Refine listing
Actions for selected content:
142352 results in Open Access
Aerosol optical depth disaggregation: toward global aerosol vertical profiles
-
- Journal:
- Environmental Data Science / Volume 3 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e16
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Occupational percutaneous injuries and exposures at a dental teaching institution from 2017 to 2023
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s120
-
- Article
-
- You have access
- Open access
- Export citation
-
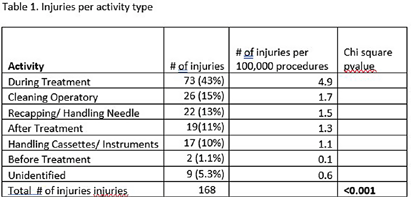
Background: All dental professionals face the risk of occupational percutaneous injuries and exposures. Previous studies have reported high incidents of percutaneous injuries among dentists. This study examined injury data over six years at a large teaching institution for trends to increase awareness and to design appropriate interventions to reduce injury rates. Method: Study injury data was collected for the department of employee and occupational health. The data was entered into an electronic incident reporting system from 2017-2023. Statistical analysis was performed with Openepi to determine injury trend by year and overall association by activity type. Result: There was a total of 168 injuries reported between 2017 and 2023. A majority of the injuries (54%) were caused by a needle or sutures followed by instruments at 41%. Most of the injuries (44%) occurred during treatment and while cleaning the surgical spaces at 15%. Only 13% of the injuries were attributed to handling or recapping needles. Chi-square test 0.2618 (p>.05) indicated there was no significant difference between years and number of injuries. Overall chi-square p ( < 0 .001) by activity type was significant indicating risk was not equal across all activities. Conclusion: Injuries declined during COVID-19 but soared back up in 2023. Needles, sutures, and instruments were the predominant source of injuries. Injuries occurred during treatment (43%), while cleaning the surgical space (15%) and while recapping or handling needles (13%). This study is the first step in understanding the trend and factors attributing to injuries to implement appropriate corrective actions. Further analysis should be conducted to identify specific procedures or clinical activities exposing employees to Occupational percutaneous injuries.

Perceptions on Penicillin Allergy Labels among Nurses and Prescribers in Three Pediatric Urgent Care Sites
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s45
-
- Article
-
- You have access
- Open access
- Export citation
-
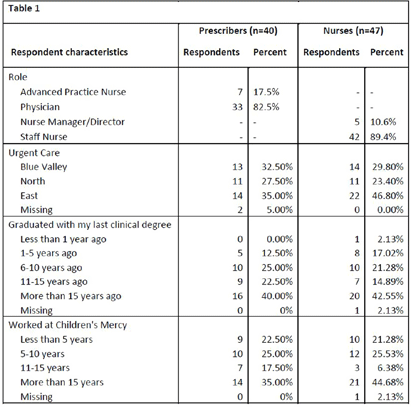
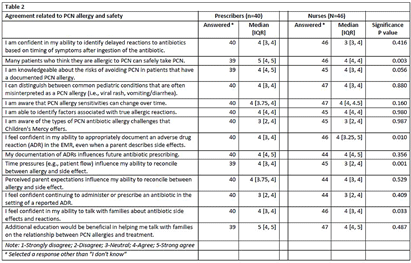
Background: National guidelines recommend penicillins (PCN) as first-line treatment for many common pediatric infections in the outpatient setting. Although less than 1% of the United States population has a true, IgE-mediated PCN-allergy, approximately 10% of patients are labeled with a PCN-allergy. Accurate adverse drug reaction (ADR) documentation plays an important role in this over-labeling. We have previously shown that nurses feel assessment and documentation of PCN-allergies are critical to their role. However, additional evidence purports nurse hesitancy to interrogate allergy accuracy or reclassify parent’s response to side effect. Our objective was to explore frontline clinicians’ confidence in assessing, documenting, and responding to PCN-allergy labels. Methods: To expose barriers and prioritize improvement ideas for a multidisciplinary quality improvement (QI) project aimed to improve PCN-allergy labeling in our pediatric urgent care clinics, we deployed this investigator-developed survey to prescribers and nurses. It’s comprised of 14-questions scored on a 5-point Likert scale (4 demographic, 4 PCN/safety, 3 allergy types, 4 allergy documentations, 3 treatment options), and 1 optional free-text. We used descriptive statistics to compare survey responses between prescribers and nurses and evaluated free text comments for themes. Results: Eighty-seven clinicians across 3 sites participated, with a response rate of 35%, with variation by sites (25.3% to 41.4%). Forty-one percent of (n=36) responders have been in practice >15 years and 40.2% (n=35) have worked at our hospital > 15 years (Table 1). Overall, perceived knowledge of PCN-allergies and safety was favorable (Table 2). Prescribers reported higher confidence with: 1) perceiving many patients who believe they are allergic to PCN can safety take PCN (prescribers median=5 [IQR: 4, 5] vs. nurses median=4 [4,4], p = 0.003); and 2) perceiving that time pressures influenced their ability to reconcile allergies and side effects (prescribers median=4 [4, 5] vs. nurses median=3 [2, 4], p = 0.001). Both prescribers and nurses reported lower confidence in continuing to administer or prescribe an antibiotic in the setting of a reported ADR. Thirteen respondents (15%) provided comments with specific requests for additional family education and practice guidance, including the referral process to subspecialty clinics for PCN-allergy testing. Conclusions: Our survey results identified barriers to accurate PCN-allergy labels, including knowledge on documentation, time pressures, hesitancy to challenge parent report, and uncertainty on referral process for PCN-allergy testing. This survey will inform future drivers for our QI. Opportunities include electronic medical record refinement, improving referrals to PCN-allergy de-labeling clinics, and the development of scripted education to guide family discussions.
Disclosure: Rana El Feghaly: Merck- grant funding. Amanda Nedved: Contracted Research – Merck


First Detected Transmission of C. auris within a Minnesota Healthcare Facility Following Exposure in the Emergency Department
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s92
-
- Article
-
- You have access
- Open access
- Export citation
Timesavers: Clinical Decision Support and Automation of MRSA and VRE Deisolation
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s114-s117
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Most healthcare facilities in the US apply contact precautions (CP) for patients with methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) infection and/or colonization. Most individuals with MRSA or VRE colonization will clear over time; however, frontline clinicians rarely evaluate for discontinuation of CP, resulting in increased burden on infection preventionists (IPs). Automation of time- and test-based evaluation using clinical decision support systems (CDSS) embedded in electronic health records (EHR) may increase evaluation and discontinuation of CP when appropriate, while preserving IP resources. Methods: This quality improvement initiative was implemented at Mass General Brigham (MGB), an integrated healthcare system, where patients with MRSA or VRE infection/colonization are identified in the EHR with a corresponding “infection status” and CP applied. Following MGB policy (Figure 1), CDSS features included: 1) automated time-based resolution from 2/15/2023-11/13/2023 and 2) automated ordering of screening assays for patients eligible for test-based evaluation from 6/20/2023-11/14/2023 (Figure 2). Counts of CP discontinuation and automated ordering were performed. IPs at one MGB facility performing manual review of patients self-recorded the time spent evaluating for CP discontinuation. Using these time reports, the average time to complete these tasks and the projected time savings were calculated over the implementation period. Results: Four IPs recorded the time to review patients for CP discontinuation, including reviewing recent antimicrobial administration, microbiology results, ordering screening test(s), and contacting the primary team. Twenty-five patient encounters were timed with a mean of 4.7 minutes documented per encounter. Over a 9-month period after initiation of the automated time-based resolution, the monthly mean number of patients with CP for MRSA and VRE which were automatically discontinued was 247 and 100, respectively. Projected IP time savings over the same 9-month period for MRSA and VRE were 174.1 and 70.5 hours, respectively. Over a 5-month period after initiation of automated ordering of MRSA polymerase chain reaction (PCR)/culture, as well as VRE culture for test-based evaluation, the monthly mean number of MRSA culture, MRSA PCR, and VRE culture automatically ordered for patients on CP for MRSA and VRE were 176, 24, and 145, respectively. Projected IP time savings over the same 5-month period for MRSA and VRE were 78.3 and 56.8 hours, respectively.
Conclusion: Healthcare systems that enhance their EHR with CDSS to automate CP evaluations may improve frontline clinician workflow, patient flow and bed capacity, while optimizing use of IP resources.




Bereavement guilt among young adults impacted by caregivers’ cancer: Associations with attachment style, experiential avoidance, and psychological flexibility
-
- Journal:
- Palliative & Supportive Care / Volume 22 / Issue 6 / December 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 1998-2006
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Understanding the fluvial capture of the Guadix-Baza Basin in SE Spain through its oldest exorheic deposits
-
- Journal:
- Quaternary Research / Volume 122 / November 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 106-121
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A comparison of the welfare of free-ranging native pony herds on common land with those used for conservation grazing in the UK
-
- Journal:
- Animal Welfare / Volume 33 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e30
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Trends of Early Onset Group B Streptococcus infections and Observed Racial and Geographic Disparities Associated with GBS Infections in Tennessee, 2005-2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s131-s132
-
- Article
-
- You have access
- Open access
- Export citation
Are there risk factors commonly observed on Australian farms where the welfare of livestock is poor?
-
- Journal:
- Animal Welfare / Volume 33 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e34
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Extended-Spectrum Beta-Lactamase Producing Enterobacterales Infections in the United States, 2012-2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s32-s33
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The 2022 Special Report: COVID-19 U.S. Impact on Antimicrobial Resistance identified continued increases in the rate of extended- spectrum beta-lactamase producing (ESBL) infections in the United States from 2017 through 2020. Using similar data sources and methodology, we examined the trends of species-specific ESBL infections from 2012-2021. Methods: We identified a cohort of patients from the PINC AI and BD Research Insights databases with a clinical culture yielding a Klebsiella pneumoniae or Escherichia coli isolate with accompanying susceptibility testing. E. coli or K. pneumoniae isolates non-susceptible to ceftriaxone, cefotaxime, ceftazidime, or cefepime were considered suggestive of ESBL production. Isolates from patients with no culture yielding the same resistance phenotype of interest in the previous 14 days were counted as an incident case. Community-onset (CO) cultures were obtained ≤ day 3 of hospitalization; hospital-onset (HO) cultures were obtained ≥ day 4. We used a raking procedure to determine weights for extrapolating the number of discharges included in our sample to match the distribution of discharges, stratified by bed size, U.S. census division, urban/rural designation, and teaching status, for U.S. hospitals included in the American Hospital Association survey. We evaluated rates over time due to the changes in number of hospitalizations during the COVID-19 pandemic. Results were stratified by HO and CO, and sterile and non-sterile specimen sources. Results: In 2021, there were 48,936 ESBL K. pneumoniae and 153,112 ESBL E. coli infections among approximately 32 million discharges. Overall, most infections were CO and from non-sterile specimens. From 2012-2021, the rate of ESBL K. pneumoniae increased from 9.54 to 15.28 per 10,000 discharges. ESBL E. coli infections increased from 2012-2020 (30.18 to 51.32 per 10,000 discharges), then declined in 2021 (47.81 per 10,000 discharges) (Table 1, Figure 1). The proportion of non-sterile ESBL E. coli declined from 88% in 2012 to 83% in 2021, and the proportion of non-sterile ESBL K. pneumoniae was 85-87% over the study period (Figure 2). Conclusion: ESBL E. coli and K. pneumoniae infections increased from 2012-2021, although the CO ESBL E. coli rate decreased between 2020 and 2021. Understanding changes in culturing practices over time may provide insights into the increased proportion of ESBL E. coli from sterile sites. Additionally, further investigation into differences in organism trends, particularly in 2021, may inform prevention strategies.






Informing synthetic passive microwave predictions through Bayesian deep learning with uncertainty decomposition
- Part of
-
- Journal:
- Environmental Data Science / Volume 3 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e17
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Moving Beyond the Reflex: Effect of a Clinical Decision Support Tool on Urine Culture Ordering Practices
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s84-s85
-
- Article
-
- You have access
- Open access
- Export citation
-
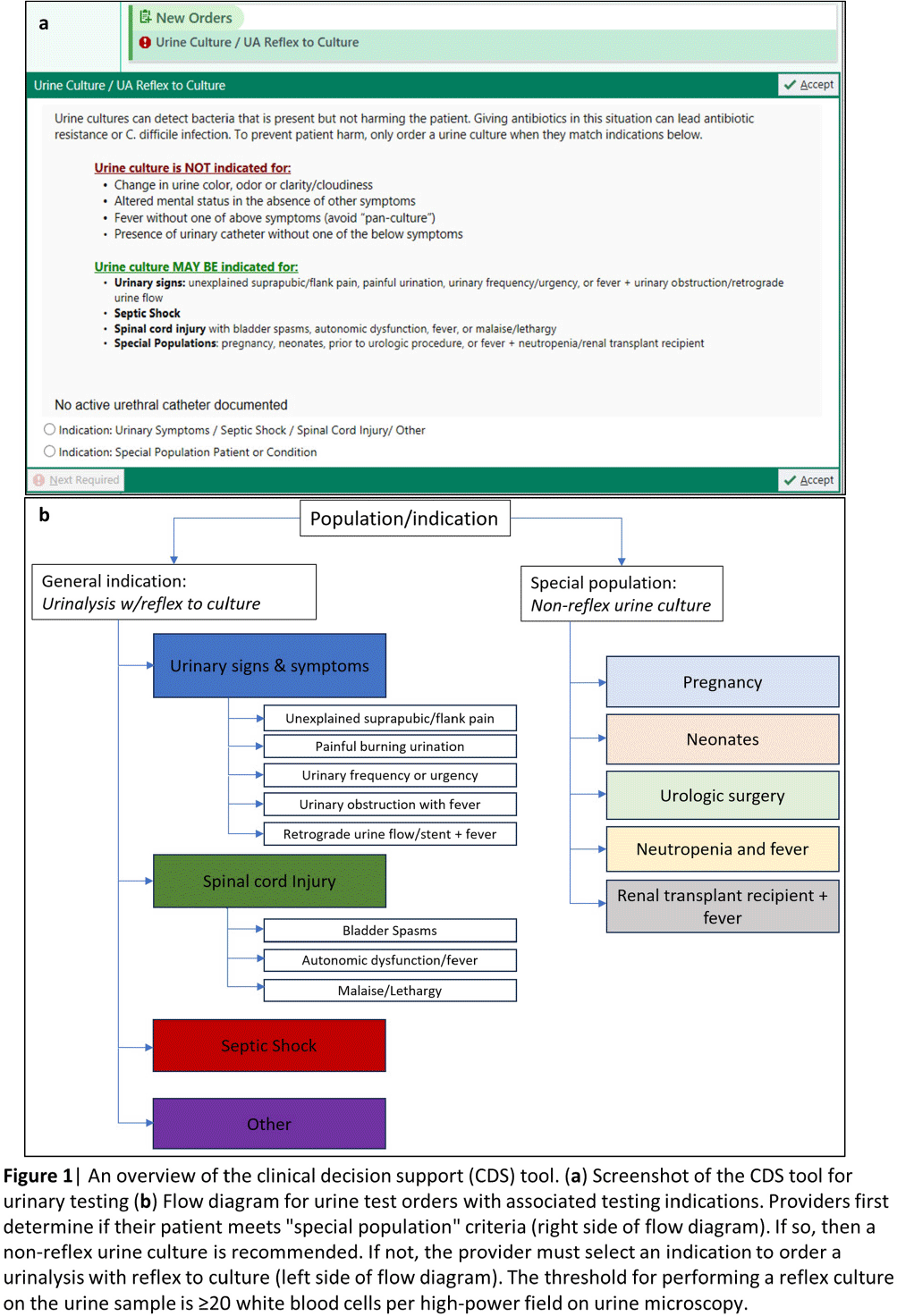
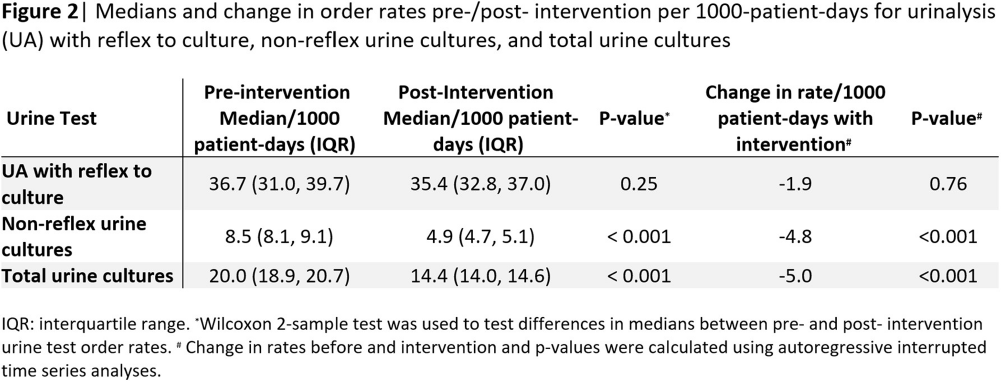
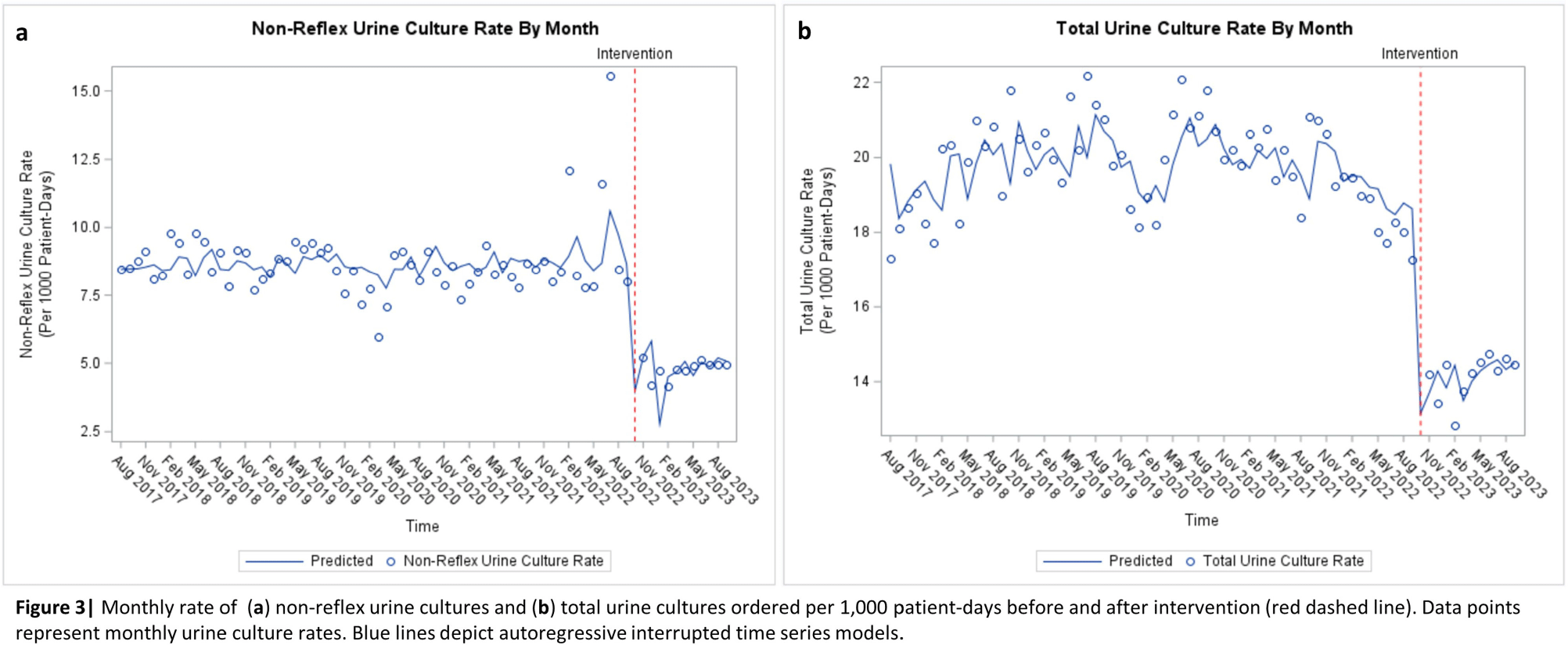
Background: Interventions targeting urine culture stewardship can improve diagnostic accuracy for urinary tract infections (UTI) and decrease inappropriate antibiotic treatment of asymptomatic bacteriuria. We aimed to determine if a clinical decision support (CDS) tool which provided guidance on and required documentation of the indications would decrease inappropriately ordered urine cultures in an academic healthcare network that already uses conditional (e.g. reflex) urine testing. Methods: In October 2022, four hospitals within one academic healthcare network transitioned to a new electronic health record (EHR). We developed an embedded CDS tool that provided guidance on ordering either a urinalysis (UA) with reflex to urine culture or a non-reflex urine culture (e.g. for pregnant patients) based on the indication for testing (Figure 1). We compared median monthly UA with reflex culture and non-reflex urine culture order rates pre- (8/2017–9/2022) and post- (10/2022–9/2023) intervention using the Wilcoxon rank-sum test. We used interrupted time-series analyses allowing a one-month time window for the intervention effect to assess changes in monthly UA with reflex culture, non-reflex urine culture, and total urine culture order rates associated with the intervention. Using SAS 9.4, we generated Durbin-Watson statistics to assess for autocorrelation and adjusted for this using a stepwise autoregressive model. Result: The median monthly UA with reflex culture order rates per 1000 patient-days were similar pre- and post- intervention at 36.7 (interquartile range [IQR]: 31.0–39.7) and 35.4 (IQR: 32.8–37.0), respectively (Figure 2). Non-reflex and total urine culture rates per 1000 patient-days decreased from 8.5 (IQR: 8.1–9.1) to 4.9 (IQR: 4.7–5.1) and from 20.0 (IQR: 18.9–20.7) to 14.4 (IQR: 14.0–14.6) post-intervention, respectively. Interrupted time-series analyses revealed that the intervention was associated with a decrease in the monthly non-reflex urine culture by 4.8 cultures/1000 patient-days (p< 0.001) and in the total urine culture monthly order rates by 5.0 cultures/ 1000 patient-days (p < 0 .001) [Figures 3a and b]. The UA with reflex order rate did not significantly change with the intervention (not pictured). Conclusion: In an academic healthcare network that already employed conditional urine testing, the implementation of an EHR-based diagnostic stewardship tool led to additional decreases in both non-reflex and total urine cultures ordered.



The Collective Responsibilities of Science: Toward a Normative Framework
-
- Journal:
- Philosophy of Science / Volume 92 / Issue 1 / January 2025
- Published online by Cambridge University Press:
- 16 September 2024, pp. 1-18
- Print publication:
- January 2025
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antimicrobial Stewardship Practice Changes Following a Statewide Educational Conference in Nebraska
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s37-s38
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: In 2023, Nebraska held its 4th state antimicrobial stewardship (AS) educational conference, an annual one-day in-person event with continuing education offered for nurses, pharmacists, microbiology lab technicians, and physicians. One challenge of educational events is determining if content has been translated into practice. We sought to assess AS-related practice changes implemented by conference attendees. Methods: Conference attendees were sent 2 surveys by email following the conference. Survey 1 questions were integrated into the continuing education credit evaluation immediately following the conference. Survey 2 was sent three months later to all registered attendees. Qualitative responses were grouped by theme and descriptive statistics were used to evaluate Results: There were 203 attendees from across the state including a diverse group of learners (Table 1) representing metropolitan and rural areas of Nebraska (Figure 1) from acute care hospitals, critical access hospitals, long-term care settings, and public health. A total of 148 attendees (73%) answered questions in Survey 1 (Table 2), and 79 (39%) attendees responded to Survey 2. On Survey 1, 94% of respondents indicated that they intended to make practice changes, though 60% anticipated barriers including further staff training needs and lack of resources and health system support. On Survey 2, 83% of respondents indicated successful implementation of practice changes at three months after the conference. The most common practice changes included enhanced communication strategies, improved antibiotic tracking, monitoring, and review, policy and procedure updates, and AS tool implementation. On Survey 1, 26% (35/131) strongly agreed that their ability to treat patients was adequate prior to the conference; this increased to 55% (72/131) post-conference. On Survey 2, 56% (22/39) of respondents reported improvement in patient outcomes because of implemented practice changes following conference attendance. However, some also mentioned a short follow-up survey timeline as a limitation in assessing patient outcome improvements. Reported outcomes included improved receptiveness from providers, patients, and families to antibiotic use recommendations, shorter prescribed durations, and more appropriate initial antibiotic selection. Improved team performance was noted by 73% (27/37) of respondents. Themes included improved communication with internal and external stakeholders, more collaborative team discussions, increased confidence in recommendations, expanded provider and staff engagement, and increased leadership involvement. Conclusions: In addition to improved knowledge and understanding for a variety of AS-related areas, attendees of the conference also reported a high rate of practice changes that led to perceived improvements in patient outcomes and team function.






In Pursuit of the Analytical Unit. Island Archaeology as a Case Study
-
- Journal:
- Cambridge Archaeological Journal / Volume 34 / Issue 4 / November 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 583-600
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Can Artificial Intelligence Support Infection Prevention and Control Consultations?
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s29-s30
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Artificial intelligence (AI) tools have demonstrated success in US medical licensing examinations; however, their utility in infection prevention and control (IPC) remains unknown. Methods: The program of hospital epidemiology handles consultation calls and records each question and answer. Using 2022 data, we selected 31 frequently asked questions. We utilized four AI tools, including Chat GPT-3.5 and 4.0, Bing AI, and OpenEvidence, to generate answers. We predefined scales (Table 1) to capture responses by three reviewers, including two hospital epidemiologists and one infection preventionist. The mean score of ≥ 3 and ≥ 4 was considered acceptable in accuracy and completeness, respectively. We reported the percentage of responses with acceptable accuracy and completeness out of assessed questions for each category. Results: Among 31 questions, 16 were associated with isolation duration, 9 with healthcare personnel (HCP) exposure, 4 with cleaning contaminated rooms, and 2 with patient exposure. Regarding accuracy, most AI tools performed worse in questions about isolation duration, ranging between 75% and 93.8%. All AI tools, except OpenEvidence, had a 100% accuracy rate for HCP and patient exposure. All AI tools had a 100% accuracy rate for contaminated room handling. The highest overall acceptable accuracy rate was observed in Chat GPT-3.5. Regarding completeness, most AI tools performed worse in questions about isolation duration, ranging between 44% and 75%. All AI tools, except OpenEvidence, had a 100% completeness rate for contaminated rooms and patient exposure. The highest overall acceptable completeness rate was observed in Bing AI (Table 2). Conclusions: All AI tools provided reasonable answers to commonly asked IPC-related questions, although, there were variations among different tools used. AI could be used to supplement the infection control program, especially if resources are limited.




Teachers’ Perceptions of Formative Assessment for Students With Disability: A Case Study From India
- Part of
-
- Journal:
- Australasian Journal of Special and Inclusive Education / Volume 48 / Issue 2 / December 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 122-135
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
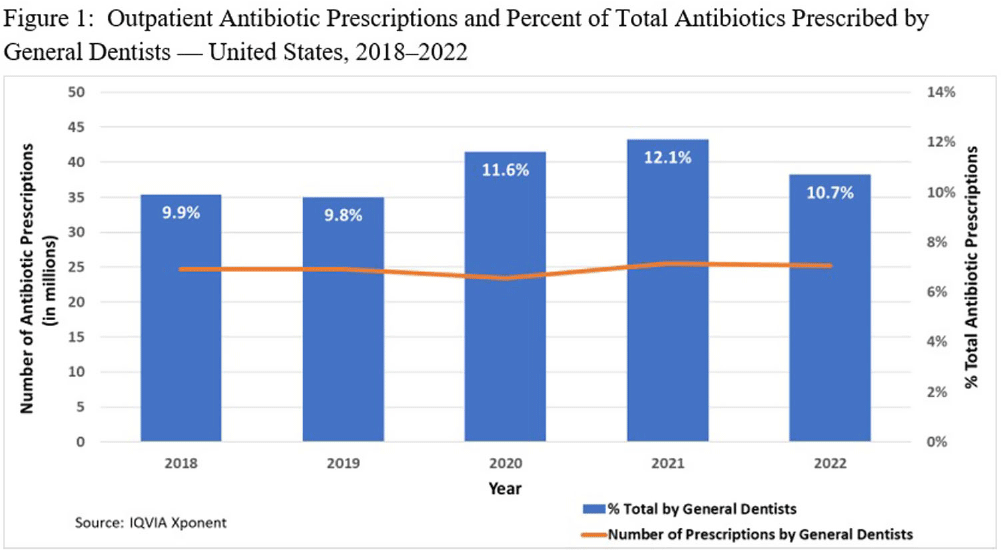
Antibiotic Prescribing by General Dentists in the Outpatient Setting — United States, 2018–2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s22-s23
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Inappropriate antibiotic use impacts patient safety and antimicrobial resistance patterns. In 2013, general dentists in the U.S. prescribed nearly 10% of all outpatient oral antibiotics (24.5 million prescriptions). The American Dental Association (ADA) published guidelines in 2019 recommending limited antibiotic prescribing for the treatment of dental pain and swelling. We characterized dental prescribing during 2018–2022 to assess whether antibiotic use decreased after the guideline’s release. In addition, we examined access to dental care. Methods: All antibiotic prescriptions dispensed during 2018–2022 were extracted from the IQVIA Xponent database, which captured ≥92% of all U.S. outpatient prescriptions and projected to 100% coverage. Prescriptions by general dentists were compared to total outpatient oral antibiotic prescriptions and summarized by patient sex, patient age, and prescriber geographic region. Census denominators were used to calculate prescribing rates per 1,000 persons. IQVIA general dentist counts were used to calculate dentists per 100,000 persons. Results: General dentists prescribed 24.7 million antibiotic prescriptions in 2018 (75 prescriptions per 1,000 persons) compared with 25.2 million (76 prescriptions per 1,000 persons) in 2022. During 2020–2022, general dentists prescribed >10% of all outpatient antibiotic prescriptions (range 10.7%–12.1%). In each year, prescription rates were higher for females, patients > 65 years, and among prescribers in the Northeast. In 2022, there were 58 general dentists per 100,000 persons in the United States. The highest general dentist rate was in District of Columbia (100 per 100,000 persons) and the lowest rate was in Delaware (41 per 100,000 persons). Conclusions: Despite the ADA’s 2019 guidelines, prescribing by general dentists remained stable during 2018–2022. Because the total number of antibiotic prescriptions overall decreased, general dentists’ share of all outpatient antibiotic prescriptions increased to >10% in recent years. Rate variation by patient characteristics and prescriber region may reflect differences in dental disease burden or may represent unnecessary antibiotic use. Dental antibiotic stewardship is needed, including dissemination and implementation of current prescribing guidelines. Further evaluation of prescribing indications and access to dental care is needed to inform dental stewardship priorities.

Risk Factors Predicting Complication of OPAT in an Academic Center: A Retrospective Cohort Study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s53-s54
-
- Article
-
- You have access
- Open access
- Export citation
-
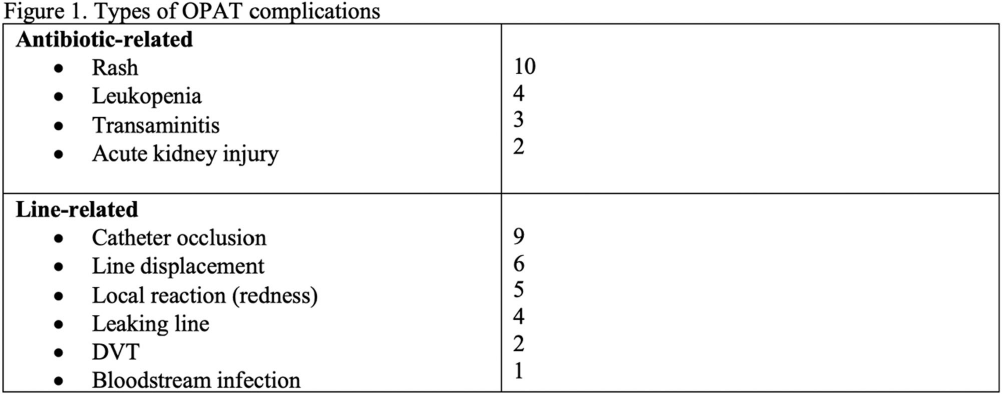
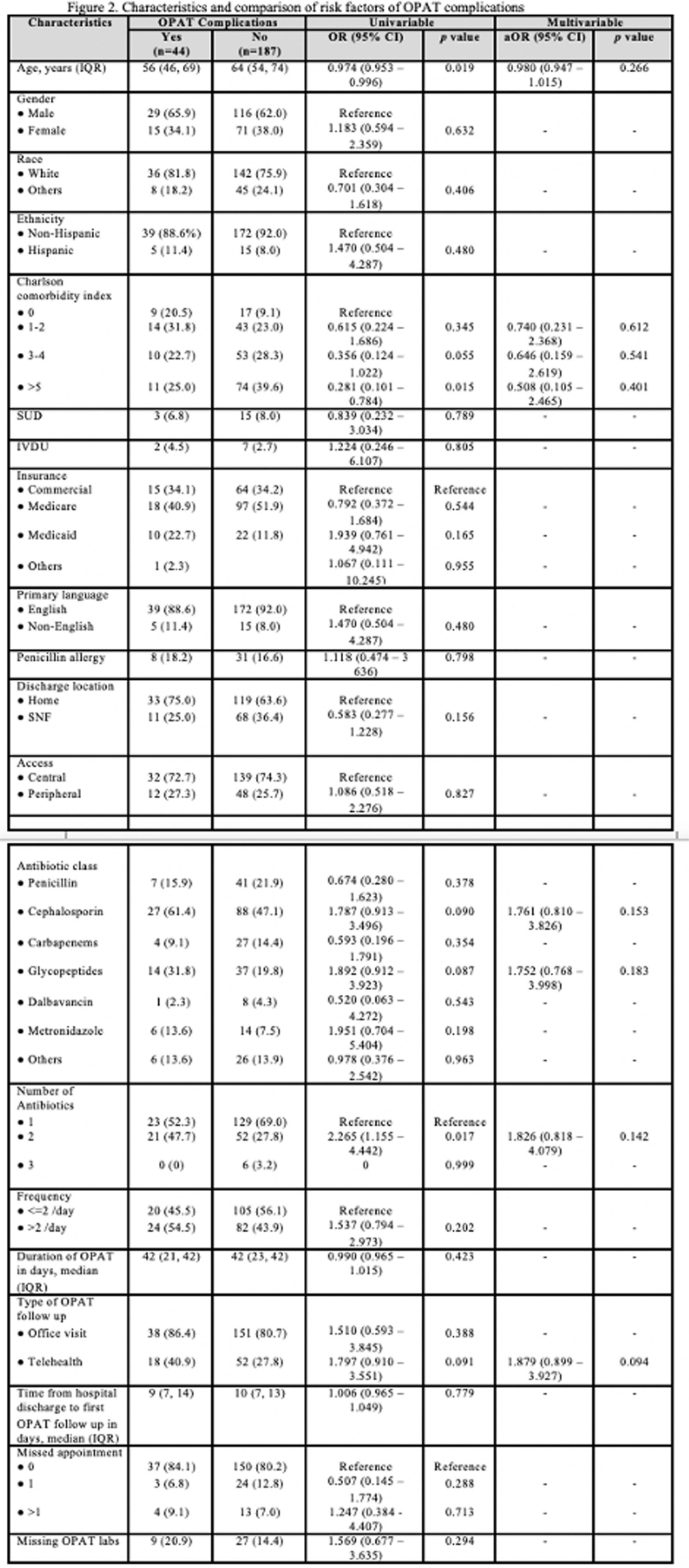
Background: While Outpatient Parenteral Antibiotic Therapy (OPAT) offers patient convenience and reduced healthcare costs, its increasing utilization has brought various complications to light, including antibiotics-related and line-related OPAT complications. In a large prospective study, 18% of the patients experienced adverse drug events. Another study showed 8.45% of patients had vascular complications. Our study aims to identify clinical predictors associated with OPAT complications. Identifying predictors for suboptimal OPAT outcomes provides an opportunity to intervene, thereby minimizing the risk of OPAT-related complications. Method: We conducted a retrospective cohort study at Tufts Medical Center of all adult patients aged ≥18 years discharged on OPAT from April 2022 to October 2022. Demographic, treatment, outcome, and complications data were extracted through chart review. The primary outcome was the proportion and predictors of OPAT complications. The secondary outcomes were OPAT completion rate, 30-day ED visit, and 30-day readmission rates related to OPAT complications. We used univariable and multivariable analyses using logistic regression models for the predictors of OPAT complications. Variables with p5 (OR, 0.281, 95% CI 0.101–0.784), but they were more likely to have received two antibiotics (OR, 2.265; 95% CI 1.155-4.442). However, no significant independent predictor OPAT complications was identified in multivariable regression analysis (Figure 2). OPAT completion rates were lower in patients with complications (59.1% versus 75.4%). The 30-day ED visit and 30-day readmission rates were significantly higher in the complication group (31.8% vs. 0 and 34.1% vs. 2.1%, respectively). Conclusion: Our study highlights the significant difference in treatment completion rates and higher incidence of ED visits and readmissions rates among those with OPAT complications. Although specific independent predictor was not identified, the association with multiple antibiotic therapies and telemedicine follow-ups suggests areas for further investigation.