). Results were similar across hospitals (Figure 3). Conclusions: Although implementing an EHHMS led to an improvement in HH adherence, we were not able to demonstrate a resultant decrease in HO-MDROs. Potential explanations include the relatively rare outcomes of interest, unrecognized confounders, and the complex interaction between HH and HO-MDROs, since poor HH adherence on a unit may lead to increased attention from infection prevention and therefore increased focus on other MDRO prevention measures.



Psychological Impact of the Volcanic Eruption in La Palma Spanish Island: Predictors of Depression, Anxiety, Stress, and Well-being
-
- Journal:
- The Spanish Journal of Psychology / Volume 27 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e18
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Variability of MDRO Reporting Across Tennessee Microbiology Laboratories
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s153
-
- Article
-
- You have access
- Open access
- Export citation
-
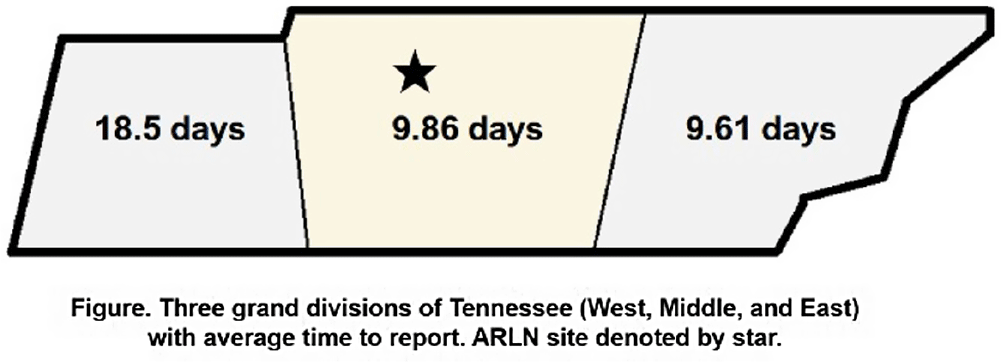
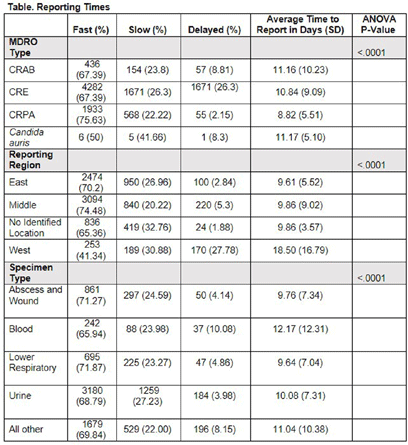
Background: Identification and timely reporting of multi-drug resistant organisms (MDROs) drives efficacy of infection prevention efforts. Data on MDRO reporting timeliness and inter-facility variability are limited. Facility-dependent variability in MDRO reporting across Tennessee was examined to identify opportunities for MDRO surveillance improvement. Methods: Data for reported Tennessee MDROs including carbapenem-resistant Enterobacterales (CRE), carbapenem-resistant Acinetobacter baumannii (CRAB), Carbapenem-resistant Pseudomonas aeruginosa (CRPA) and Candida auris, were obtained from the southeast regional Antibiotic Resistance Laboratory Network (ARLN) from 2018-2022, excluding screening and colonization specimens. Variance in days accrued from specimen collection to ARLN receipt was analyzed using one-way analysis of variance (ANOVA) with Tukey’s test (SAS 9.4). Facilities were categorized as fast (1-10 days), slow (11-20 days), or delayed (21-100 days) reporters. Results: There were 9,569 MDRO isolates reported. CRPA was reported faster than other MDROs (p < 0.001), while specimens from West Tennessee compared to other regions (p < 0.001) (Figure) and blood cultures compared to other specimens were reported more slowly (p < 0.001) (Table). There was no difference in reporting times for facilities using on-site microbiology laboratories versus reference laboratories (P = 0.062). Conclusion: MDRO reporting times varied across Tennessee by region, specimen, and organism. Future work to elucidate drivers of variability will consist of surveys and focused interviews with laboratory personnel to identify shared and unique barriers and opportunities for improvement.


Staff Perspectives on Barriers & Facilitators to Meeting Hand Hygiene Goals in a Multicenter Academic Hospital System
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s99
-
- Article
-
- You have access
- Open access
- Export citation
-
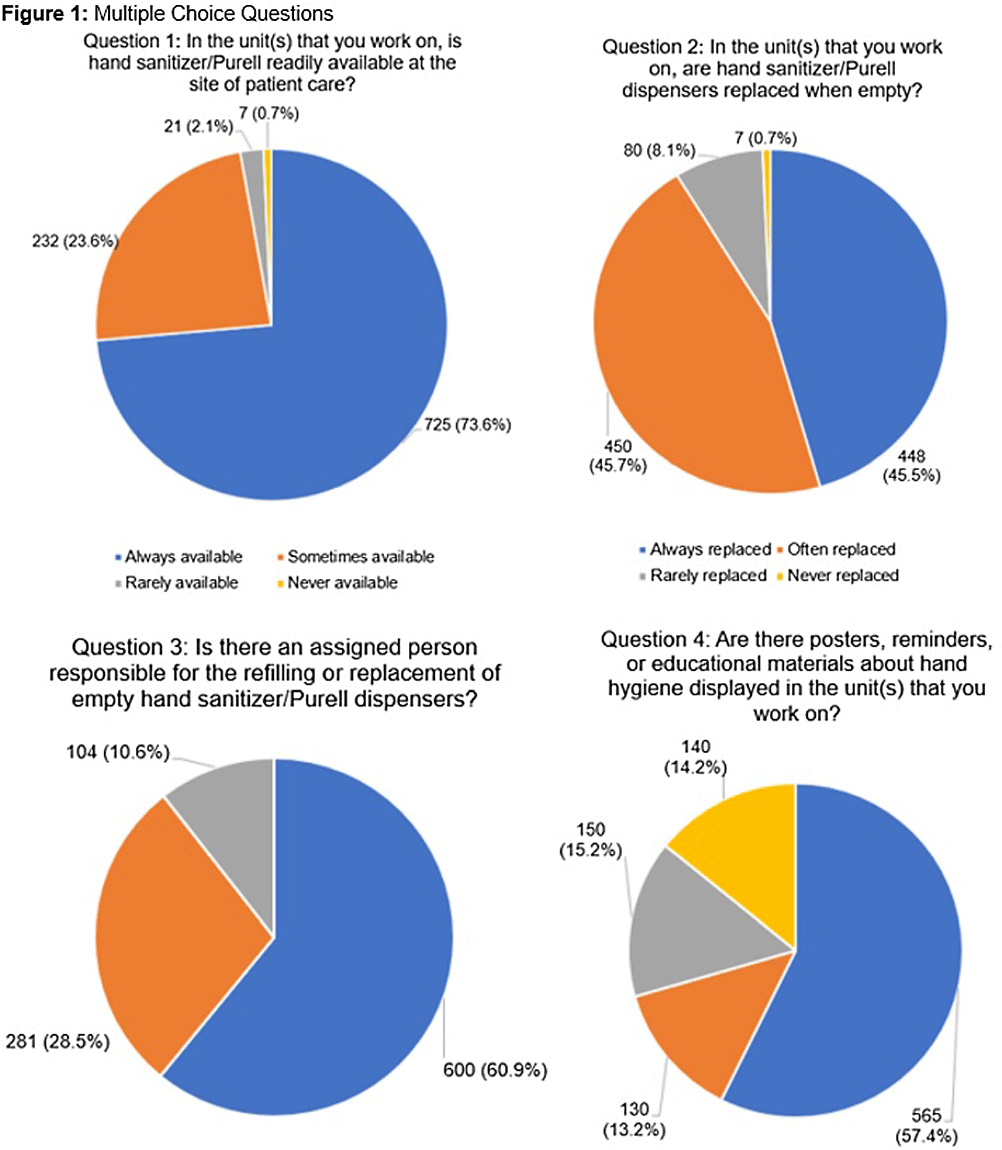
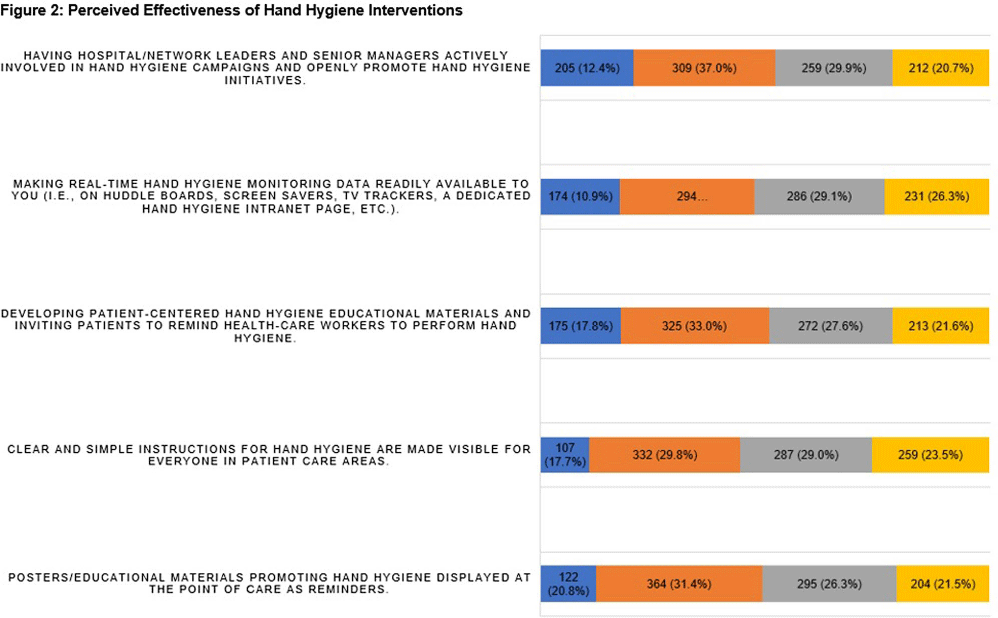
Background: Proper hand hygiene is the most important practice to reduce the transmission of infections in healthcare settings. Despite this, healthcare institutions continue to struggle to achieve and maintain high rates of hand hygiene compliance among healthcare workers with some studies estimating national healthcare worker hand hygiene compliance to be approximately 50%. Methods: We conducted an anonymous one-time survey of our Lifespan Hospital System employees to evaluate barriers and facilitators to performing hand hygiene as well as interventions to improve hand hygiene compliance. The survey was designed with guidance from the Consolidated Framework for Implementation Research and input from Lifespan infection prevention staff. Result: Over four weeks 985 (6%) Lifespan employees completed the survey. Figure 1 shows the aggregate results of the first 4 survey questions which focused on hand hygiene infrastructure at Lifespan, including availability of sanitizer, staff to manage hand hygiene supplies, and educational materials/reminders. One significant finding was >70% of respondents reported that they either did not know if their unit/department has a person assigned to replace/monitor hand hygiene supplies, or if so, who that person is. We also asked employees to rate how effective different interventions would be at improving hand hygiene compliance. Figure 2 shows of five proposed interventions, three were rated as either “moderately effective” or “very effective” by >50% of respondents. These included displaying hand hygiene instructions, making hand hygiene data available to employees, and displaying materials/reminders promoting hand hygiene. There were also 977 free-text responses regarding “barriers or facilitators to proper hand hygiene”. Major barriers identified were a lack of staff to monitor and refill supplies, slow replacement of hand hygiene products, lack of sanitizer dispensers and sinks, inconsistency of sink location and dispenser placement, lack of hand hygiene reminders/educational materials, time constraints, skin irritation from sanitizer, and an inability to have dispensers in behavioral health units. Survey responses led us to enhance the following: educational materials and reminders in work areas; staff education; leadership involvement in hand hygiene initiatives; routine auditing and feedback; conveniently placed sanitizer dispensers and sinks at the point of care; and making hand hygiene compliance data readily available to staff. Conclusion: This survey identifies important barriers and facilitators to achieving high rates of hand hygiene compliance among healthcare workers and provides the basis for interventions aimed at improving hand hygiene compliance in a large multicenter academic hospital system.