Refine listing
Actions for selected content:
142351 results in Open Access
Molecular and Epidemiological Characterization of Pediatric and Adult C. difficile Infection in Canadian Hospitals, 2015-2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s10-s11
-
- Article
-
- You have access
- Open access
- Export citation
-
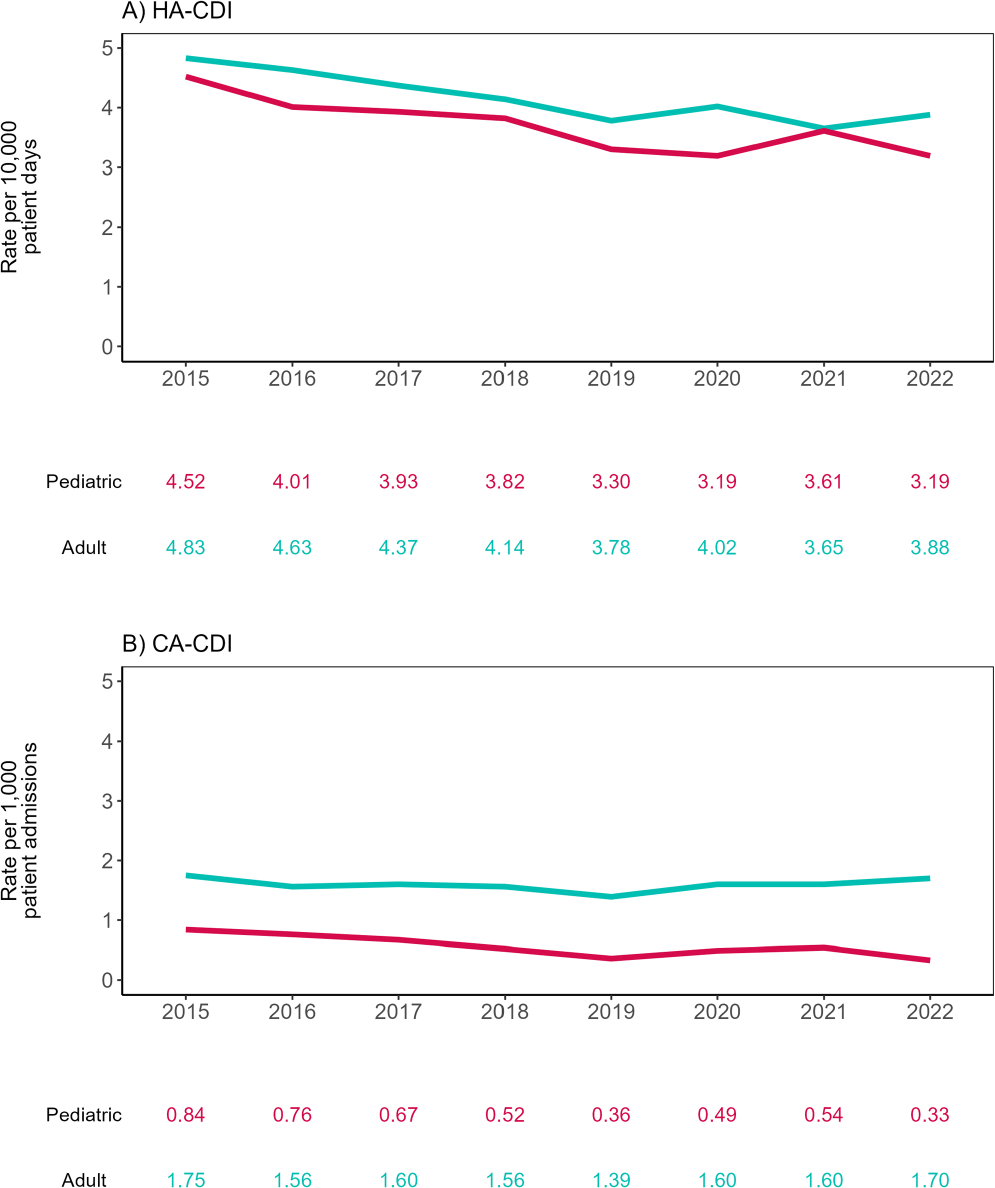
Background: The molecular and epidemiological landscape of C. difficile infection (CDI) has evolved markedly in the last decade; however, limited information is available contrasting differences between adult and pediatric populations. We describe a multicenter study evaluating healthcare-associated (HA) and community-associated (CA) adult and pediatric-CDI identified in the Canadian Nosocomial Infection Surveillance Program (CNISP) network from 2015 to 2022. Methods: Hospitalized patients with CDI were identified from up to 84 hospitals between 2015–2022 using standardized case definitions. Cases were confirmed by PCR, cultured, and further characterized using ribotyping and E-test. We used two-tailed tests for significance (p≤0.05). Results: Of 30,817 cases reported, 29,245 were adult cases [HA-CDI (73.2%), CA-CDI (26.8%)] and 1,572 were pediatric cases [HA-CDI (77.7%), CA-CDI (22.3%)]. From 2015 to 2022, HA-CDI rates decreased 19.7% (p=0.007) and 29.4% (p=0.004) in adult and pediatric populations, respectively (Figure 1). CA-CDI rates remained relatively stable in the adult population (p=0.797), while decreasing 60.7% in the pediatric population (p=0.013). Median ages of adult and pediatric patients were 70 (interquartile range (IQR), 58–80) and seven (IQR, 3–13) years, respectively. Thirty-day all-cause mortality was significantly higher among adult vs. Pediatric CDI patients (11.0% vs 1.4%, p < 0.0001). No significant differences in other severe outcomes were found. Ribotyping and susceptibility data were available for 4,620 samples: 3,558 adult (77.0%) and 1,062 pediatric (23.0%). The predominant adult and pediatric ribotypes (RT) were 106 (12.2/16.2%), 027 (11.4/3.2%), and 014 (8.8/8.2%). Overall, RT027 prevalence significantly decreased from 17.9% in 2015 to 3.2% in 2022 (p=0.003), while RT106 increased from 8.5% to 14.4%. Resistance rates among adult and pediatric isolates were similar for all antimicrobials tested except moxifloxacin (16.2% vs. 6.2%, p < 0.0001, respectively). Adult moxifloxacin resistance decreased from 30% to 6.3% from 2015 to 2022 (p=0.006). Adults with moxifloxacin-resistant CDI were older (median: 74 vs. 69 years, p < 0.001) and had higher thirty-day all-cause mortality (13% vs. 9.8%, p=0.041) and recurrence (10% vs. 5.7%, p < 0.001) compared to those with moxifloxacin non-resistant CDI, while these trends were not observed in pediatric patients. Among RT027 strains, moxifloxacin resistance decreased from 91.0% in 2015 to 7.1% in 2022. There was one metronidazole-resistant pediatric sample in 2018 and no resistance to vancomycin or tigecycline in either population. Conclusion: We have found differences in the epidemiological and molecular characteristics of adult and pediatric CDI, with higher thirty-day all-cause mortality among adults. Overall, RT106 has replaced RT027 as the predominant ribotype with a concomitant decrease in fluoroquinolone resistance.

The policy basis of group sentiments
-
- Journal:
- Political Science Research and Methods / Volume 13 / Issue 2 / April 2025
- Published online by Cambridge University Press:
- 16 September 2024, pp. 482-488
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Assessment of 19 Operation Room and Sterile Processing Units in Puerto Rico, 2023: Preliminary Findings using a new ICAR Tool
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s105-s106
-
- Article
-
- You have access
- Open access
- Export citation
Candida auris Screening of High-Risk Patients: A Descriptive Comparison of 2 Strategies.
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s147
-
- Article
-
- You have access
- Open access
- Export citation
Reduction in IUSS (Immediate Use Steam Sterilization) Associated with Reduction in Surgical Site Infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s89
-
- Article
-
- You have access
- Open access
- Export citation
Diagnostic Stewardship Opportunities for Emergency Department Evaluation of Children with Suspected Urinary Tract Infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s77
-
- Article
-
- You have access
- Open access
- Export citation

On the stability of fully nonlinear hydraulic-fall solutions to the forced water wave problem
-
- Journal:
- Journal of Fluid Mechanics / Volume 993 / 25 August 2024
- Published online by Cambridge University Press:
- 16 September 2024, A9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Traumatic stress in parents of children with congenital heart disease: a scoping review
-
- Journal:
- Cardiology in the Young / Volume 34 / Issue 8 / August 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 1622-1635
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impacts of Hospital Acquired Bloodstream Infections in Patients Undergoing Hemodialysis Through a Central Venous Catheter
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s73
-
- Article
-
- You have access
- Open access
- Export citation
Nationwide analysis of antimicrobial prescription in Korean hospitals between 2018 and 2021: The 2023 KONAS report
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s38-s40
-
- Article
-
- You have access
- Open access
- Export citation
-
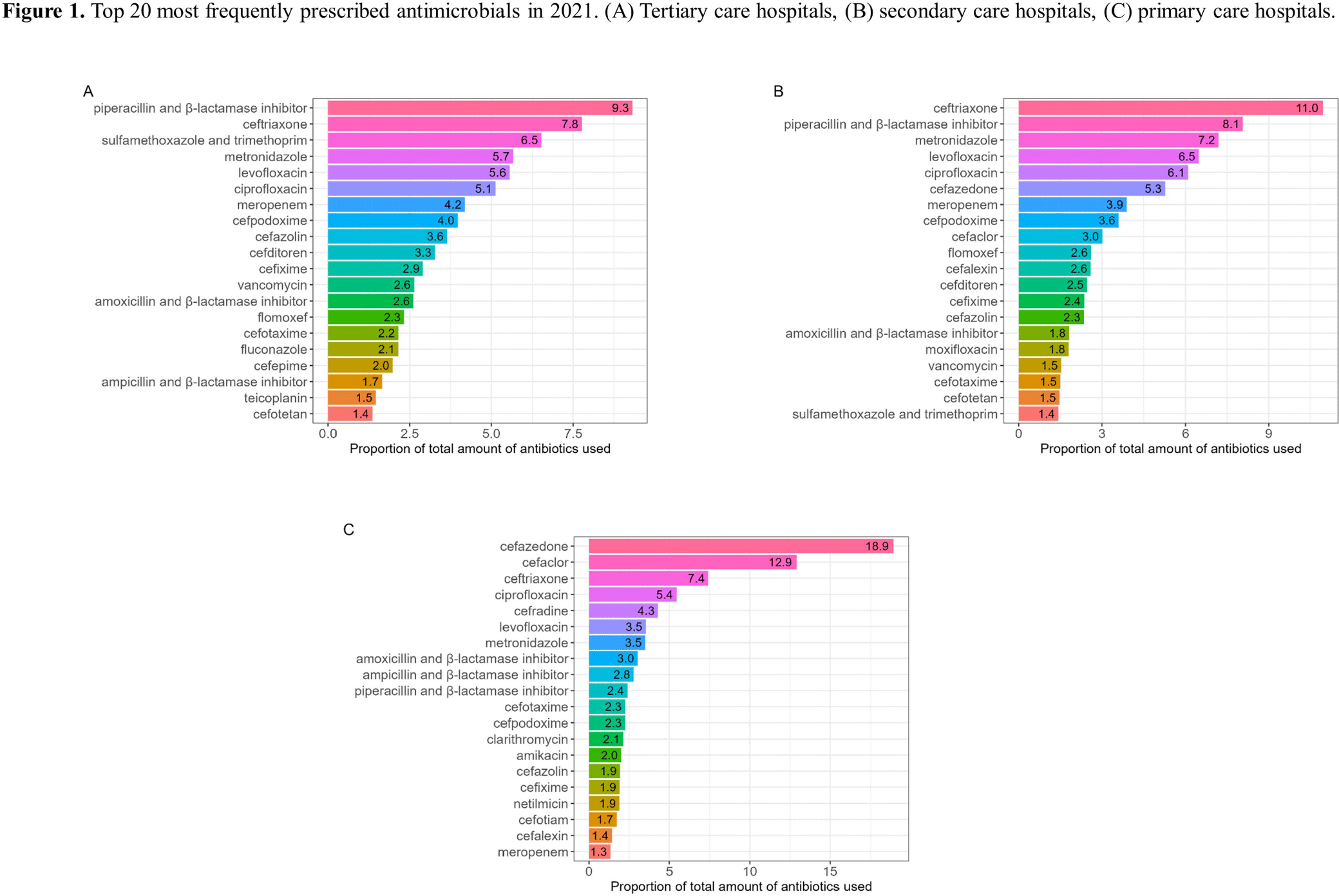
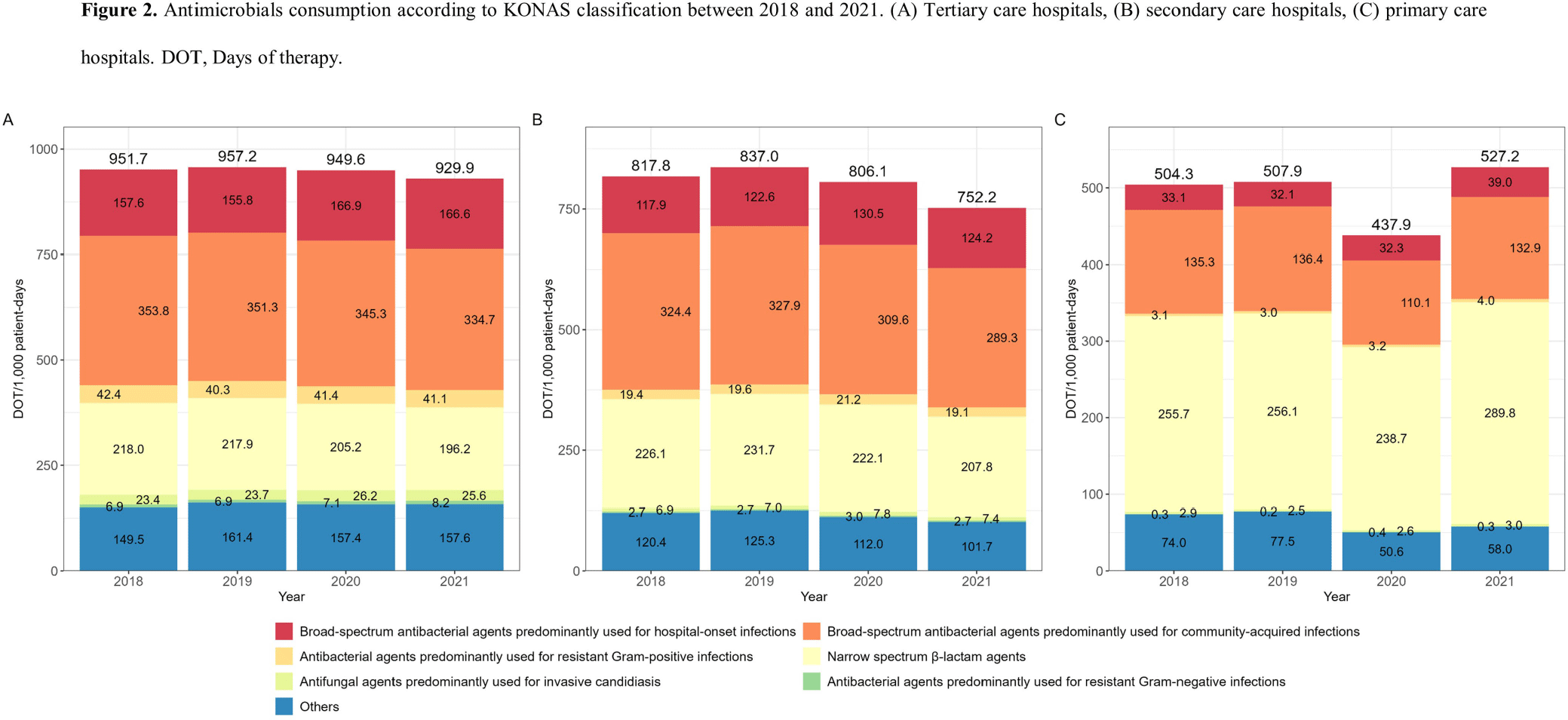
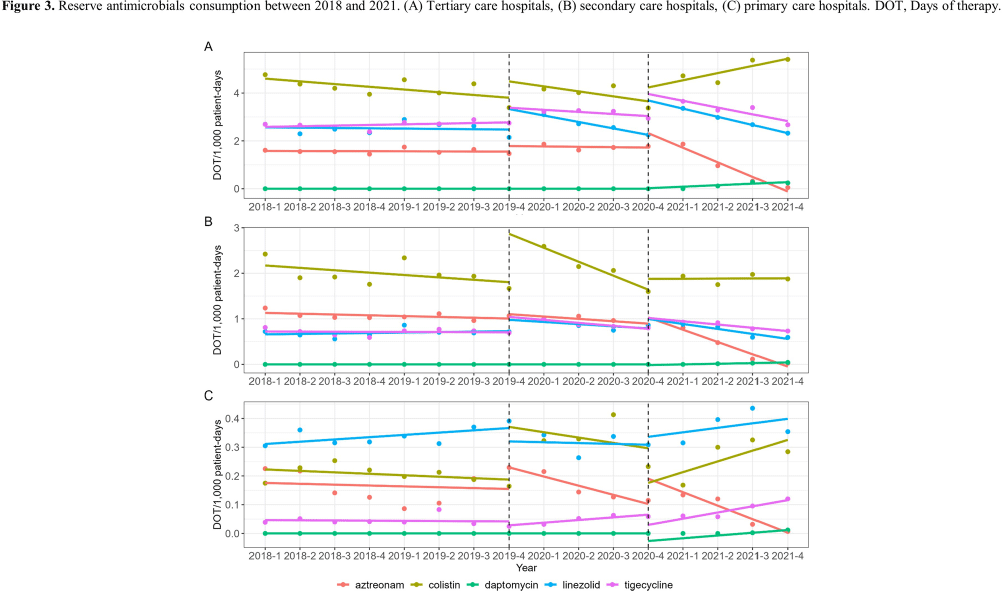
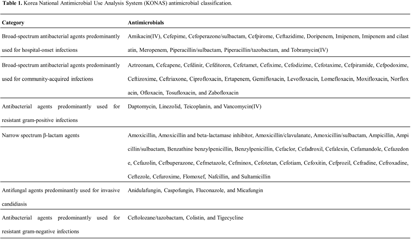
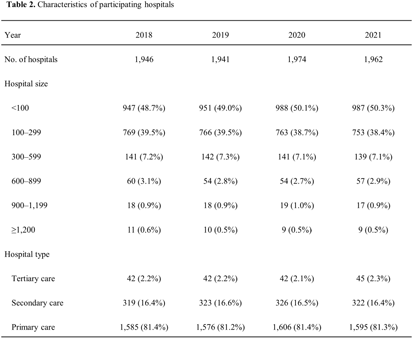
Background: Data on antimicrobial use at the national level is crucial to establish domestic antimicrobial stewardship policies and enable medical institutions to benchmark against each other. This study aimed to analyze antimicrobial use in Korean hospitals. Methods: We investigated the antimicrobials prescribed in Korean hospitals between 2018 and 2021, using data from the Health Insurance Review and Assessment. Primary care hospitals (PCHs), secondary care hospitals (SCHs), and tertiary care hospitals (TCHs) were included in this analysis. Antimicrobials were categorized according to the Korea National Antimicrobial Use Analysis System (KONAS) classification, which is suitable for measuring antimicrobial use in Korean hospitals. Results: Out of more than 1,900 hospitals, PCHs and TCHs represented the largest and lowest percentage of hospitals, respectively. The most frequently prescribed antimicrobial in 2021 was piperacillin/β-lactamase inhibitor (9.3%) in TCHs, ceftriaxone (11.0%) in SCHs, and cefazedone (18.9%) in PCHs. Between 2018 and 2021, the most used antimicrobial class according to the KONAS classification was ‘broad-spectrum antibacterial agents predominantly used for community-acquired infections’ in TCHs and SCHs, and 'narrow spectrum beta-lactam agents' in PCH. Total consumption of antimicrobials has decreased from 951.7 to 929.9 days of therapy (DOT)/1,000 patient-days in TCHs and from 817.8 to 752.2 DOT/1,000 patient-days in SCHs during study period, but not in PCHs (from 504.3 to 527.2 DOT/1,000 patient-days). Moreover, in 2021, while use of reserve antimicrobials has decreased from 13.6 to 10.7 DOT/1,000 patient-days in TCHs and from 4.6 to 3.3 DOT/1,000 patient-days in SCHs, it has increased from 0.7 to 0.8 DOT/1,000 patient-days in PCHs. Conclusion: This study confirms that antimicrobial use differs by hospital type in Korea. Recent increases of use of antimicrobials, including reserve antimicrobials, in PCHs reflect the challenges that must be addressed.





General practitioner and nurse experiences of type 2 diabetes management and prescribing in primary care: a qualitative review following the introduction of funded SGLT2i/GLP1RA medications in Aotearoa New Zealand
-
- Journal:
- Primary Health Care Research & Development / Volume 25 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e34
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
What is the dietary intake and nutritional status of defence members: a systematic literature review
-
- Journal:
- Nutrition Research Reviews / Volume 38 / Issue 1 / June 2025
- Published online by Cambridge University Press:
- 16 September 2024, pp. 267-281
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Setting the tone: the diffusion of moral and moral-emotional appeals across political and public discourse
-
- Journal:
- Political Science Research and Methods / Volume 13 / Issue 2 / April 2025
- Published online by Cambridge University Press:
- 16 September 2024, pp. 489-496
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Pangolin Universal Notching System: a scale-marking methodology for pangolins
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Qualitative Evaluation of an Antimicrobial Stewardship Tele-Mentoring Program in US Rural & Critical Access Hospitals
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s58-s59
-
- Article
-
- You have access
- Open access
- Export citation
-
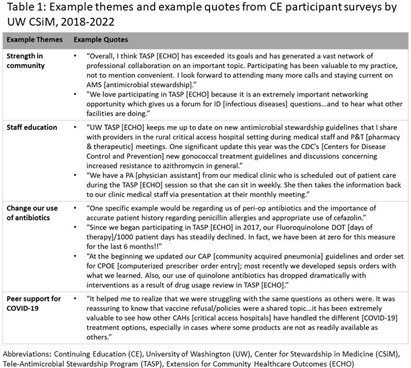
Background: The University of Washington (UW) Center for Stewardship in Medicine (CSiM) supports a tele-antimicrobial stewardship (AMS) program (TASP) using the ECHO approach (Extension for Community Healthcare Outcomes) in small, rural, and Critical Access Hospitals (primarily in the western U.S.) with education, mentoring, organizational capacity building, and a community of peers. To evaluate the continuing education (CE) component of UW-TASP ECHO, CSiM surveyed individuals receiving CE credits as part of the program. This survey was designed to track individuals’ satisfaction with the program and to assess the impact of UW-TASP ECHO on AMS in participating facilities. Methods: The CE participants’ survey was completed annually by individuals participating in UW TASP ECHO using online survey software. The survey included closed-ended and open-ended questions. Responses to open-ended questions were entered into Atlas.ti qualitative analysis software and coded iteratively according to themes that emerged. When a new code emerged partway through the coding process, earlier surveys were re-coded for the new code. Final codes were grouped into themes and sub-themes and quotes from each theme identified were summarized and attached to the theme and reported. Results: Data from three administrations of this survey were available: 2018-2019 (n=66); 2020-2021 (n=27); and 2021-2022 (n=30). These surveys were completed by a total of 95 individuals from 53 hospitals. Seven of these individuals completed a survey in each year, 14 completed a survey in two years, and 74 completed only one survey. Themes identified were COVID-19 support (including procedures and policies, being kept up-to-date, research summaries, and peer support), the antibiotic pocket guide developed by UW, strength in community, staff education, role of CSiM in developing/strengthening the AMS program at the facility, change in use of antibiotics, UW imprimatur, learning/growing as a healthcare provider, and importance for small, rural hospitals (see examples in Table 1). Conclusions: This qualitative analysis provides evidence from surveys of individuals participating in CE that UW TASP ECHO has had a meaningful impact in such domains as building a strong community among small, rural and critical access hospitals, educating staff, changing antibiotic use and providing peer support, among others.

Evaluation of a peer-led research best practices training for community health workers and promotoras
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e117
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Managerial Influence on Infection Prevention and Control (IPC) Implementation in Israeli Hospitals: A Doctoral Research Study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s102-s104
-
- Article
-
- You have access
- Open access
- Export citation
-
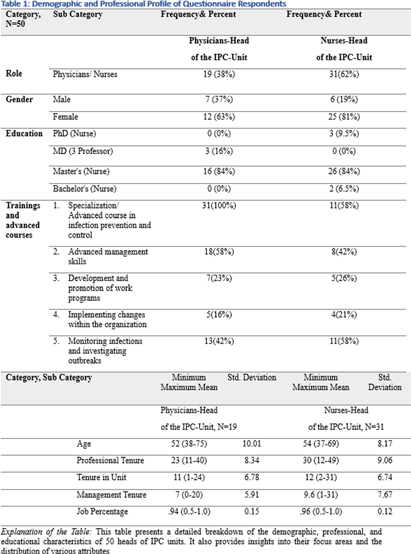
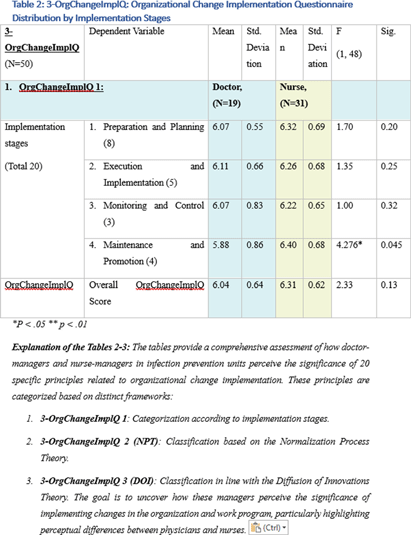
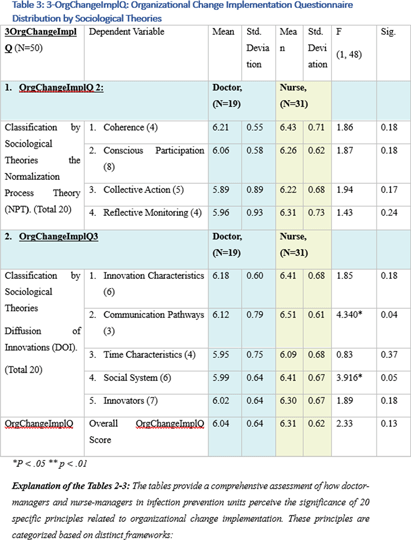
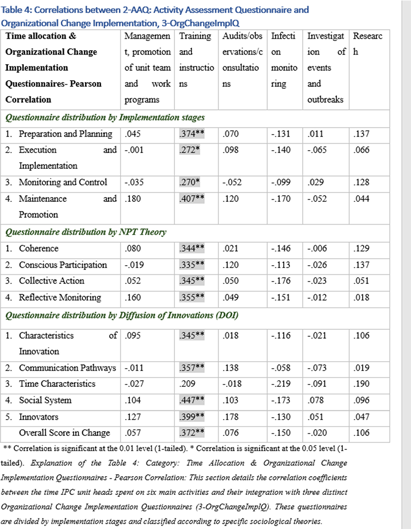
Background: This research, part of a doctoral study, aims to examine the impact of managerial factors on the implementation of Infection Prevention and Control (IPC) measures in Israeli hospitals. The study focuses on identifying key facilitators and barriers from the perspectives of physician and nurse managers, with an emphasis on understanding the integration of managerial strategies and theoretical frameworks in IPC implementation. Objective: The objective is to explore specific managerial factors, both facilitators and barriers, influencing the effective implementation of IPC measures. The research investigates these influences through the lens of physicians and nurses managing IPC units in public hospital settings. Methodology: A mixed-method approach was adopted, involving in-depth interviews with ten IPC-Unit managers (five physicians and five nurses) and a comprehensive questionnaire distributed among IPC-Unit heads. The study’s demographic and professional profiles of participants are detailed in Table 1. The data collection process encompassed an Activity Assessment Questionnaire (2-AAQ) and an Organizational Change Implementation Questionnaire (3-OrgChangeImplQ), with the distribution of responses categorized by implementation stages and sociological theories (Tables 2-4). Result: Managerial autonomy emerged as a significant catalyst for IPC implementation, with supportive leadership and resource allocation being critical. Differences in approaches between physician and nurse managers were observed, reflecting diverse strategies in planning, execution, monitoring, and maintenance of IPC measures. The findings also revealed a natural alignment with sociological theories, particularly Normalization Process Theory (NPT) and Diffusion of Innovations (DOI), despite a lack of formal training in these areas. Conclusions: The study underscores the multifaceted nature of IPC implementation, highlighting the importance of managerial autonomy, supportive leadership, and a deep understanding of organizational culture. The inherent alignment of IPC strategies with NPT and DOI theories suggests the potential of these frameworks in guiding IPC implementation. The research advocates for the integration of these theoretical perspectives into formal training programs to enhance the effectiveness of IPC measures in healthcare settings.




Environmental Fungal Contamination Characterization of Three Inpatient Units Utilizing Optimized Detection Methods
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s97-s98
-
- Article
-
- You have access
- Open access
- Export citation
-
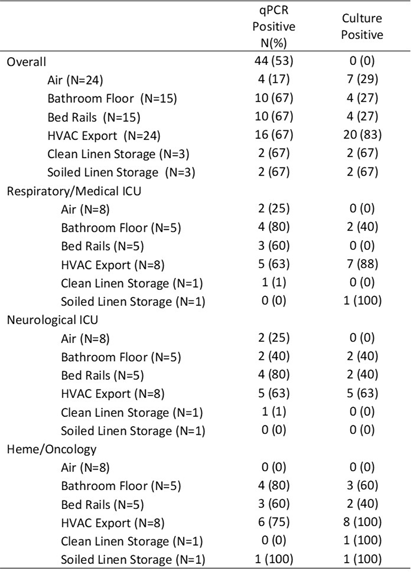
Background: Environmental sampling and detection methods for fungi in healthcare settings are not well-established. We previously refined methods for fungal sampling and detection in a controlled laboratory environment and aimed to validate them in a real-world healthcare setting. Methods: We performed a microbiological analysis of air and surfaces in three inpatient units at a tertiary care center. Surface samples were obtained with foam sponges from 3 locations in patient rooms (Patient bedrails, bathroom floor, HVAC export) and 5 locations in units (HVAC exports 3x, clean linen storage, soiled linen storage). Air samples were taken with an active air sampler directly below HVAC exports. Sponges were processed using the stomacher technique. Samples underwent DNA extraction followed by qPCR with FungiQuant primers targeting the 18S rRNA gene. Amplicons from positive samples were sequenced (NextSeq 1000, 300bp PE) and SmartGene databases were used to interpret sequence data. For comparison to culture methods, samples were also plated onto Sabouraud and HardyCHROM Candida + auris medias. Fungal growth underwent DNA extraction, 18S PCR and Sanger sequencing for genus and species identification. Results: A total of 85 samples were obtained, from 15 patient rooms and three units resulting in 61 surface and 24 air samples. Patients in study rooms had a median age of 53, 9 (60%) were male, and no patients had an invasive fungal infection during their hospital encounter. 44 (53%) and 39 (46%) samples were positive for fungi via qPCR and culture, respectively. Of the 44 positive qPCR samples, microbiome analyses identified at least one fungi to the species, genus and family levels in 43 (98%), 28 (64%), 18 (41%) samples, respectively (Table 1). 114 total isolates were identified of which the most common were Mallassezia restricta (30 [26%]), Malassezia globose (29 [25%]), and Pennicillium paradoxum (4 [4%]). 39 genera were identified of which the most common were Mucor (19 [49%]) and Candida (8 [21%]). Of the 39 culture positive samples, 90 total isolates were recovered. The most common species were Paradendryphiella arenariae (19 [21%]), Aspergillus niger (12 [13%]) and Penicillium commune (12 [13%]). Conclusion: These results demonstrate the presence of diverse fungal species in both air and surface samples across inpatient units. Higher sensitivity was noted utilizing qPCR, however, identified genera and species were markedly different between qPCR and culture methods. Larger studies are needed to assess the efficacy of qPCR for fungal detection in the healthcare environment.

Large-Scale S. aureus Screening with Molecular Epidemiology; the Role of MSSA and Community MRSA in Hospital Transmissions
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s15
-
- Article
-
- You have access
- Open access
- Export citation
The association between the timing of initial hepatitis B vaccination and seropositivity in healthcare personnel
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 11 / November 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 1347-1349
- Print publication:
- November 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
