Refine listing
Actions for selected content:
142352 results in Open Access

Regional variations in the demographic response to the arrival of rice farming in prehistoric Japan
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Creation of a Multi-Year Pediatric Candidemia Antibiogram in Georgia Identifies Changing Epidemiology and Resistance Trends
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s129-s130
-
- Article
-
- You have access
- Open access
- Export citation
Factors Associated with Inappropriate Urine Culture Orders in Hospitalized Patients with Indwelling Urinary Catheters
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s69
-
- Article
-
- You have access
- Open access
- Export citation
-
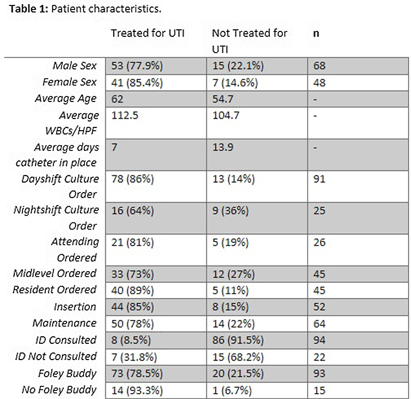
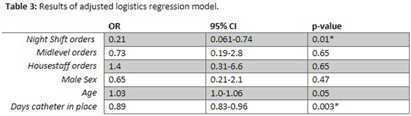
Background: Catheter-associated urinary tract infection (CAUTI) is among the most prevalent healthcare-associated infections. Clinical diagnosis of CAUTI and National Healthcare Safety Network (NHSN) definitions do not always align. Most patients with indwelling urinary catheters ultimately develop asymptomatic bacteriuria (ASB) due to bacterial colonization and may be misattributed as CAUTI. Urine cultures ordered on patients with ASB may lead to reporting of non-clinically significant CAUTI to NHSN. We sought to examine factors associated with ordering inappropriate urine cultures in patients with urinary catheters. Methods: All CAUTIs that were reported to the NHSN at a large academic medical center in Eastern North Carolina were evaluated from October 2021-July 2023. A logistic regression model was fit for patients treated for urinary tract infection (UTI) with the following covariates: age, sex, time of urine culture order, provider type, and days that the urinary catheter was in place. All data analysis was performed in SAS (SAS Institute Inc., SAS 9.4, Cary, NC: SAS Institute Inc., 2002-2023). Results: Table 1 demonstrates patient characteristics stratified by treatment for UTI. The analysis suggests that abnormalresults from urine cultures ordered overnight were less likely to be treated with antibiotics,and this result was statistically significant in both the adjusted and unadjusted analyses – see table 2 and 3. The model also suggests abnormal results from urine cultures ordered by housestaff and older patients were more likely to be treated for UTI, but these results were not statistically significant – see table 3. Finally, the longer a catheter was in place the less likely an abnormalurine culture was to be treated and this finding was statistically significant – see table 3. Conclusion: Cultures that did not prompt antimicrobial treatment did not impact patient care decisions and could be considered as inappropriate orders. This can result in CAUTIs reported to NHSN that were not clinically significant. Abnormal results from cultures that were ordered by the overnight team were less likely to be treated for clinical UTI and this may represent an important target for diagnostic stewardship interventions.




Perspectives and Awareness of Environmental Sustainability in the Infection Prevention and Control Community Nationally
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s25
-
- Article
-
- You have access
- Open access
- Export citation
Exposure to anti-refugee hate crimes and support for refugees in Germany
-
- Journal:
- Political Science Research and Methods / Volume 13 / Issue 3 / July 2025
- Published online by Cambridge University Press:
- 16 September 2024, pp. 755-764
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Clinical and Genomic Characteristics of Candida auris in Central Ohio: An Insight into Epidemiological Surveillance
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s93
-
- Article
-
- You have access
- Open access
- Export citation
-
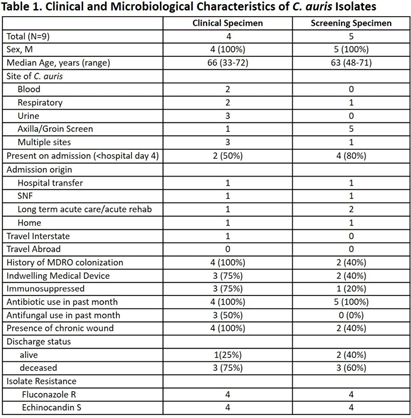
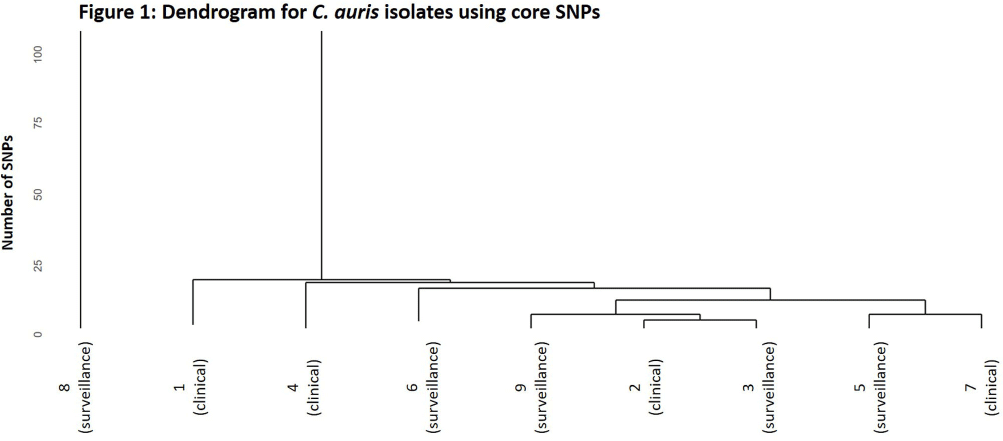
Background: Candida auris is an emerging threat to hospitalized patients and invasive disease is associated with high mortality. This study describes clinical and microbiological characteristics of nine patients identified with C. auris at Ohio State Wexner Medical Center discovered through active surveillance or clinical investigation and uses whole genome sequencing (WGS) to compare isolates. Methods: In November 2022, an active C. auris surveillance program was implemented to screen patients admitted to high-risk units (intensive care units and progressive care units). Bilateral axilla and groin swabs were obtained upon unit admission and, if positive, were submitted for C. auris polymerase chain reaction (PCR) with culture and sensitivity testing. Patients with a positive screening or clinical isolate from November 2022 to November 2023 underwent chart review for clinical characteristics, microbiologic data, and index admission information. For each isolate, DNA was extracted and WGS was performed. Core single nucleotide polymorphism (SNP) variation identified from the sequence data was used to infer genetic relationships among the isolates. Results: Nine patients were identified between November 2022 and November 2023. The clinical and microbiologic characteristics are summarized in Table 1. All patients were hospitalized at various acute care facilities across the state at least once in the preceding 12 months. C. auris was determined to be present on admission for 6 patients. For 5 of these patients, it was their first interaction with our healthcare system. Three patients were not in contact isolation for >3 days before C. auris was identified. Unit wide point-prevalence screening was completed in these cases and no evidence of transmission was found. WGS showed eight of the nine isolates were related with 28 or less core SNP differences between isolates (Figure 1). One isolate (8) was genetically distinct with >45000 core SNP differences. Five isolates were highly related with a range of 4-15 SNP differences. No temporal or spatial overlap at our institution was identified among these five patients. Conclusions: The active surveillance program identified several patients colonized with C. auris in addition to those found through clinical testing. Multiple risk factors for C. auris were identified with high patient mortality (67%). Majority of the isolates were closely related without association with a known outbreak or epidemiologic link, suggesting a possible diffuse common reservoir. Next steps with surveillance in acute care and long-term care facilities will be critical for early detection to halt transmission of this organism.


Evaluation of a Sepsis Alert System at a Veterans Affairs Medical Center
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s61
-
- Article
-
- You have access
- Open access
- Export citation
Investigation of a Donor-derived Carbapenamase-producing Carbapenem-resistant Enterobacterales Hospital Outbreak
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s126-s127
-
- Article
-
- You have access
- Open access
- Export citation
-
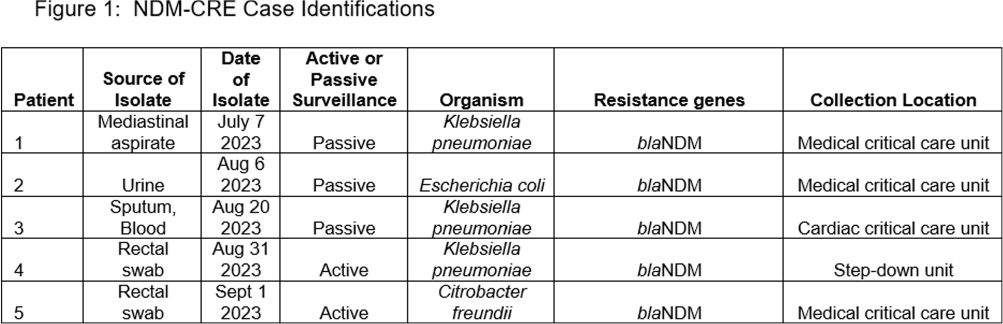
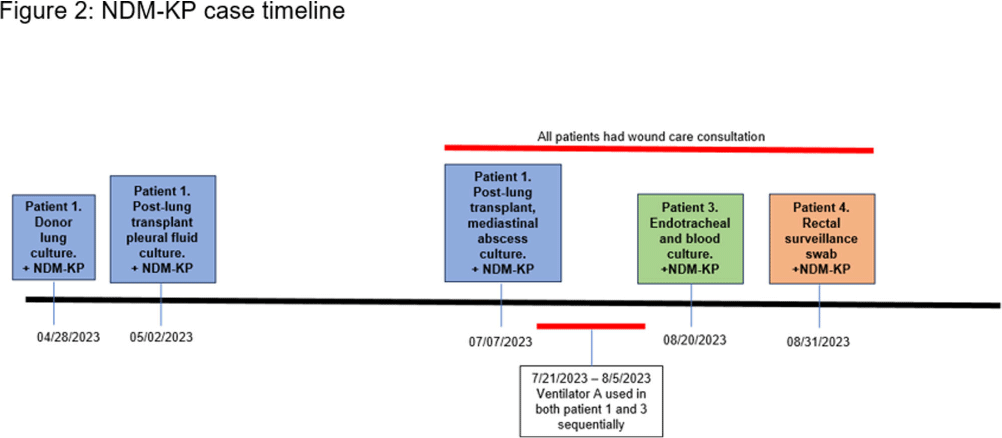
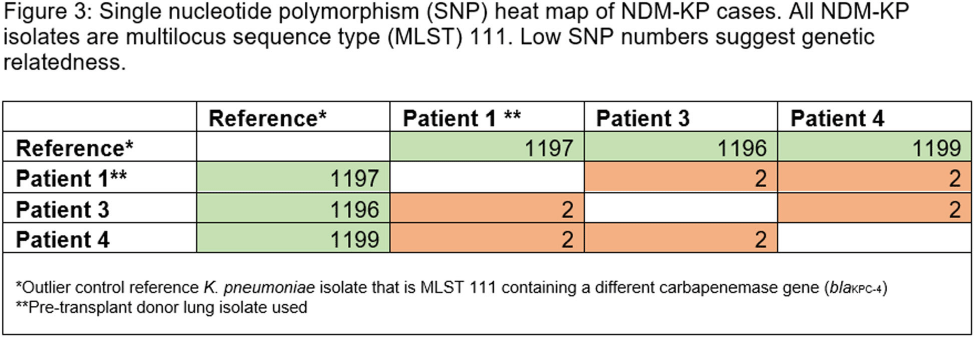
Carbapenamase-producing carbapenem-resistant Enterobacterales (CP-CRE) is an urgent public health threat for healthcare facilities. Solid organ transplant (SOT) recipients carry an increased risk for CRE infection and colonization due to prolonged exposures to antimicrobials, healthcare facilities and immunosuppression. CRE infection in SOT patients is associated with an increase in morbidity and mortality. Here, we describe a hospital outbreak investigation of three cases of New Delhi metallo-beta-lactamase (NDM) - CRE that led to novel findings with implications for further interdisciplinary investigations. An NDM-CRE infection in a critically-ill patient was identified during passive surveillance and prompted an investigation. Previous CP-CRE passive surveillance cases were reviewed. Rectal screening was performed for potentially exposed patients. 403 rectal swabs were tested for carbapenemase genes in active surveillance. Patients identified to have a new NDM-CRE isolate on active or passive surveillance were considered cases and underwent in-depth chart review including possible patient-to-patient exposures, hospital locations, procedures, devices, and consultations. NDM-CRE isolates were sent to the Minnesota Department of Health (MDH) for whole genome sequencing (WGS) to assess relatedness. Five NDM-CRE cases were identified, with all isolates harboring blaNDM including three NDM-Klebsiella pneumoniae (NDM-KP) cases (Figure 1). The first NDM-KP case, patient 1, developed mediastinal infection following lung transplantation. Review of United Network for Organ Sharing revealed that respiratory specimens from patient 1’s donor grew NDM-KP and a bronchial wash at the time of transplant yielded NDM-KP. The second NDM-KP case (patient 3) developed ventilator-associated pneumonia and was found to have used sequentially the same ventilator as patient 1. The third NDM-KP case (patient 4) was detected via rectal swab in active surveillance and shared wound care personnel in common with patients 1 and 3 (Figure 2). WGS demonstrated two single nucleotide polymorphisms (SNP) among all three isolates, strongly suggesting relatedness (Figure 3). Best practices for infection prevention were reviewed with wound care personnel. To date, no further NDM-KP isolates have been identified. Investigation was facilitated by in-depth chart review and WGS via the Central Region Antimicrobial Resistance Laboratory Network at MDH. Detection of the NDM-KP from a lung donor specimen appears genetically linked to clinical isolates in other patients, raising the possibility of a donor-derived hospital outbreak. This investigation is the first to describe a donor-derived NDM outbreak in a healthcare facility. Communication between organ procurement agencies, transplant centers, and infection prevention must be optimized to prevent CRE-associated morbidity in SOT receipts and CRE hospital outbreaks.



Morphological evaluation for the narrowest section of the patent ductus arteriosus in infants by CT: a crucial point for device closure
-
- Journal:
- Cardiology in the Young / Volume 34 / Issue 9 / September 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 1983-1989
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Rapid Genomic Characterization of High-Risk, Antibiotic Resistant Pathogens Using Long-Read Sequencing to Identify Nosocomial
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s106
-
- Article
-
- You have access
- Open access
- Export citation
The distribution of non, nenny and non fait in Pre-Classical and Classical French
-
- Journal:
- Journal of French Language Studies / Volume 34 / Issue 3 / November 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 431-456
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Multitask Neural Networks to Predict Antimicrobial Susceptibility Results of Escherichia coli Clinical Isolates
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s26-s27
-
- Article
-
- You have access
- Open access
- Export citation
-
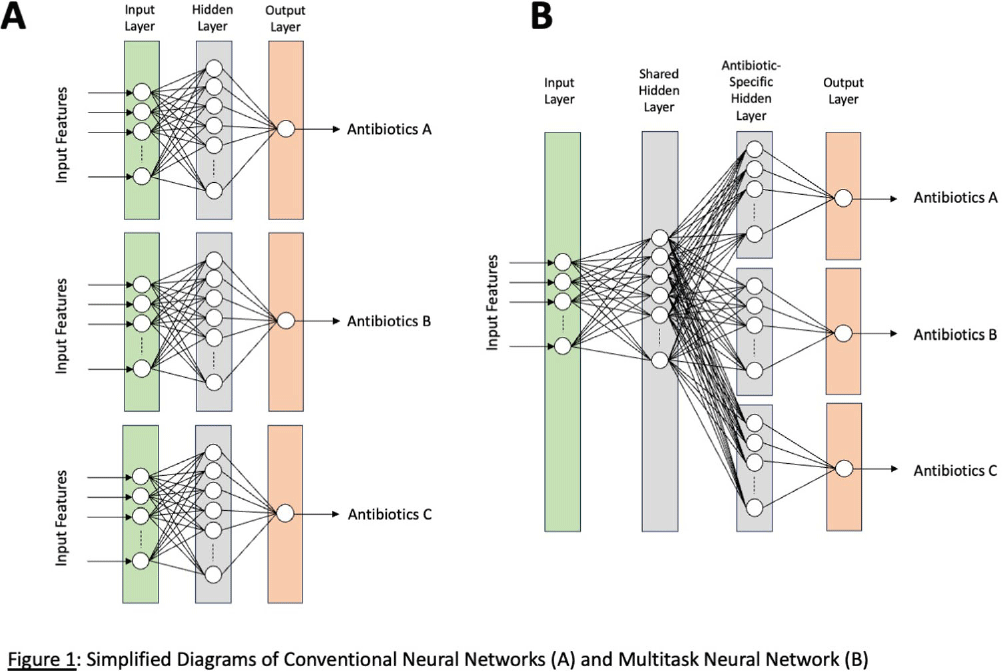
Background: Machine-learning (ML) models, such as neural networks (NNs), have been proposed to predict antimicrobial susceptibility at the patient level while incorporating patient-level information from electronic medical record (EMR) systems. However, NNs often do not perform well in predicting rare outcomes, such as carbapenem resistance. We aimed to apply a novel multitask NN to create personalized antibiograms for individual patients with Escherichia coli clinical isolates to predict antimicrobial resistance (AMR) for four major antimicrobial classes simultaneously with improved accuracy for carbapenem resistance by using shared hidden layers (Figure 1). Methods: We analyzed all E. coli clinical isolates from the US Veterans Health Administration’s network from January 1, 2017, to December 31, 2019, focusing on AMR profiles of aminopenicillins, narrow-spectrum (NS) cephalosporins, extended-spectrum (ES) cephalosporins, and carbapenems. Patient-level clinical data (demographics, antimicrobial exposure history, previous isolates (if any), comorbidities, and recent procedures) were extracted from EMR. Antibiograms for all hospitals were generated using standard methods for the preceding calendar years. We employed logistic regression to evaluate the efficacy of conventional antibiograms in predicting AMR profiles. We adopted the ML approach using conventional NNs and novel multitask NNs on all extracted clinical data and hospital antibiograms. The models were trained with data from 2017 and 2018 and then tested on 2019 data, assessing their performance using the area under the receiver-operating curve (AUC). Results: The study included 257,968 E. coli isolates, split into 171,391 for training and 86,577 for validation. The prevalence of AMR in the test data from 2019 was 49.8% for aminopenicillins, 28.4% for NS cephalosporins, 10.7% for ES cephalosporins, and 0.2% for carbapenems, respectively. Conventional hospital antibiograms showed low prediction accuracy with AUC scores of 0.56 for aminopenicillins, 0.67 for NS cephalosporins, 0.61 for ES cephalosporin, and 0.67 for carbapenem. AUC scores from preliminary models for conventional and multitask NNs were 0.78/0.78 for aminopenicillins, 0.83/0.82 for NS cephalosporins, 0.84/0.85 for ES cephalosporins, 0.68/0.75 for carbapenems. While producing improved accuracy for carbapenem and comparable accuracies for three other classes, multitask NNs took approximately 66% less time for model training than conventional NNs. Conclusions: Integrating EMR data with NNs improved their predictive accuracy, potentially leading to a decision-support tool for better empirical antimicrobial therapy guidance in the window between species identification and confirmed susceptibilities. Multitask NNs can potentially improve the prediction accuracy of uncommon AMRs while maintaining comparable prediction accuracies for common AMRs and optimizing the efficiency of model training.
Disclosure: Michi Goto: Contracted Research - Merck

Case validation of bloodstream infections with an antibiotic-resistant organism
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s156
-
- Article
-
- You have access
- Open access
- Export citation
Bad Habits that Stick: An Investigation into Adhesive Medical Tape Use Practices and Beliefs
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s29
-
- Article
-
- You have access
- Open access
- Export citation
Patient First Strategies for Reducing Inequities in HAI Prevention
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s76-s77
-
- Article
-
- You have access
- Open access
- Export citation
Inpatient Hospice Impact on Blood Culture Practices Near the Time of Death, Tertiary Center, Northern California, 2019–2023
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s85-s86
-
- Article
-
- You have access
- Open access
- Export citation
-
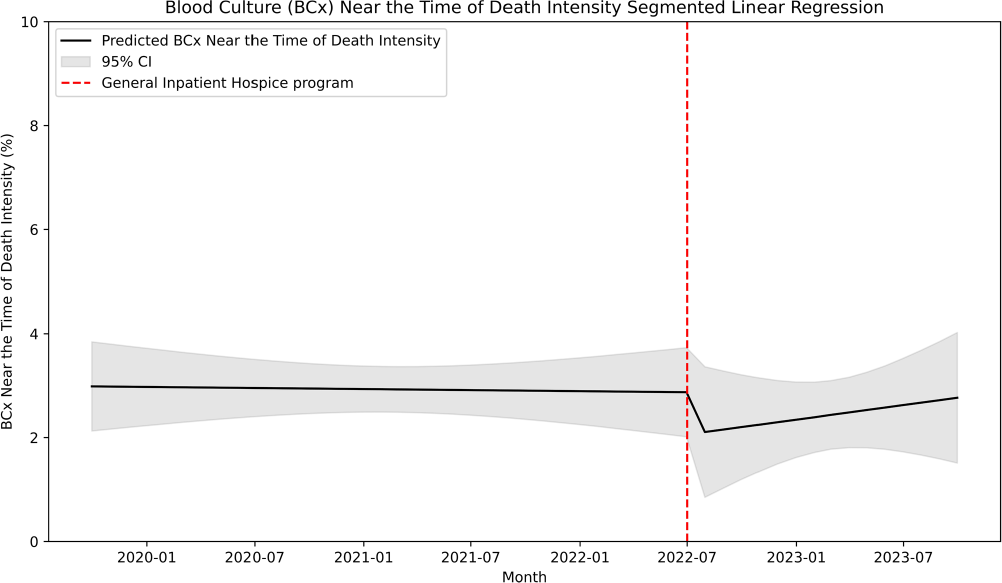
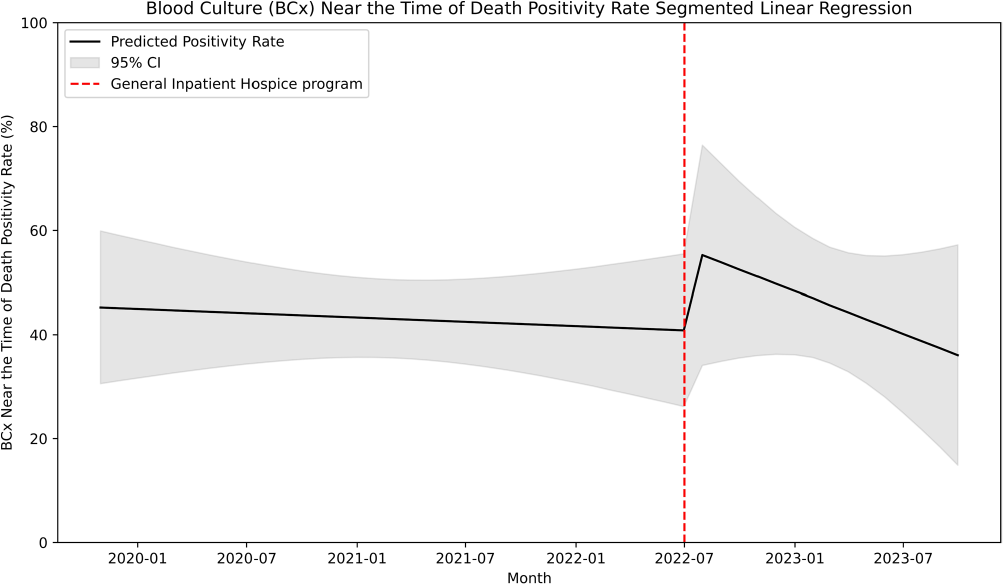
Introduction: Many central line-associated bloodstream infections are identified in patients nearing the end of life. Stanford Health Care recently introduced the General Inpatient Hospice program. This program offers inpatient hospice care for patients who, due to uncontrolled symptoms, cannot be discharged to a hospice facility or receive home hospice care. We investigated whether this program would impact blood cultures practices near the time of death. Methods: We performed a retrospective cohort study at Stanford Health Care using records of blood culture events from May 2019 to October 2023. We defined a blood culture near-death as those collected within 2 days before the date of death. We performed an interrupted time series linear regression before and after the implementation of the General Inpatient Hospice program on July 1, 2022 to assess blood culture intensity near-death. Blood culture intensity was defined as the proportion of cultures collected near-death in relation to the total number of blood cultures. Additionally, we calculated blood culture positivity rate, which was defined as the proportion of positive blood cultures among all those collected during our study period. Results: Out of 220,269 blood cultures from 24,955 unique patients, a total of 6,147 cultures (9%) were obtained near the time of death. Among these subjects, the median age was 65 years (range 20–102), with 43% identifying as being of White race-ethnicity and 57% as male. Of these cultures, 3044 were positive (49.5%), with Escherichia coli (618, 24%), Klebsiella pneumoniae (341, 13%), and Staphylococcus aureus (166, 10%) being the most common organisms. After the implementation of the General Inpatient Hospice program, the median enrollment was 12 patients (range 3–18) and the median mortality rate was 2.3% (range 2–3%). The blood culture intensity near death decreased by 0.81%, a change that was not statistically significant (95% CI -2.4% to 0.8%, p=.32; Figure 1). Subsequently, the blood culture intensity showed a non-significant increasing trend of 0.05% (95% CI -0.1% to 0.2%, p=0.53). The blood culture positivity rate near the time of death increased by 16% following the intervention, but this increase was not statistically significant (95% CI – 11.8% to 43.3%, p=.26; Figure 2), and it was followed by a non-significant downtrend of 1.9% (95% CI -3.9% to 1.4%, p=.36). Conclusion: We found no significant association between the implementation of an inpatient hospice program and blood culture practices near the time of death, likely due to low patient enrollment.


Estimating public opinion from surveys: the impact of including a “don't know” response option in policy preference questions
-
- Journal:
- Political Science Research and Methods / Volume 13 / Issue 3 / July 2025
- Published online by Cambridge University Press:
- 16 September 2024, pp. 663-679
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Methylome-wide association study of multidimensional resilience
-
- Journal:
- Development and Psychopathology / Volume 37 / Issue 4 / October 2025
- Published online by Cambridge University Press:
- 16 September 2024, pp. 1730-1741
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of Discontinuing Contact Precautions for Multidrug-resistant Gram-negative Enterobacteriaceae in a Large Health System
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s139-s140
-
- Article
-
- You have access
- Open access
- Export citation
-
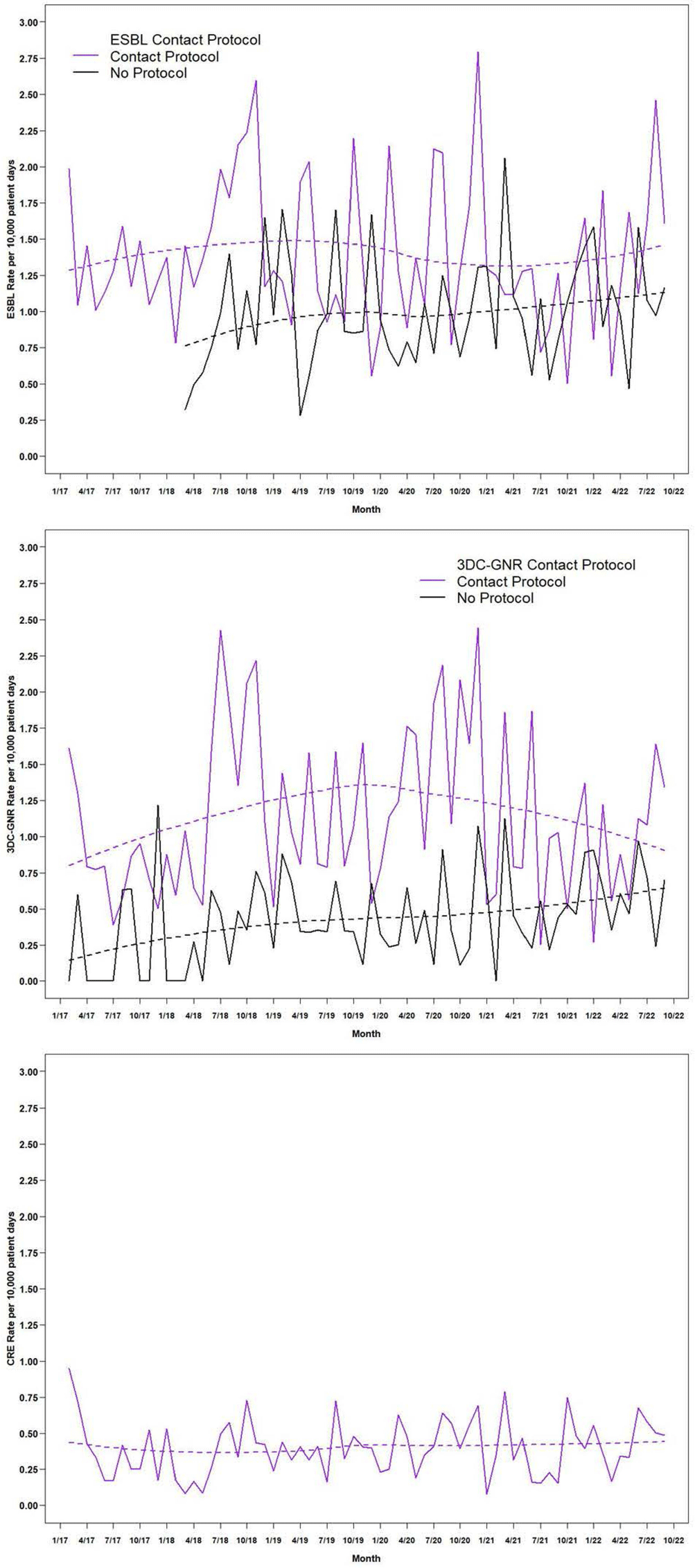
Background: Contact precautions (CP) to prevent transmission of multidrug-resistant gram-negative (MDRGN) Enterobacteriaceae are recommended, although studies of discontinuation of CP (DcCP) have found no change in healthcare associated infections (HAI) due to extended-spectrum beta-lactamase (ESBL) producing Enterobacteriaceae. Limited data exists on DcCP for MDRGN in a large health system. Methods: We performed a retrospective observational study analyzing the relationship between use of CP and HAI due to two definitions of MDRGN Enterobacteriaceae: ESBL, and non-susceptibility to ≥3 drug classes (3DC-GNR), with carbapenem resistant Enterobacteriaceae (CRE) serving as control. The study included all inpatient admissions from 2/2017 through 9/2022 at 21 acute care hospitals. Hospitals had latitude to determine CP practices based on local risk assessment, but in 2/2018, system-wide transmission-based precautions guidance was updated to recommend DcCP for MDRGN Enterobacteriaceae and in 12/2019 was updated to clarify DcCP specifically for ESBL and 3DC-GNR while continuing CP for carbapenem-resistant organism carriage. We interviewed infection preventionists to define when CP were used for CRE, ESBL, and 3DC-GNR Enterobacteriaceae. HAI were defined using National Healthcare Safety Network criteria including all HAI categories. We compared the incidence rate of HAI attributable to the two MDRGN types in hospital months with and without use of CP, with HAI due to CRE as a comparison group since all hospitals used CP for CRE throughout the study period. Results: The periods of CP use, by hospital, are shown in Figure 1. Throughout the study period, there were 987 HAI attributed to ESBL Enterobacteriaceae, 579 due to 3DC-GNR Enterobacteriaceae, and 329 due to CRE. Figure 2 shows the unadjusted aggregate rate of HAI for each of the three MRGN types, including among hospitals with and without CP in each month, for ESBL and 3DC-GNR. In months with and without CP, the rate of HAI was 1.482/10,000 and 1.093/10,000 patient days (incidence rate ratio [IRR], 1.356 [95% confidence interval, 1.195-1.540]) for ESBL Enterobacteriaceae. In months with and without CP, the rate of HAI was 1.071/10,000 and 0.493/10,000 patient days (IRR,2.173[95% confidence interval, 1.838-2.569]) for 3DC-GNR Enterobacteriaceae. Conclusion: DcCP was not associated with an increase in HAI due to ESBL and 3DC-GNR Enterobacteriaceae in aggregated facilities that self-selected for DcCP. Facilities that used CP were associated with significantly higher rates of ESBL and 3DC-GNR Enterobacteriaceae, a relationship that did not change as hospitals DcCP for these MDRGN. Further analyses are necessary to assess for a causal relationship.



Analyzing the Relationship Between Socioeconomic Deprivation and Outpatient Medicare Part D Fluroquinolone Claims in Texas
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s75-s76
-
- Article
-
- You have access
- Open access
- Export citation
-
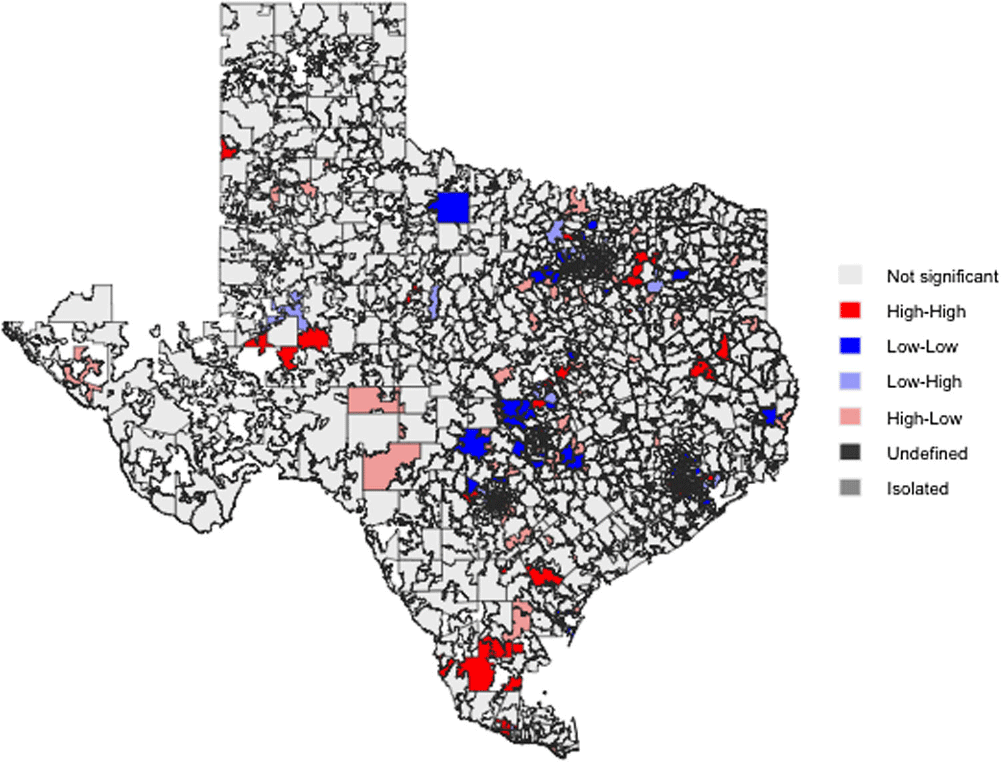
Background: Only a few studies have assessed the relationship between deprivation and excessive antibiotic use. In Texas, antimicrobial prescription is particularly high compared with the rest of the US. This study analyzed the association between local area socioeconomic deprivation and providers’ fluoroquinolone claim rates among beneficiaries 65 years and older in Texas. Method: This ecological study utilized provider- and area-level data from Medicare Part D Prescribers and the Social Deprivation Index (SDI) repositories. To identify geographic patterns and autocorrelation in and between SDI and fluoroquinolone claims, spatial dependence of these two variables was assessed by bivariate Local Indicators of Spatial Association (LISA) cluster mapping along with the global and local Moran’s I analyses. Negative binomial regression models were employed to evaluate the relationship between provider- and area-level characteristics (prescriber’s gender, specialty, rural-urban community area, beneficiaries' demographics, area-level population, and normalized SDI) and fluoroquinolone claim rates per 1,000 beneficiaries. Result: A total of 11,996 providers were included. There was no spatial dependence between SDI and rates of fluoroquinolone claims in Texas (Global Moran’s I =0.01, P=0.618). Bivariant LISA maps showed 85 high-high and 38 low-low spatial clusters. Higher SDI (incidence rate ratio (IRR) 0.98, 95% confidence interval (CI) 0.97-0.99 per 1-unit increment) and male providers (IRR 0.96, 95%CI 0.94-0.99) were associated with lower claim rates. In contrast, several factors were associated with higher claim rates, including non-metropolitan areas (1.04, 95%CI 1.00-1.09), and practices with a high proportion of male patients (IRR 1.12, 95%CI 1.10-1.14), Black patients (IRR 1.05, 95%CI 1.03-1.07), or Medicaid beneficiaries (IRR 1.15, 95%CI 1.12-1.17). Effect modification was observed between SDI and rurality, with higher SDI in non-metropolitan areas associated with higher claim rates, whereas SDI in metropolitan areas was inversely related to claim rates. Conclusion: This study showed that the distribution of high and low SDI and rates of fluoroquinolone claims were more geographically clustered than expected by random chance alone. Lower fluoroquinolone claim rates among Texas Medicare providers were seen in metropolitan areas with higher SDI, indicating potential barriers to care. Conversely, higher claim rates were observed in rural areas with higher SDI, signifying a possible knowledge or attitude gap towards fluoroquinolone use. These findings provide opportunities for public health professionals to explore gaps in the knowledge and attitudes of patients and providers related to antimicrobial use, particularly in rural regions, and investigate barriers to healthcare access in metropolitan areas.