Refine listing
Actions for selected content:
142351 results in Open Access
Retreat of the Greenland Ice Sheet leads to divergent patterns of reconfiguration at its freshwater and tidewater margins
-
- Journal:
- Journal of Glaciology / Volume 70 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e65
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Survey of VA Laboratory Practices for Carbapenem-resistant Acinetobacter baumannii and Pseudomonas aeruginosa
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s79
-
- Article
-
- You have access
- Open access
- Export citation
Pilot of a Bowel Habit Assessment Tool to Enable Early Identification of C. diff Infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s63
-
- Article
-
- You have access
- Open access
- Export citation
-
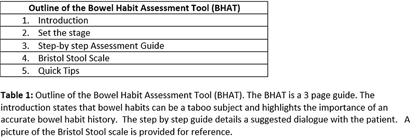
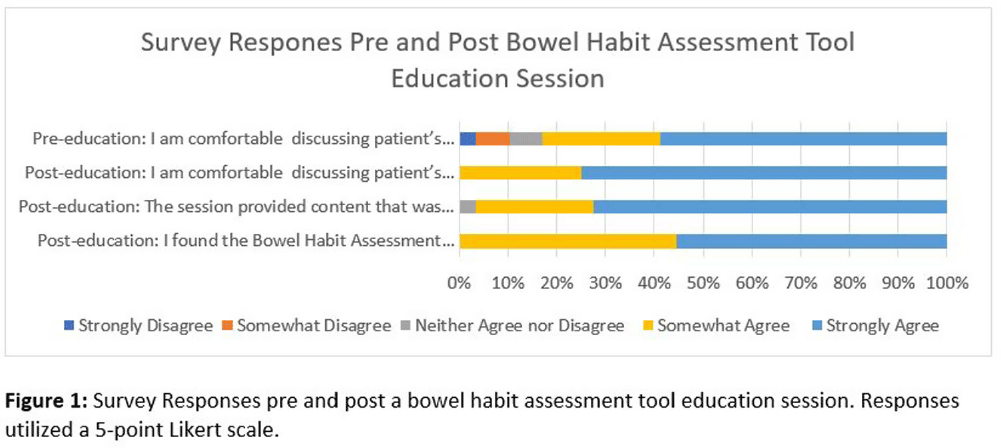
Background: Gastrointestinal conditions are common in hospitalized patients. Decreased mobility, dietary changes, medications and their underlying illness may alter patients’ bowel movements. It’s important for health care providers to be aware of patient’s bowel habits, especially for early identification of Clostridiodies difficile infection (CDI). Prior research has shown that patient modesty may be a barrier to discussing bowel habits with nurses and providers. This can lead to delay in diagnosis of CDI, lack of timely isolation and possible misclassification of community onset CDI cases as hospital onset (HO-CDI). Methods: A Bowel Habits Assessment Tool (BHAT) was developed to assist health care providers in learning skills to assess and document patient bowel habits accurately. The tool provides a structured approach to help clinicians gather relevant information, identify abnormalities, and promote effective communication with patients. The tool was developed by an infectious disease physician and modeled on existing tools utilized to take a sexual history. A team of infectious disease physicians, nurses and a gastroenterologist reviewed the tool and provided feedback. See Table 1. The tool was introduced as a pilot program at a 180 bed academically affiliated Veterans Affairs Hospital. Micro educational sessions were held to provide education about the importance of a bowel habit history, introduce the tool and teach its use in clinical care. The teaching sessions were led by an Infectious Disease physician and a nurse infection preventionist. An anonymous pre and post survey employing a 5-point Likert scale was administered to participants. All participation was voluntary. This project was reviewed and approved as a Quality Improvement by the VA Research Office, Eastern Colorado Health Care System. Results: Twenty nine healthcare personnel participated in the pilot. Participants included nurses (13), resident physicians (13), medical students (2) and nursing assistants (1). 59% of participants stated that they strongly agree with the statement “I am comfortable discussing patient’s bowel habits” on the pre-survey. (Question 1). This increased to 73% after the BHAT educational session. The mean difference between pre and post survey responses for question one was 0.45 (CI 0.08761 to 0.8089, p= 0.0167). All participants found the BHAT related to their work and useful, with 41% strongly agreeing and 52% somewhat agreeing that the BHAT was useful. See figure 1: Survey Responses. Conclusions: The effectiveness of a bowel habit assessment tool was demonstrated using a pre and post survey. BHAT improved clinicians comfort level discussing patient’s bowel habits.


A One-year Hospital System Review of Plasma Next-Generation Sequencing in a Mixed Population
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s84
-
- Article
-
- You have access
- Open access
- Export citation
System infection prevention in hospital networks – a SHEA research network survey
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s108
-
- Article
-
- You have access
- Open access
- Export citation
Real-time Whole Genome Sequencing Surveillance as an Effective Outbreak Detection and Mitigation Tool
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s113-s114
-
- Article
-
- You have access
- Open access
- Export citation
-
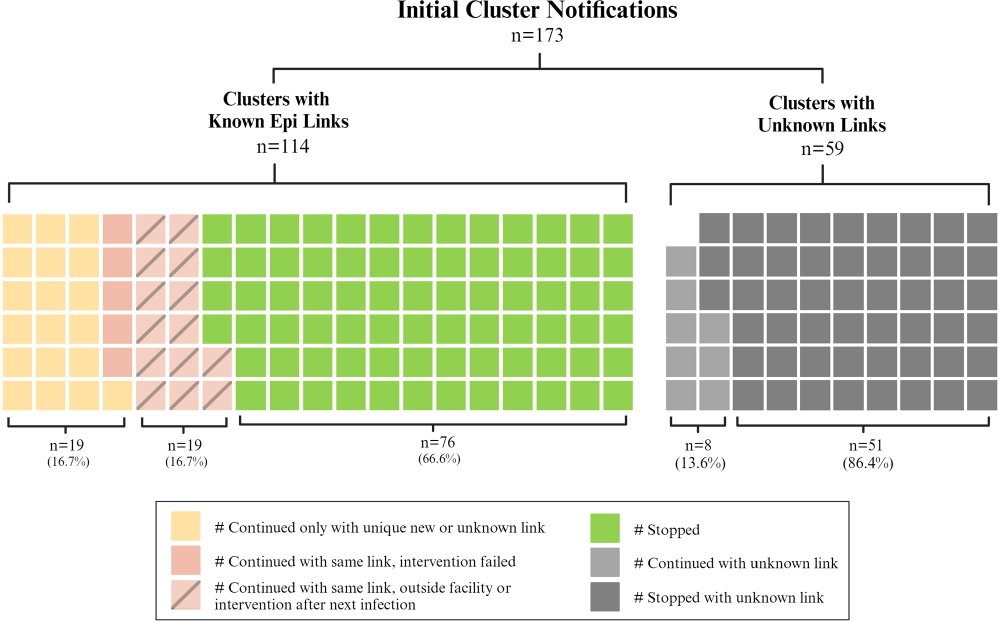
Background: Detection of outbreaks traditionally relies on passive surveillance, and often misidentify or miss outbreaks. Whole genome sequencing (WGS) surveillance has emerged as a proactive measure, enabling early detection of outbreaks and facilitating rapid intervention strategies. WGS surveillance has not been widely studied due to infrastructure, cost, and evidence barriers regarding its impact on reducing healthcare-associated infections (HAIs). This study represents findings from two years of a real-time WGS surveillance program called the Enhanced Detection System for Healthcare-associated Transmission (EDS-HAT). Methods: The study was conducted at UPMC Presbyterian hospital, a 694-bed tertiary care center. Patient isolates of select bacterial pathogens were collected and underwent WGS weekly from November 2021 to November 2023. Potential transmission was defined using single-nucleotide polymorphism thresholds (≤15 for all organisms except Clostridioides difficile). Genetically related clusters were reviewed weekly for epidemiological linkages (unit, personnel, or procedural commonalities) and appropriate interventions were initiated by the infection prevention and control team. We described the frequency of genetic relatedness and nature of epidemiological linkages. Results: Of 7,051 eligible unique patient organism isolates, 4,723 were deemed healthcare-associated and underwent WGS. EDS-HAT identified 478 (12.2%) isolates genetically related to ≥1 other isolate across 173 clusters. Epidemiological links were found in 278 (58.2%) isolates in 114 clusters, with the majority being unit-based (205 isolates, 71.9%); other epidemiological links included equipment or healthcare workers (32 isolates, 11.5%), external facilities (24 isolates, 8.6%), and shared endoscopes (17 isolates, 6.1%); all endoscope outbreaks were effectively contained at two patients. No epidemiological links could be identified for 200 (41.8%) isolates. Infection prevention initiated 134 interventions in 114 clusters, including 74 (55.2%) general staff notification and education, 25 (18.7%) enhanced cleaning efforts, 23 (17.2%) hand hygiene/personal-protective equipment compliance observations, 9 (6.7%) environmental cultures, and 3 (2.2%) enhanced microbiological surveillance. Following the detection of an epidemiological link and intervention, 94/101 (94.1%) outbreaks were effectively halted on the intervened route (Figure). Conclusion: This study demonstrates the feasibility and efficacy of EDS-HAT as an infection prevention tool. Early detection and intervention of outbreaks significantly enhance the capability of healthcare facilities to control and prevent the spread of HAIs. Investment in infrastructure and implementation costs will result in reducing pathogen transmission and improving patient safety in acute care settings.
Disclosure: Alexander Sundermann: Honoraria - Opgen

“AWECoP has made my teaching experience so much better!” – Creating community and improving teaching practice through an Animal Welfare Education Community of Practice (AWECoP)
-
- Journal:
- Animal Welfare / Volume 33 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e35
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Automated Discontinuation of Isolation Precautions with the Use of Electronic Health Record Tools
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s135
-
- Article
-
- You have access
- Open access
- Export citation
-
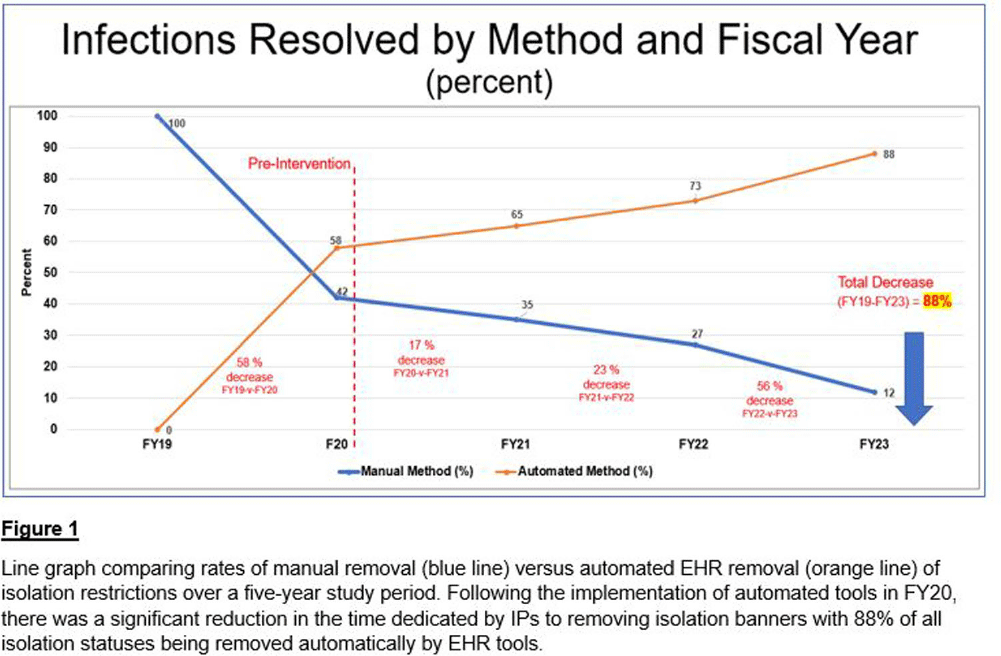
Background: At a comprehensive cancer center, hundreds of patients are screened daily for infections requiring the implementation of isolation precautions. Discontinuation of precautions is determined by negative testing, resolution of infection, or other criteria. Determining appropriate discontinuation of isolation precautions is labor intensive for Infection Preventionists (IPs). An unintended consequence of manual discontinuation is that numerous patients remain on isolation indefinitely. This was amplified during the COVID-19 pandemic when thousands of patients were placed on isolation precautions. Using electronic health record (EHR) tools, opportunities for process improvements were developed. Our goal was to establish an automated method to resolve isolation precautions. We aimed to decrease the number of manually resolved precautions by 25% each fiscal year (FY), compared to our baseline of activity in FY 2019 (FY19). Our secondary aim was to automate adding and resolving precautions when testing is initiated for suspected transmissible conditions (rule-out testing features).
Methods: Infection Control (IC) collaborated with EHR analysts to build tools to automate a process for appropriate isolation discontinuation. We reviewed our internal data in conjunction with evidence-based guidelines and started with acute, short-term infections that do not require repeat testing or cultures. Expiration dates were established for these infections to resolve automatically after meeting criteria. A secondary review determined that additional infections could be added safely to this process. The secondary aim of establishing rule-out testing was implemented for respiratory viral panels (including SARS-COV-2) and C. difficile testing. When testing was ordered for these conditions, a suspect-infection status and alert for precautions were automatically added to patients’ EHR banners. If the assay resulted negative, the suspect-infection status was automatically removed from their chart. Results: Our baseline of active infections in FY19 was approximately 2,700 cases. From FY19 through FY23, 123,115 infections were added to our patients, and 128,422 infections were resolved. In the first year of implementation, there was a 58% decrease in the number of manually resolved cases. From the initiation of our project through the end of FY23, manual discontinuation of precautions has decreased by 88%. Conclusions: We successfully implemented a process improvement project to appropriately remove patients from isolation precautions automatically using EHR tools, which resulted in reduced labor on our IPs and patient time spent on isolation restrictions. Additional benefits from this process improvement extend to decreasing unnecessary costs to the patient and the organization, better stewardship of supply/resources, and improving patient satisfaction.

Outpatient Antibiotic Consumption Trends in Belgium: A Comparative Analysis of Reimbursement and Sales Data, 2013-2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s152-s153
-
- Article
-
- You have access
- Open access
- Export citation
-
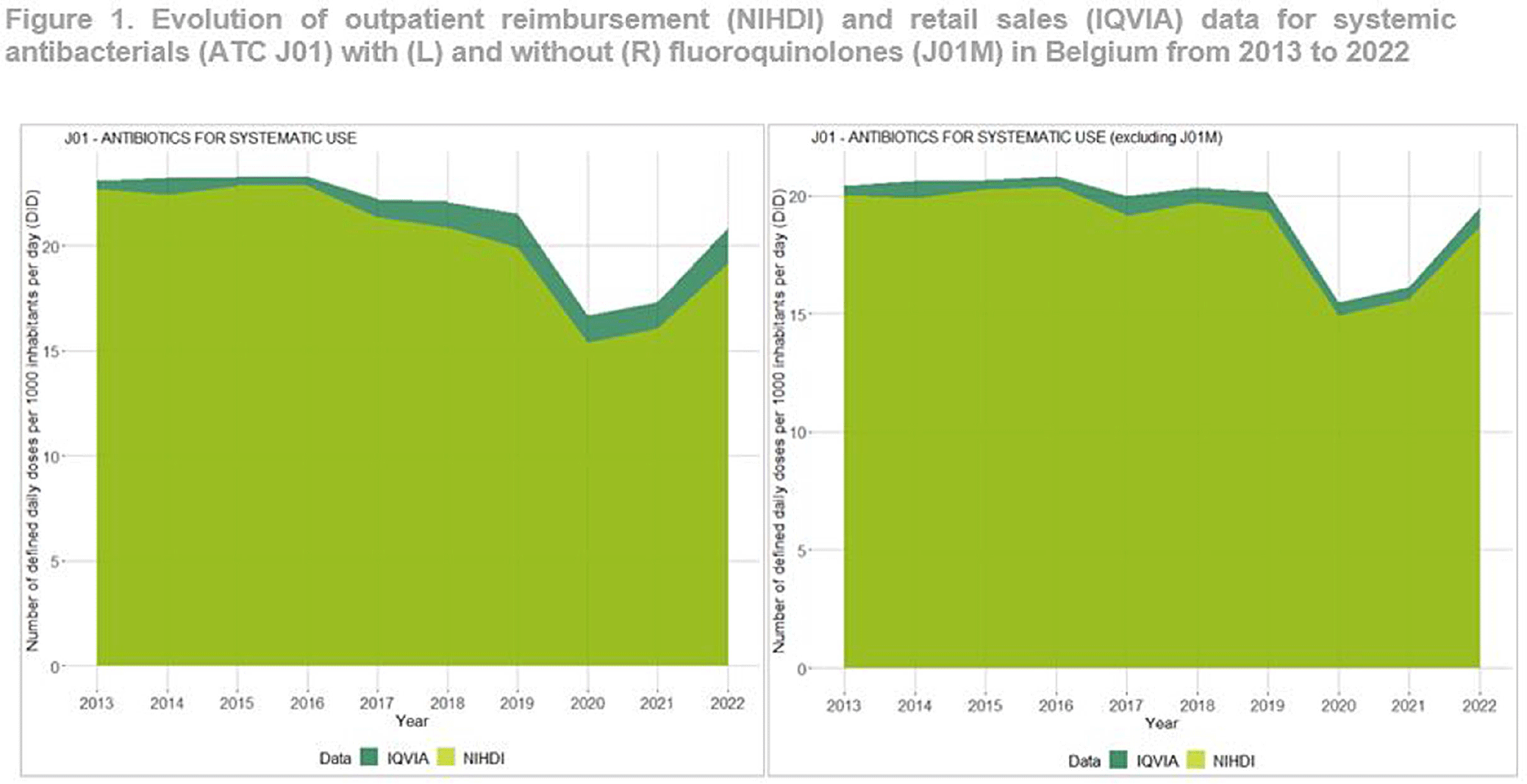
Background: Antimicrobial resistance (AMR) is a global public health concern, necessitating close and timely monitoring of antibiotic consumption (AMC). In Belgium, AMC surveillance traditionally relies on reimbursement data, excluding over-the-counter non-reimbursed or imported products and involving a time lag. This study investigates disparities in AMC between reimbursement data and retail data, providing insights into AMC variations. Additionally this study seeks to critically evaluate the validity and representativeness of the reimbursed data in accurately reflecting the true extent of AMC in the country. Method: Utilizing reimbursement data from the National Institute for Health and Disability Insurance (NIHDI) and retail data (IQVIA Sales data; www.iqvia.com) for systemic antibacterials (ATC Group J01), outpatient consumption was estimated for the period 2013-2022. Volume of antimicrobials was measured in Defined Daily Doses (DDDs - WHO ATC/DDD Index 2023), while population data were extracted from Eurostat. Relative differences (RDs) in DDDs per 1000 inhabitants per day (DID) were computed, and validated through correlation analysis (Pearson’s r) and Bland–Altman plots. Result: J01 antibacterial sales declined from 23.10 DID (2013) to 20.85 (2022). Non-linear decreases, notably during the Covid-19 pandemic (21.54 DID in 2019 to 16.69 in 2020), followed by a rebound to pre-pandemic quantities in 2022 were observed (Figure 1). Reimbursement NIHDI data slightly underestimated IQVIA sales, with RDs ranging from 2% (2013) to 9% (2022). Notable differences, especially in recent years were attributed to quinolone reimbursement criteria changes implemented by law in Belgium in 2018, reducing the reimbursed proportion from 99% (2017) to 35% (2022). ATC-3 level analysis revealed disparities in low-DID groups (J01B, J01E and J01G). Notably, a small proportion of amphenicols (J01B) were reimbursed ( < 1 0%), with a congestion relieving combination product of tiamphenicol (+ N-acetylcysteine; Fluimucil®) frequently bought and remaining unreimbursed. Overall and across ATC3 groups, the correlation between NIDHI and IQVIA estimates was almost perfect across years and the Bland–Altman plots showed high agreement. Conclusion: Reimbursement data are reliable for outpatient AMC monitoring with slightly lower estimates than retail data across most categories. The 2018 quinolone reimbursement criteria change highlights the necessity of incorporating retail data for accurate assessments in this specific category. The synergistic use of reimbursement and retail datasets is crucial for a comprehensive understanding of consumption patterns, supporting effective AMR mitigation strategies in Belgium.

Changes in Antibiotic Use and Disruptions to Antimicrobial Resistance Detection in South Africa and Uganda, 2019 – 2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s132
-
- Article
-
- You have access
- Open access
- Export citation
Comparative Analysis of Healthcare-associated Bloodstream Infections & CLABSI Surveillance in A Singaporean tertiary Hospital
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s154-s155
-
- Article
-
- You have access
- Open access
- Export citation
-
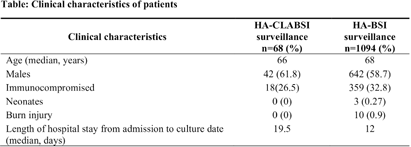
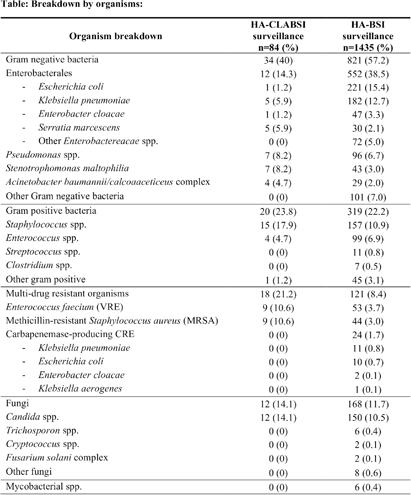
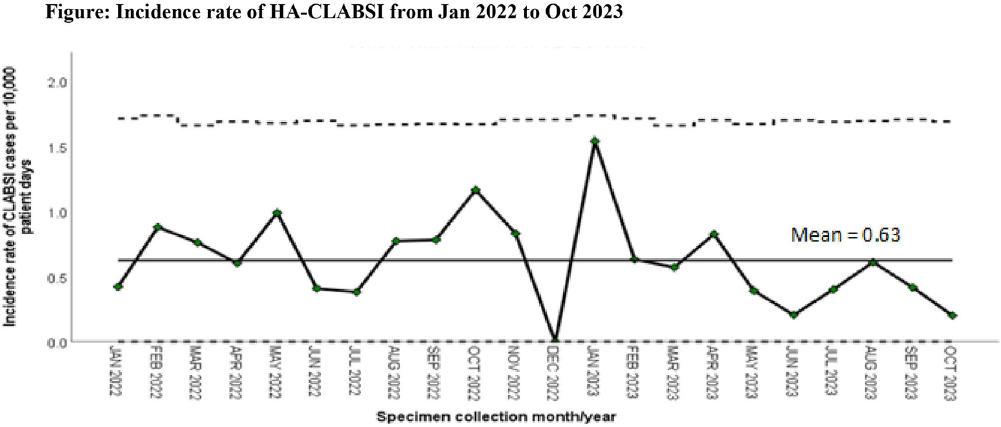
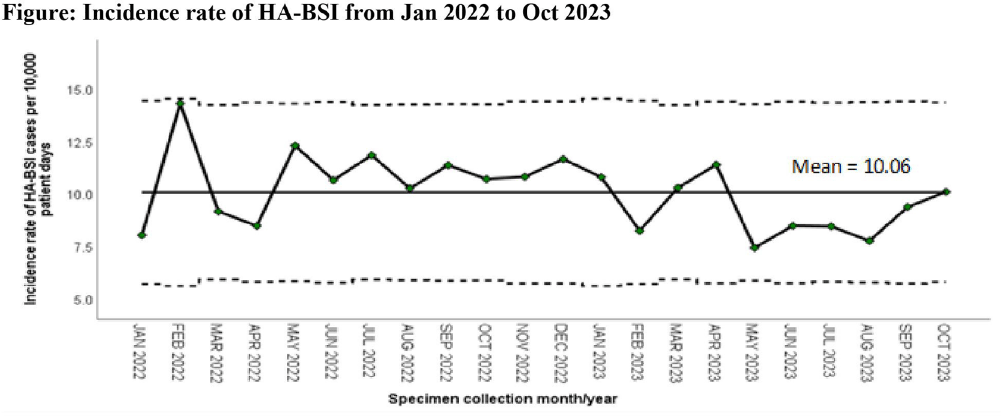
Background: Healthcare-associated central line associated bloodstream infection (HA-CLABSI) surveillance is important for monitoring healthcare-associated infections (HAIs) and evaluating effectiveness of infection prevention (IP) measures. However, implementing it is a laborious and time-consuming approach. Exclusive focus on central lines neglects HAI risk due to peripheral vascular catheters. This study aimed to assess whether HA-CLABSI incidence could be inferred from HA-bloodstream infection (BSI) trends and explore shift to HA-BSI surveillance. Methods: The study was performed in a Singaporean tertiary care hospital. Electronic medical records review was performed to determine whether positive blood cultures met Centers for Disease Control/National Health Safety Network (CDC/NHSN) definitions for HA-CLABSI and HA-BSI. Incident episodes of HA-BSI were included (excluding positive cultures repeated within 14 days). Incident organisms were explored to identify common causative pathogens (excluding same organisms isolated from cultures repeated within 14 days). CLABSI and BSI occurring ≥72hrs after admission were considered healthcare-associated. Patients under oncology or hematology service were considered immunocompromised. Incidence rates (IR) per 10,000 patient-days, patient characteristics and causative pathogens were compared between both indicators. Results: From January 2022 to October 2023, mean IR for HA-CLABSI was 0.63 (n=68) and for HA-BSI was 10.06 (n=1094). Median age of patients with HA-CLABSI was 66 years and HA-BSI was 68 years. HA-CLABSI and HA-BSI were more common in males (60.86% & 58.68%). Median duration between admission to HA-CLABSI was 20 days and to HA-BSI was 12 days. Median duration between central line insertion to HA-CLABSI was 16 days. Of 1094, 631 (57.7%) patients had vascular catheter(s) (i.e., IV cannula, port-a-cath, peripherally-inserted central catheter or central line) inserted at time of HA-BSI diagnosis, of whom 46 (7.3%) patients had CLABSI ±2days from positive blood culture. There was no significant correlation between monthly aggregate data from these indicators (Spearman’s correlation coefficient= 0.36, p-value=0.1). Predominant organisms causing HA-CLABSI and HA-BSI were gram negative bacteria (GNB, 40% & 57.21%), gram positive bacteria (24.71% & 22.23%), and fungi. Common GNB in CLABSI patients were Pseudomonas spp. and Stenotrophomonas maltophilia (8.24%), followed by Serratia marcescens and Klebsiella pneumoniae (5.88%). The frequent GNB in HA-BSI patients were Escherichia coli (15.4%), Klebsiella pneumonia (12.68%), and Pseudomonas spp. (6.69%). Common multi-drug resistant organisms were vancomycin-resistant Enterococcus faecium (10.59% & 3.69%) and methicillin-resistant Staphylococcus aureus (10.59% & 3.07%). Conclusion: HA-BSI did not correlate with HA-CLABSI. HA-BSI reflects heterogenous population outcomes. For utilization as surveillance indicator, further assessment on exclusion criteria is required to improve specificity.




Factors associated with clinician willingness to adopt HPV self-sampling and self-testing for cervical cancer screening
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e118
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Health Equity Factors and Healthcare-Associated Infections in Louisiana Facilities, 2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s17
-
- Article
-
- You have access
- Open access
- Export citation
Impact of Stewardship Pharmacist Driven MRSA Nasal Surveillance and De-escalation of Anti-MRSA Therapy
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s44
-
- Article
-
- You have access
- Open access
- Export citation
Implications of high-resolution velocity and strain rate observations for modelling of Greenlandic tidewater glaciers
-
- Journal:
- Journal of Glaciology / Volume 70 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e17
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of Vascular Access Teams on Central Line Associated Bloodstream Infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s11
-
- Article
-
- You have access
- Open access
- Export citation
-
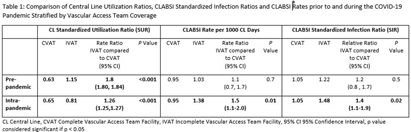
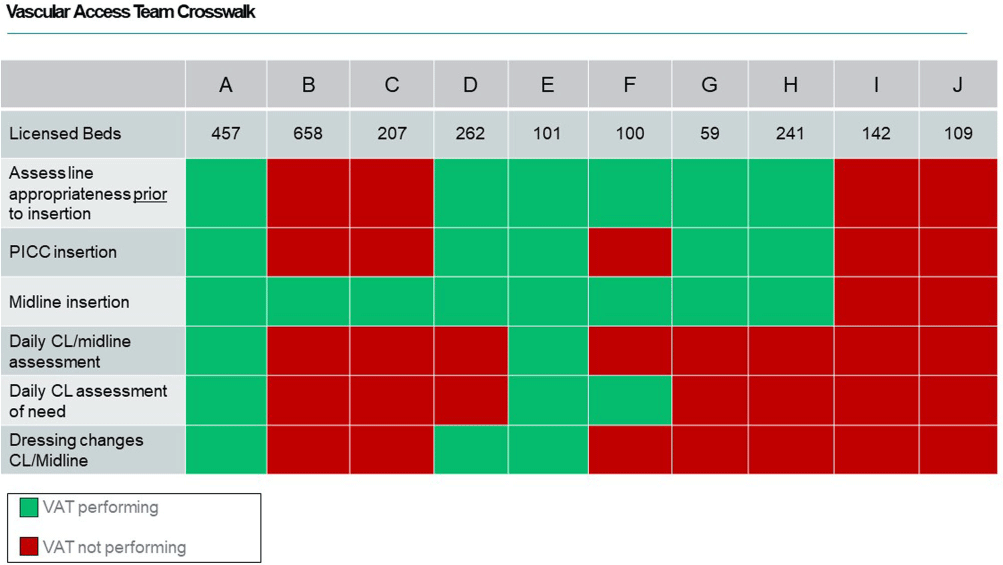
Background: During the COVID-19 pandemic, rates of central line bloodstream infections (CLABSI) increased nationally. Studies pre-pandemic showed improved CLABSI rates with implementation of a standardized vascular access team (VAT).[PL1] [PL2] [mi3] Varying VAT resources and coverage existed in our 10 acute care facilities (ACF) prior to and during the pandemic. VAT scope also varied in 1) process for line selection during initial placement, 2) ability to place a peripherally inserted central catheter (PICC), midline or ultrasound-guided peripheral IV in patients with difficult vascular access, 3) ownership of daily assessment of central line (CL) necessity, and 4) routine CL dressing changes. We aimed to define and implement the ideal VAT structure and evaluate the impact on CLABSI standardized infection ratios (SIR) and rates prior to and during the pandemic. Methods: A multidisciplinary workgroup including representatives from nursing, infection prevention, and vascular access was formed to understand the current state of VAT responsibilities across all ACFs. The group identified key responsibilities a VAT should conduct to aid in CLABSI prevention. Complete VAT coverage[mi4] was defined as the ability to conduct the identified responsibilities daily. We compared the SIR and CLABSI rates between hospitals who had complete VAT (CVAT) coverage to hospitals with incomplete VAT (IVAT) coverage. Given this work occurred during the pandemic, we further stratified our analysis based on a time frame prior to the pandemic (1/2015 – 12/2019) and intra-pandemic (1/2020 - 12/2022). Results: The multidisciplinary team identified 6 key components of complete VAT coverage: Assessment for appropriate line selection prior to insertion, ability to insert PICC and midlines, daily CL and midline care and maintenance assessments, daily assessment of necessity for CL, and weekly dressing changes for CL and midlines[NA5] . A cross walk of VAT scope (Figure 1) was performed in October 2022 which revealed two facilities (A and E) which met CVAT criteria. Pre-pandemic, while IVAT CLABSI rates and SIR were higher than in CVAT units, the difference was not statistically significant. During the pandemic, however, CLABSI rates and SIR were 40-50% higher in IVAT compared to CVAT facilities (Incident Rate Ratio 1.5, 95% CI 1.1-2.0 and SIR Relative Ratio 1.4, 95% CI1.1-1.9 respectively) (Table 1). Conclusions: CLABSI rates were lower in facilities with complete VAT coverage prior to and during the COVID-19 pandemic suggesting a highly functioning VAT can aid in preventing CLABSIs, especially when a healthcare system is stressed and resources are limited.


An Examination of Racial/Ethnic Differences in the Antibiotic Treatment of Community Acquired Pneumonia
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s23
-
- Article
-
- You have access
- Open access
- Export citation
S. aureus Surveillance and Decolonization Associated with Decreased MRSA, but not MSSA, Infections in the Neonatal ICU
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s117-s118
-
- Article
-
- You have access
- Open access
- Export citation
-
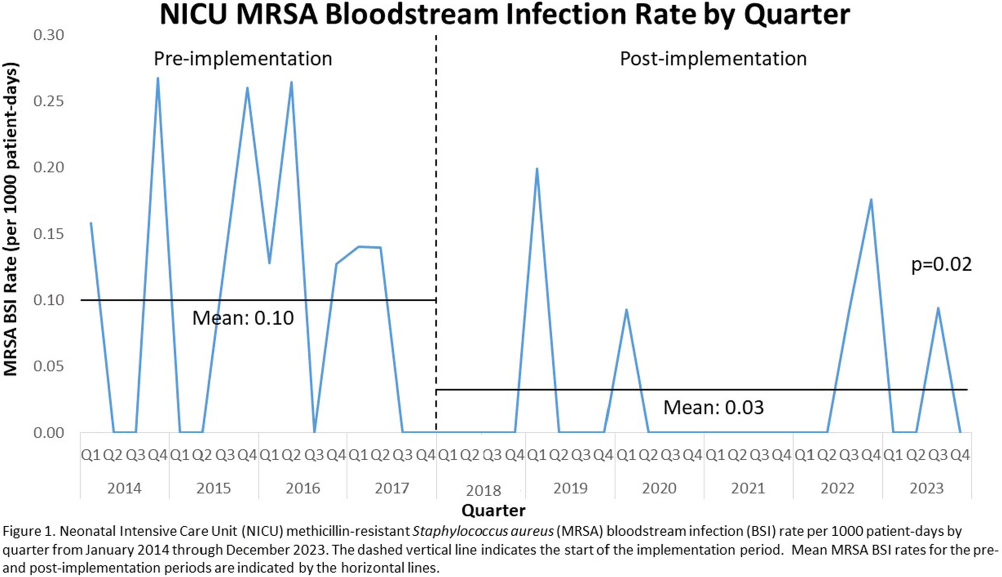
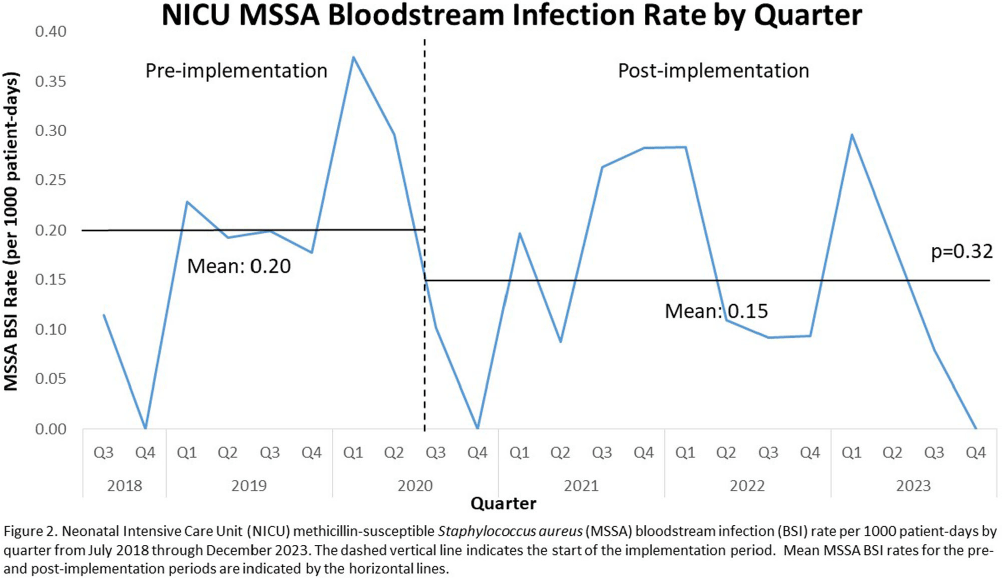
Background: Invasive Staphylococcus aureus infections cause significant morbidity and mortality in neonatal intensive care unit (NICU) infants.1 Colonization (asymptomatic carriage in the nose, skin, or gut) is a risk factor for subsequent invasive infection (e.g., pneumonia, bone infections, bloodstream infections, etc.). Active surveillance and decolonization measures for S. aureus-colonized infants have been associated with decreased invasive infection rates. 2-4 Methods: A methicillin-resistant S. aureus (MRSA) surveillance and decolonization program, consisting of admission and weekly MRSA nasal cultures followed by intranasal mupirocin plus chlorhexidine baths for colonized infants, was implemented in our level IV NICU with 150 beds in 2006.5 Due to poor compliance with decolonization protocols5, existing practices were reviewed and multiple interventions to increase compliance were implemented in 2018. These renewed efforts included revision of the existing MRSA decolonization protocol, updating the associated electronic medical record order set, re-education of unit staff, and weekly review by the Infection Prevention (IP) and NICU leadership teams to ensure the decolonization protocol was followed for newly colonized infants. Mean MRSA bloodstream infection (BSI) rates were calculated quarterly pre- (January 2014-December 2017) and post- (January 2018-December 2023) implementation of renewed efforts and compared via unpaired t-test. In July 2020 a similar methicillin-susceptible S. aureus (MSSA) surveillance and decolonization program was implemented with an associated revision of existing documents, education campaign, and weekly review of infants with new MSSA colonization. Mean MSSA BSI rates pre- (July 2018-June 2020) and post- (July 2020-December 2023) implementation were compared via unpaired t-test. Results: Renewed implementation of MRSA surveillance and decolonization was associated with a sustained decrease in the mean MRSA BSI rate (Figure 1): 0.10 per 1000 patient-days pre-implementation, 0.03 post-implementation (p=0.02). Following implementation of MSSA surveillance and decolonization, there was no statistically significant change in the mean MSSA BSI rate (Figure 2): 0.20 per 1000 patient-days pre-implementation, 0.15 post-implementation (p=0.32). Conclusions: Implementation of a robust MRSA surveillance and decolonization program in the NICU was associated with a sustained decrease in invasive MRSA infections. No change in invasive MSSA infection rates was observed following implementation of a similar protocol for MSSA. Additional research is needed to better understand the role of MSSA surveillance and decolonization in the NICU.
References: 1. Ericson, J.E., et al., JAMA Pediatr, 2015. 2. Popoola, V.O., et al., ICHE, 2016. 3. Kotloff, K.L., et al., Pediatrics, 2019. 4. Voskertchian, A., et al., ICHE, 2018. 5. Reich, P.J., et al. Clin Microbiol Infect, 2016.


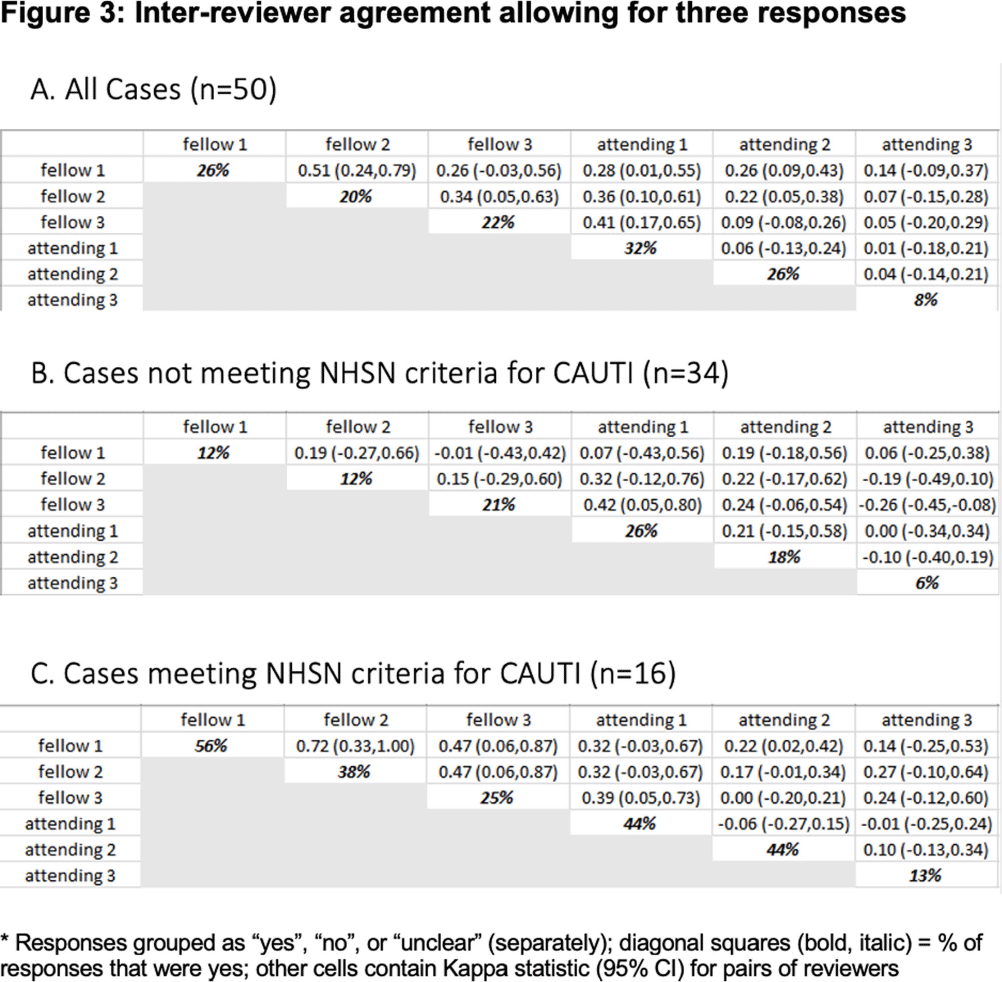
Inter-rater agreement of CAUTI (catheter-associated urinary tract infections) diagnosis among Infectious disease physicians
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s70-s71
-
- Article
-
- You have access
- Open access
- Export citation
-
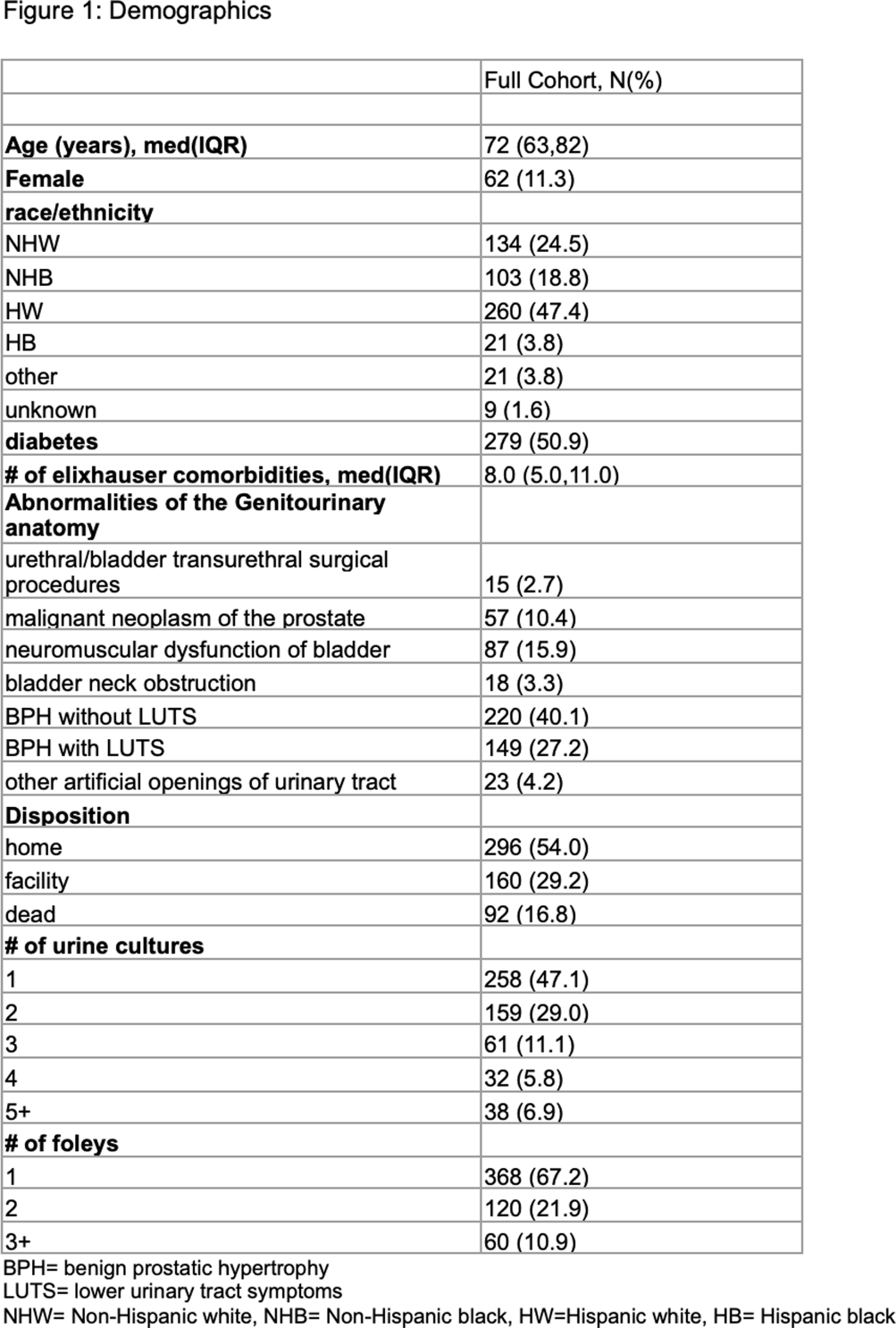
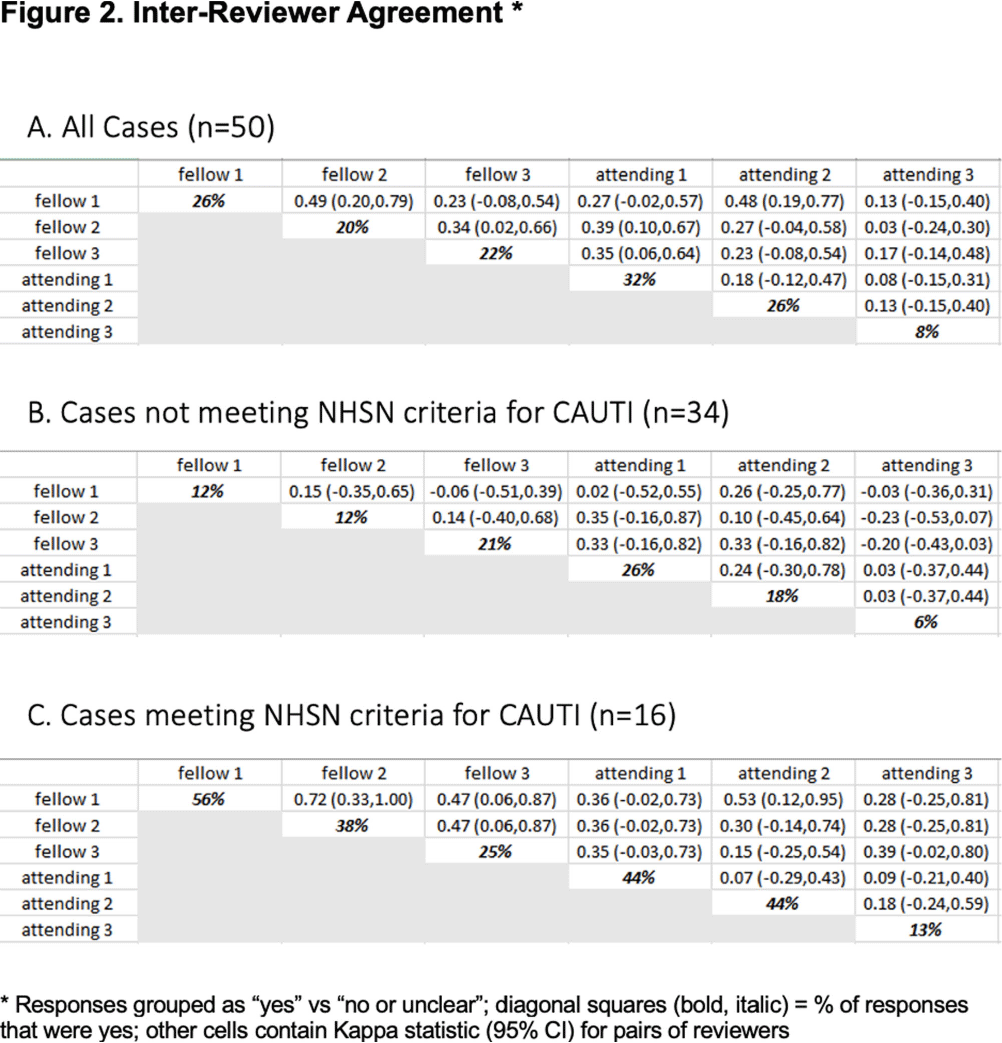
Background: CAUTIs constitute forty percent of nosocomial infections, yet their direct link with mortality remains debated. In 2009, NHSN estimated the economic burden of CAUTIs in the U.S. to be over $340 million. Limited data exist on inter-physician concordance in diagnosing CAUTIs, especially in patients with abnormal genitourinary (GU) anatomy. Our study assessed inter-provider variability in diagnosing CAUTI in 50 such patients, including those meeting NHSN(National healthcare safety network) criteria. Methods: We included a random set of 50 adults (18+) with abnormal GU anatomy admitted to the University of Miami hospitals from January 2018 to November 2021 who had a urinary foley catheter and at least one positive urine culture during their hospitalization. Three Infectious disease fellows and three board-certified Infectious disease physicians independently reviewed each patient’s chart, classifying them as having or not having a CAUTI. Inter-physician reliability was assessed using kappa statistics. Results: Our findings highlight substantial variation in clinician-determined CAUTI incidence among the 50 patients with abnormal GU anatomy, ranging from 8% to 32% (Figures 2,3). Inter-rater agreement on CAUTI diagnosis was generally poor (Kappa Hollenbeak CS, et al. The attributable cost of catheter-associated urinary tract infections in the United States: A systematic review. Am J Infect Control. 2018 Jul;46(7):751-757. Trautner BW, et al. Development and validation of an algorithm to recalibrate mental models and reduce diagnostic errors associated with catheter-associated bacteriuria. BMC Med Inform Decis Mak. 2013 Apr 15;13:48. Gafary M, et al. Catheter Associated Urinary Tract Infections (CAUTI) in Bladder Cancer Patients Post Cystectomy With a Neobladder, Open Forum Infectious Diseases, Volume 2, Issue suppl_1, December 2015, 293.



It Takes a Village: Leveraging a Multidisciplinary Team and Technology for Urine Culturing Stewardship
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s82-s83
-
- Article
-
- You have access
- Open access
- Export citation
-
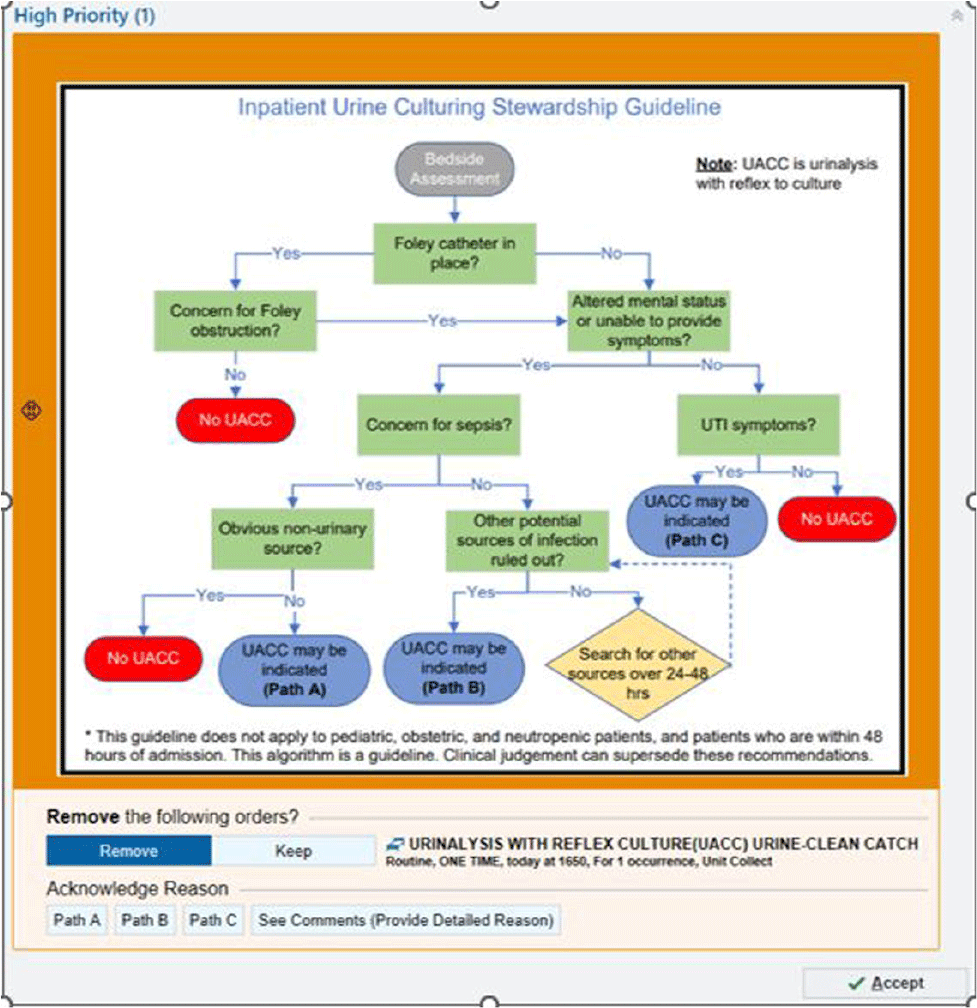
Background: Patients without urinary tract infection (UTI) symptoms but with a positive urine culture are considered to have asymptomatic bacteriuria (ASB). This often represents colonization and treatment is not recommended or clinically beneficial. Treatment of ASB can promote antimicrobial resistance and increased rates of Clostriodies difficile infections. Many cases of ASB are incorrectly assigned as CAUTIs due to over-culturing practices. We hypothesized that a urine culture algorithm, embedded within a best practice alert (BPA) in the electronic medical record (EMR), would reduce urine culturing practices for ASB. Methods: From Feb 2022 through May 2023, a multidisciplinary team implemented an Inpatient Urine Culturing Stewardship Guideline. A BPA fired when a provider placed a urinalysis with reflex to culture (UACC) or urine culture (UC) order for patients who met criteria (Image 1). The BPA directed providers to remove the order, select the appropriate pathway from the guideline, or provide a rationale for placing the order. The intervention was piloted on three intensive care units and two progressive care units, containing both medical and surgical patients. Monthly ordering practices, CAUTI rates, and gram-negative rod (GNR) bacteremia rates from a 13-month pre-intervention baseline period were compared to a 16-month intervention period. Over the same time periods, we also assessed changes in ordering practices for comparison units which did not implement the intervention. Pre-and-post intervention cohorts were analyzed using median two sample tests and Exact Poison Method, as appropriate. Results: On intervention units there was a 41.0% reduction in the median number of UACC and UC orders per 1000 patient days from 16.31 during the baseline period to 9.62 in the intervention period (p=0.0036). Pan cultures per 1000 patient days in which one of the orders was a UACC or UC fell by 42.2% from a median of 10.20 per 1000 patient days to 5.90 (p=0.0008). The comparison units saw no significant reductions in UACC and UC orders (p=0.21) or pan cultures (p=1.0). On the intervention units, the CAUTI rate for the baseline period was 1.31 per 1000 catheter days versus 0.79 in the intervention period (IRR = 1.65; p=0.44). GNR bacteremias remained stable on the intervention units between the baseline and intervention periods (p=0.82). Conclusion: This multidisciplinary intervention, leveraging EMR clinical decision support, reduced urine and pan culturing practices while demonstrating a trend towards a reduced CAUTI rate. The prevalence of GNR bacteremias remained consistent with baseline levels, suggesting the intervention did not cause harm.