Refine listing
Actions for selected content:
142351 results in Open Access
Teaching Antimicrobial Decision-Making in Medical Education: A Qualitative Study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s42-s43
-
- Article
-
- You have access
- Open access
- Export citation
-
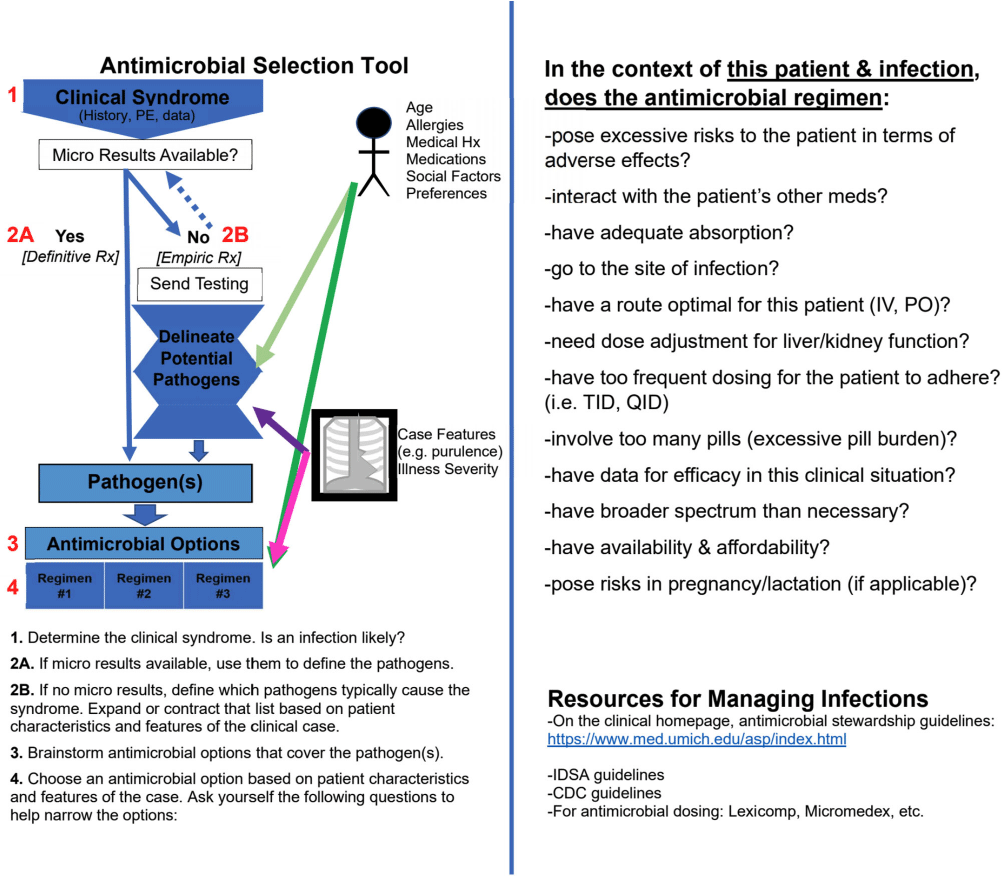
Background: Inappropriate use of antimicrobials contributes to the growing threat of antibiotic resistance. While physicians encounter infections in virtually every facet of medical practice, research has shown that physicians have difficulty determining the need for antimicrobials and choosing the right drug. Physicians’ difficulties with antimicrobial prescribing likely begin early in medical education, yet little is known about how medical students learn to make antimicrobial choices. Our study sought to better understand how medical students learn antimicrobial decision-making, including the impact of a new learning tool introduced in the Infectious Diseases (ID) and Microbiology preclinical course. Method: From 2021-2023, we conducted 18 individual interviews with a purposive sample of medical students at the University of Michigan who had taken the preclinical ID/Microbiology course during the 2019-2021 curricular years. We asked participants how they learned to make antimicrobial decisions and how the course and clinical rotations influenced their understanding of antimicrobial choice. The six participants who took the 2021 course were additionally asked how an antimicrobial decision-making tool introduced that year impacted that process (Figure 1). The tool was adapted from prior work on antimicrobial reasoning (Abdoler et al, 2020). Participants were asked whether they remembered being introduced to the tool (approximately 18 months prior) and if they utilized it during their clinical rotations. Results were analyzed using Dedoose Software to facilitate thematic analysis. Result: Several themes emerged on analysis. Nearly all participants reflected that they learned elements of antimicrobial decision-making during clinical rotations, through observation or direct interaction with physician mentors and patients. Several participants described the preclinical period as content learning, with clinical rotations providing a space to consolidate and scaffold knowledge, as well as transfer knowledge to new situations or tasks. Of the 6 students interviewed regarding the antimicrobial decision-making tool, only one remembered it and could accurately describe its components prior to being shown the tool during the interview. Conclusion: Results suggest that participants view the preclinical ID/Microbiology course primarily as an opportunity to learn content, and perceive learning antimicrobial decision-making directly from practicing physicians in the clinical portion of medical school. An antimicrobial decision-making tool introduced during the preclinical ID/Microbiology course in 2021 did not impact students’ conceptualization of how they learned this skill. Given that practicing physicians often make antimicrobial prescribing errors, regular re-introduction of the tool during clinical rotations may help bridge preclinical antimicrobial educational content to the clinical phase of learning, counteract inappropriate antimicrobial lessons encountered clinically, and ground students' burgeoning antimicrobial prescribing skills in a logical reasoning model.

Infection prevention making a difference on statewide standardized infection ratios for device-associated HAIs from 2015-2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s28-s29
-
- Article
-
- You have access
- Open access
- Export citation
-
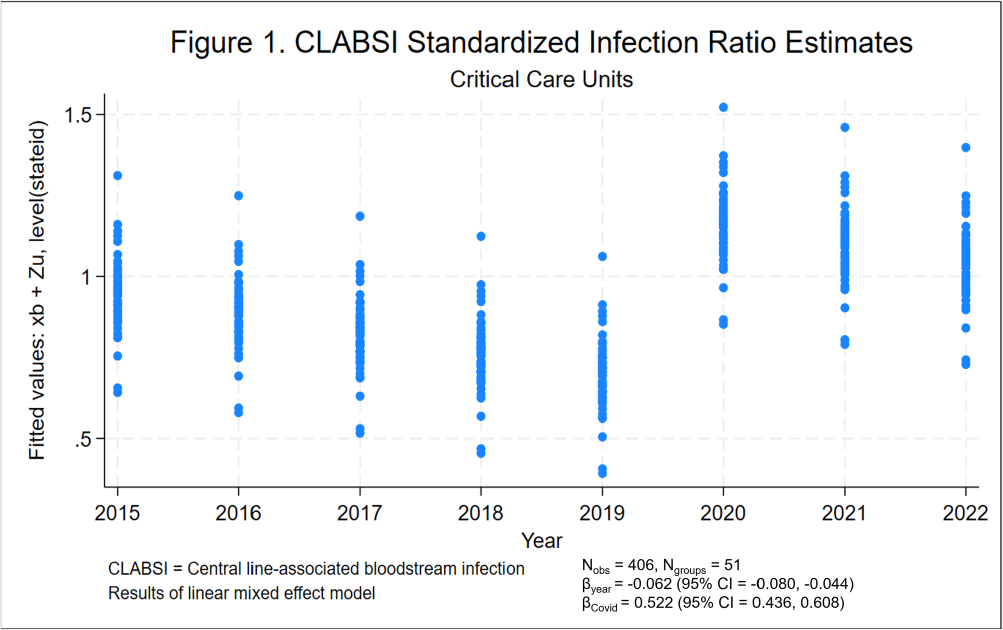
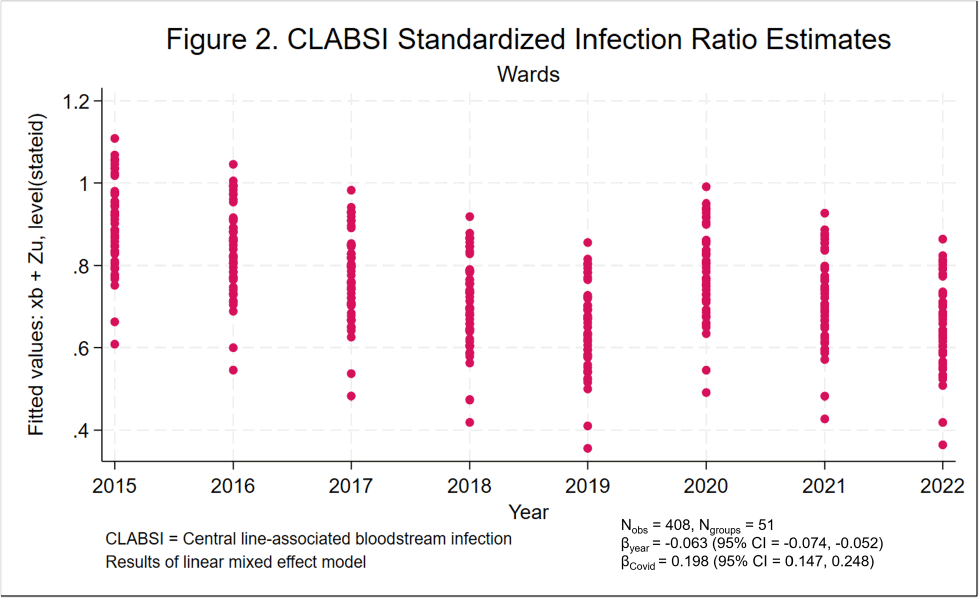
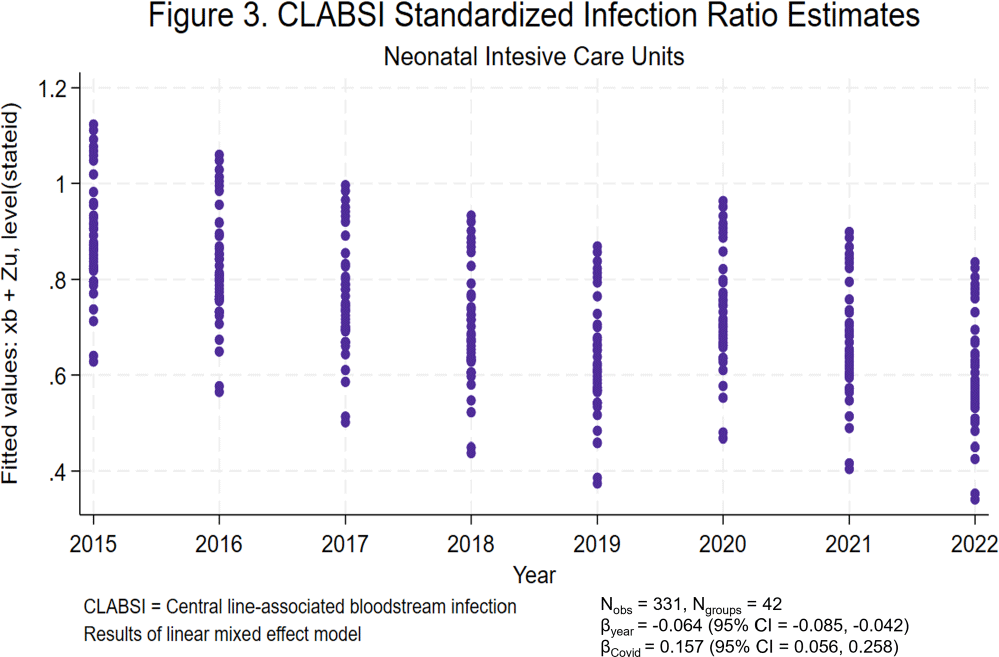
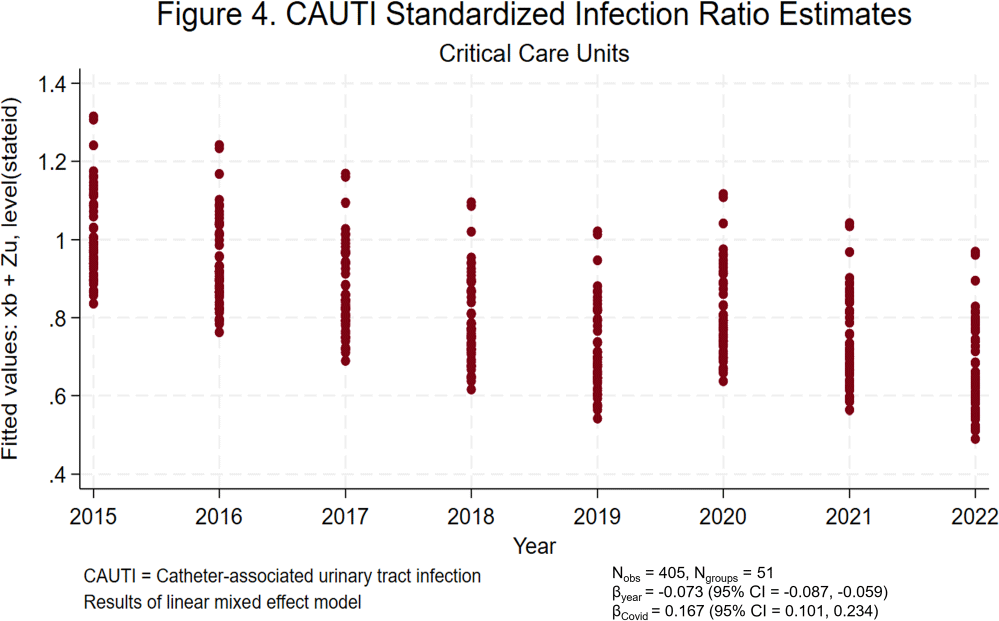
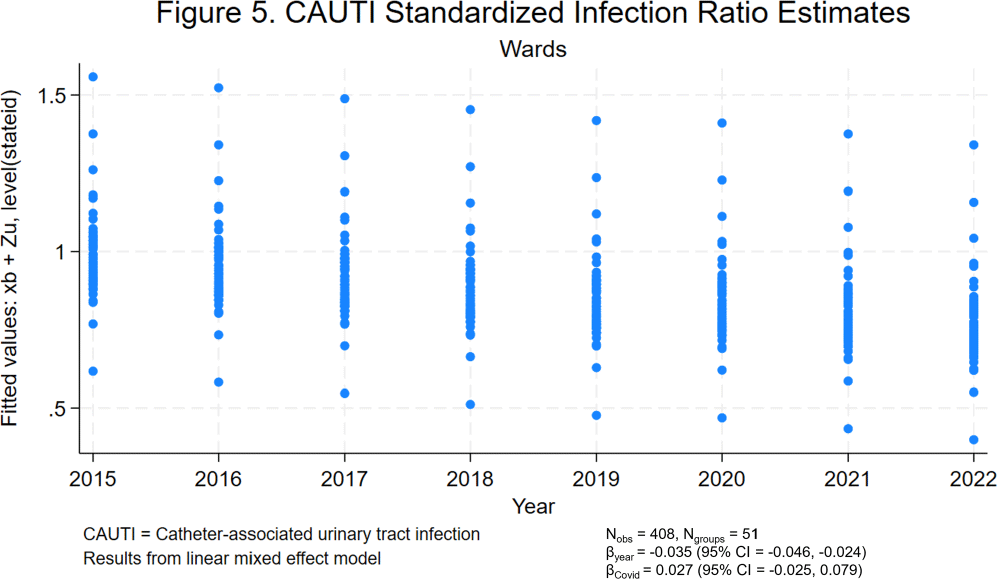
Background: Central line-associated bloodstream infections (CLABSIs) and catheter-associated urinary tract infections (CAUTIs) cause significant morbidity and mortality among hospitalized patients. Over the last 10 to 20 years, hospital accountability for the prevention of device-associated infections increased at the state and national levels. For example, the Centers for Medicare & Medicaid Services implemented the Hospital Inpatient Quality Reporting Program in 2015. The objective of this study was to assess the impact of increased federal attention on infection prevention using longitudinal data from the National Healthcare Safety Network (NHSN). We hypothesize that there was a significant decrease in statewide standardized infection ratios (SIRs) for CLABSI and CAUTI over the last 8 years. Methods: We collected SIRs for CLABSI and CAUTI in acute care hospitals for all 50 states and Washington D.C. from the NHSN database from 2015 to 2022. For CLABSI, we performed unique analyses for critical care units, wards, and neonatal intensive care (NICU) locations. For CAUTI, we stratified by critical care units and wards. We included all states with more than 5 hospitals reporting data. Those with fewer than 5 were excluded by listwise deletion in the corresponding analysis. We tested trends over time using linear mixed effect models with year as fixed effect and state as random effect. We also included an indicator variable representing the influence of SARS-CoV-2 (Covid-19) on healthcare-associated infections (HAIs). We elected an alpha of 0.05 as the threshold for statistical significance. Results: Overall, CLABSI and CAUTI SIRs exhibited significant negative slopes (Figures 1-5) after controlling for the influence of Covid-19. Each analysis revealed progressively lower SIRs compared to the previous year except for the 2019-2020 interval. Interestingly, the linear trend resumed after 2020 with subsequently lower SIRs in 2021 and 2022. Covid-19 had a greater influence on CLABSI SIRs in critical care settings compared to ward or NICU locations. The slope of CAUTI SIRs were impacted less by Covid-19 in wards compared to critical care settings. Conclusion: The results of the analysis demonstrate that CLABSI and CAUTI are trending in the desired direction despite the HAI spike during Covid-19. Government and hospital stakeholders in the United States should be encouraged by the reported trends and continue to prioritize the funding and use of resources for evidence-based device-associated infection prevention.





Exploring Socioeconomic Disparities in Surgical Site Infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s2-s3
-
- Article
-
- You have access
- Open access
- Export citation
-
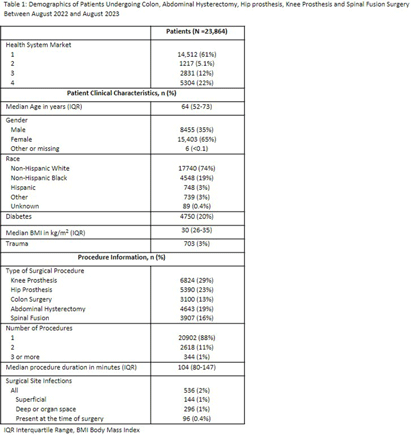
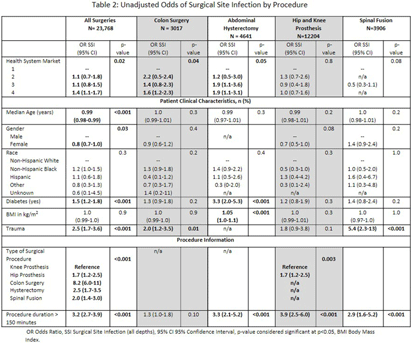
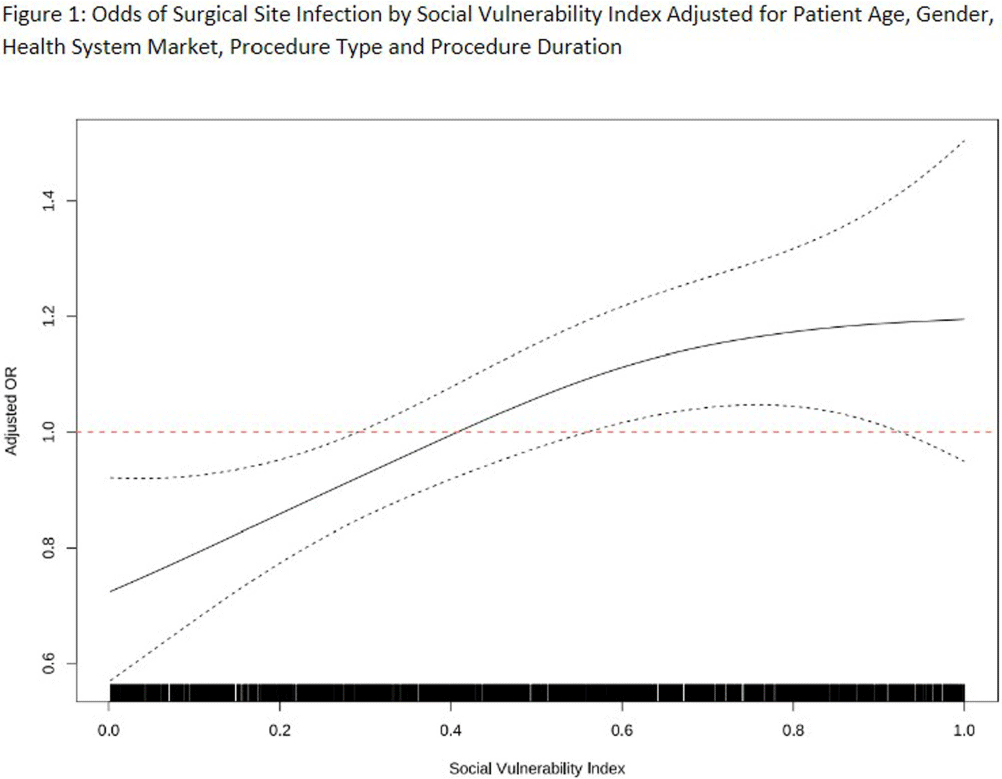
Introduction: Social disparities have been shown to impact a wide variety of healthcare outcomes. Surgical site infections (SSIs) are associated with substantial patient morbidity, but studies on the intersection of social disparity and SSI are limited. We sought to evaluate the association between SSI and the Center for Disease Control and Prevention’s social vulnerability index (SVI). Methods: Patients with National Health Safety Network (NHSN) procedure codes for colon, abdominal hysterectomy, hip prosthesis, knee prosthesis and spinal fusion surgeries were retrieved from the electronic medical records of 20 hospitals across 4 geographic markets. SSIs were identified by trained infection preventionists using NHSN definitions. Descriptive statistics were used for baseline demographic and clinical characteristics. Univariate logistic regression was performed to assess the association of demographic, clinical, and procedural factors with the outcome of SSI. Further univariate subgroup analysis was completed by procedure. To account for the nonlinear relationship between the social vulnerability index and SSIs, smoothing splines were used in a Bayesian hierarchical logistic regression model, with random effects to account for the different market practices. Nonlinear effects of procedure duration were also investigated while adjusting for the patient age, procedure type, and health system market. Results: 23,864 surgical procedures among 22,319 unique patients identified between 1 August 2022 and 31 August 2023. 96 patients with infection present at time of surgery were excluded. The study population was mostly white (74%) and female (65%) (Table 1). Less than 13% of the patients had more than one procedure during this time. In a univariate analysis, we found evidence of market and procedure effects, with colon surgery being associated with the highest odds of SSI. Procedure duration was significantly associated with SSI in both univariate and multivariable models, with a drastic increase in the odds of SSI for procedures > 150 mins. In the multivariable model we found that SVIs lower than 0.4 (95% CI 0.28 to 0.55) are associated with an adjusted odds ratio (aOR) < 1. (Figure 1) Conclusions: Our study shows that the relationship of social vulnerability and adverse outcomes is highly complex with nonlinear dynamics at play. After adjusting for procedure type, duration, patient age, gender and health system market the odds of SSIs increase sharply in patients with higher SVI until leveling off at an elevated risk.



An Improved Algorithm for the Detection of Ventilator Associated Pneumonia
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s151-s152
-
- Article
-
- You have access
- Open access
- Export citation
-
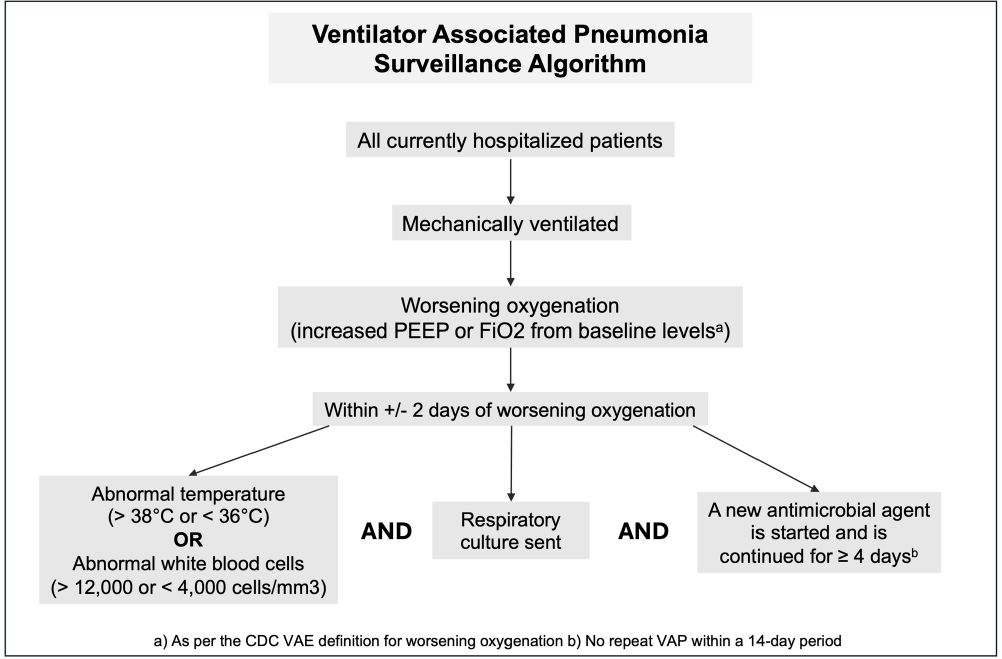
Background: Ventilator associated pneumonia (VAP) is associated with significant rates of morbidity and all-cause mortality. Active VAP surveillance can identify risk factors for which targeted preventive measures can be implemented. However, surveillance efforts are complicated by challenges associated with accurate VAP diagnosis. We aimed to improve the accuracy and automation of existing VAP diagnostic algorithms to better identify patients at risk. Methods: The study was conducted at NYU Langone Health from June 2022 through December 2023. We created a semi-automated VAP surveillance system using the Centers for Disease Control & Prevention (CDC) ventilator associated event (VAE) definition as a base framework (Figure 1). We modified this definition to include additional elements, such as having a sputum culture ordered within 48 hours of worsening oxygen status, regardless of culture result. Using this algorithm—followed by manual clinician reviews—we retrospectively assessed possible VAP cases to determine the ability of our surveillance system to correctly identify VAP. Results: Of the 123 possible VAP cases identified through our automated system, 75 (61%) were correctly diagnosed as VAP after clinical review. This reflects a rate of 1.5 infections per 1000 ventilation days across the system and 1.85 infections per 100 patients ventilated for greater than 2 days. Of the 48 remaining patients without VAP after clinical review, 25% (n=12) were characterized as having hospital-acquired pneumonia, 21% (n=10) as acute respiratory distress syndrome or infection at another site and 10% (n=5) as pulmonary embolism/infarction. Among all patients identified through this automated system (VAP and non-VAP), 53% experienced in-hospital death. Discussion: Our automated VAP surveillance algorithm identified 123 cases of potential VAP, 61% of which were consistent with a clinical diagnosis of VAP upon manual chart review. Our VAP rate of 1.5 infections per 1000 ventilation days was similar to published rates at other North American hospital systems. The high in-hospital mortality rate among these patients highlights the need for improved surveillance systems and earlier interventions to reduce the risk of VAP. There are several limitations to the CDC’s VAE definition, including its requirement of a positive microbiologic culture and focus on sputum quality. This potentially misses cases of culture-negative VAP in patients receiving antibiotics prior to sputum collection. Our goal is to continue to validate and improve our algorithm’s ability to correctly identify patients with clinical VAP, so that targeted prevention efforts can be focused upon the patients with the highest risk for poor outcomes.
Disclosure: Madeline DiLorenzo: Stocks - Abbvie, Amgen Inc., Becton Dickinson, Biogen Inc., Bristol Myers and Squibb, CVS Health, Davita Inc., Elevance Health, Gilead, Henry Schein, Hologic Inc., Humana Inc., Jazz Pharmaceuticals, Laboratory Corp, Merck and Co., Quest Diagnostics, ResMed Inc., Teladoc Health, Vertex Pharmaceuticals, West Pharmaceuticals


Excavating ancient pilgrimage at Nessana, Negev
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Guideline-unjustified inpatient therapy for non-ICU patients with community-acquired pneumonia (CAP) at 105 Veterans Affairs
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s40-s41
-
- Article
-
- You have access
- Open access
- Export citation
-
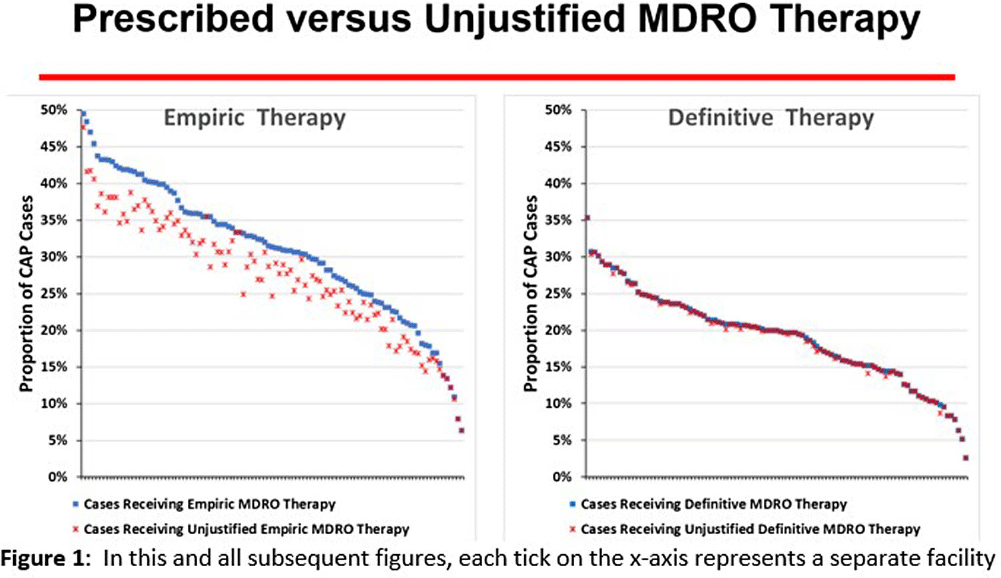
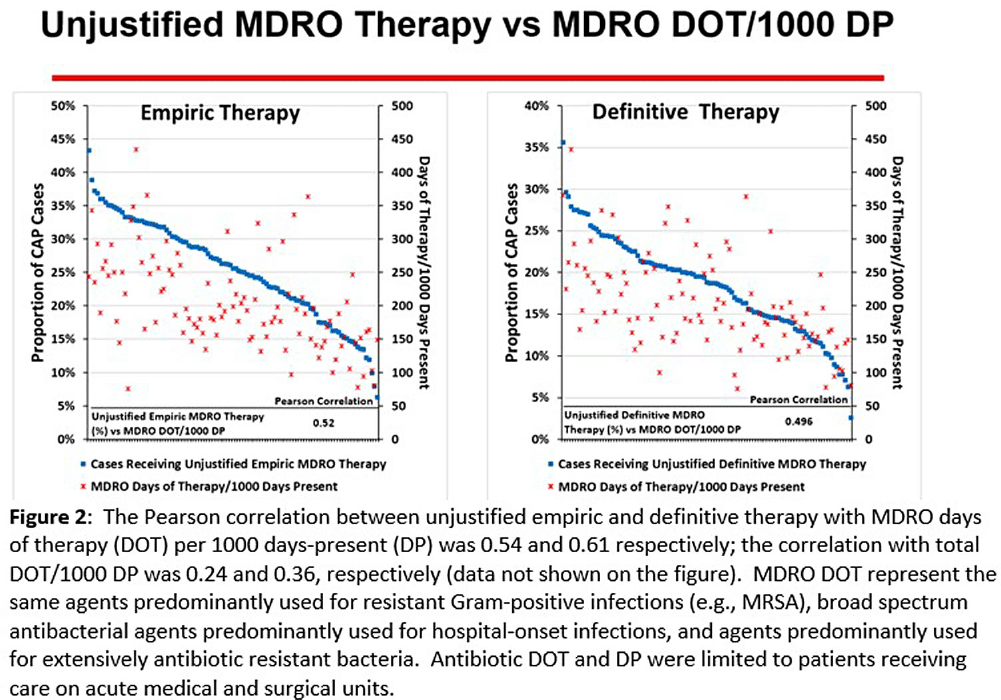
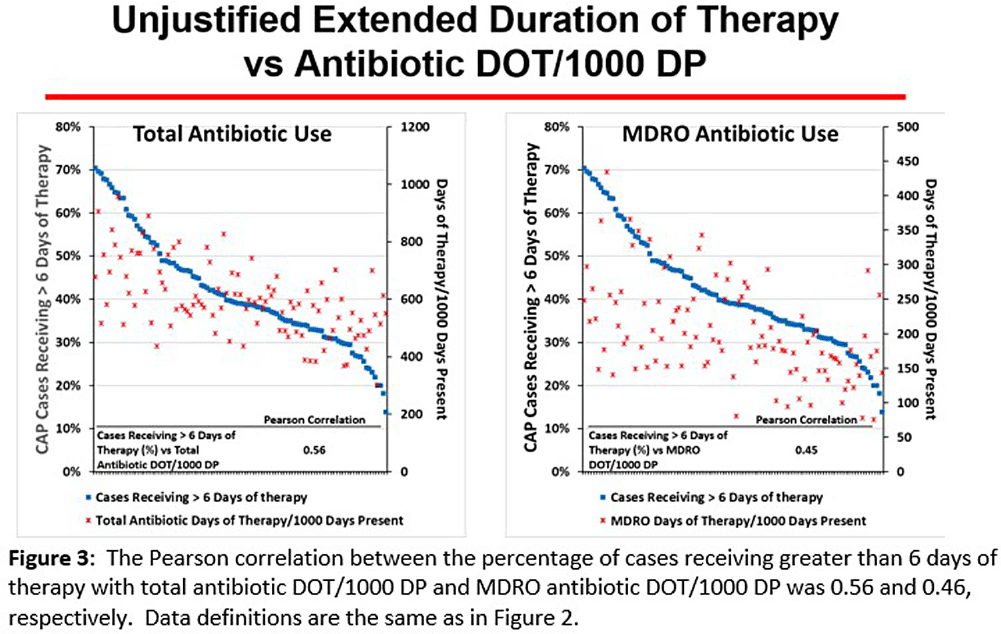
Background: CAP is often inappropriately treated with agents active against multidrug-resistant organisms (MDRO; methicillin-resistant S. aureus [MRSA] and P. aeruginosa [PSA]) and for prolonged duration. We assessed the relationship between antibiotic use with ATS/IDSA guideline-unjustified empiric and definitive MDRO therapy and prolonged duration in non-ICU inpatients with CAP at 105 VA Medical Centers. Methods: From VA Corporate Data Warehouse data, we identified patients with discharge ICD-10-CM codes consistent with CAP from 1/2022-3/2023, excluding cases with 14 days of antibiotic therapy, ICU admission, concurrent infections, or severe immunocompromise. We considered as jultified empiric (≤third day of hospitalization) therapy: anti-MRSA therapy for patients with prior positive MRSA cultures, anti-PSA therapy for patients with prior positive PSA cultures, and both anti-MRSA & anti-PSA therapy in patients with severe pneumonia and intravenous antibiotics in the prior 3 months. Definitive (>third day of hospitalization) anti-MDRO therapy was considered unjustified in patients who had achieved clinical stability and whose cultures did not grow MRSA or PSA. Prolonged duration (>6 days of therapy) was unjustified if patients were clinically stable or discharged by day 5. Results: The median age of the 29,260 patients was 75 (IQR 69,81); 4.6% were women. While 33% and 22% of patients received empiric or definitive MDRO therapy, such therapy was jultified in 12% and 0.5%, respectively. Median facility use of empiric and definitive MDRO therapy was 31% (IQR 25%,38%) and 20% (15%,23%), respectively (Figure 1); this use was unjustified in 89% (85%,93%) and 100% (100%,100%), respectively. Pearson’s correlation coefficient between MDRO therapy and rates of unjustified empiric and definitive MDRO therapy for CAP was 0.54 and 0.61, respectively (Figure 2). Although 99% of patients were discharged or stable by day 5, 42% received prolonged therapy. The median frequency of prolonged therapy was 39% (33%,48%); facility rates of prolonged therapy had a correlation of 0.56 with total antibiotic use and 0.46 with MDRO therapy (Figure 3). Discussion: Based on electronic documentation, we identified 1) substantial opportunities to reduce unjustified anti-MDRO therapy and the duration of therapy in hospitalized non-ICU patients with CAP; 2) a moderate correlation of unjustified anti-MDRO therapy with increased MDRO antibiotic use and of prolonged duration of therapy with increased total and MDRO antibiotic use. The correlation of lower quality prescribing with increased antibiotic use provides further impetus for tools such as dashboards (Figure 4) to assist antibiotic stewards in designing and monitoring interventions to reduce unjustified therapy.





MDRO Colonization Among Nursing Homes Patients: A Risk Classification Tool for Early Identification
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s118-s119
-
- Article
-
- You have access
- Open access
- Export citation
-
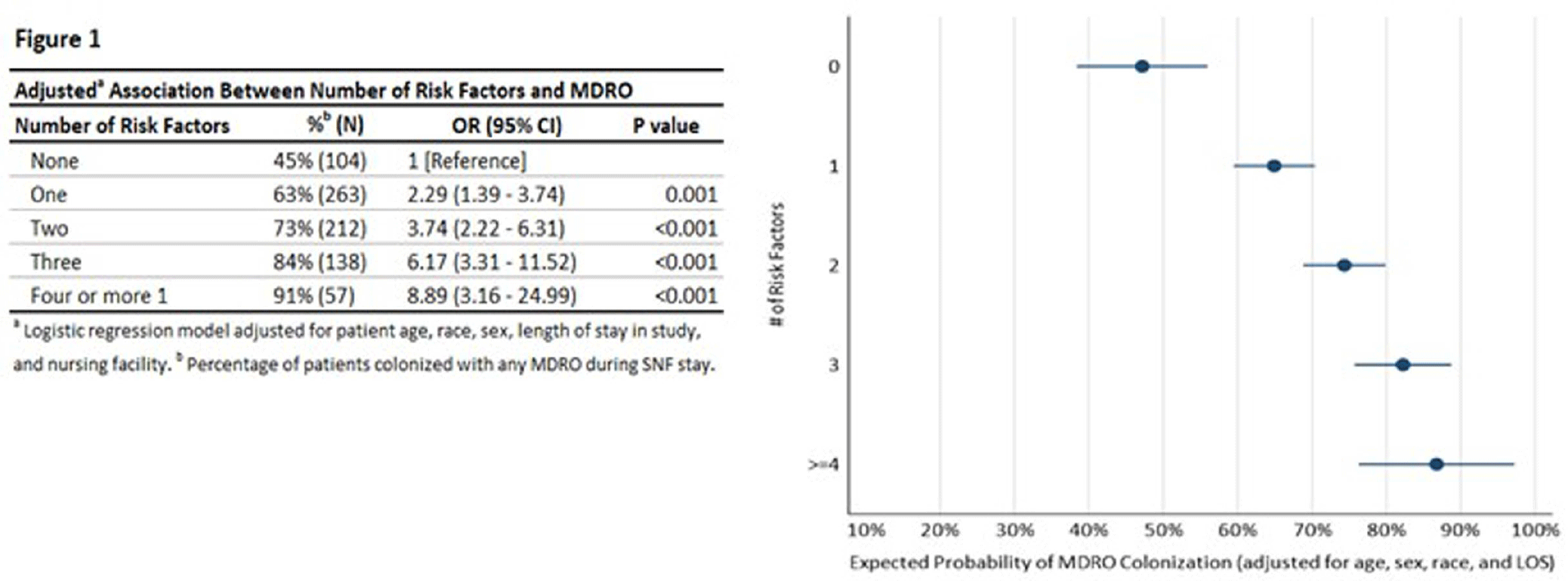
Background: Nursing homes (NHs) have high prevalence of multi-drug resistant organisms (MDROs) with rates exceeding those in hospitals. This study proposes quantifying patients’ risk of MDRO colonization and creating a risk profile for the NH patient populations to assist in reducing MDRO burden in health care facilities. Methods: We assessed a risk classification model using data from a prospective cohort study (2018 Pathways study). Patient sample included 783 newly admitted patients followed for up to 180 days and 9,587 samples collected from patients during 2,089 visits. Individual risk factors of MDRO colonization were assessed using unadjusted logistic regression, and patients were risk classified based on number of risk factors. Multivariate regression was performed to obtain odds of MDRO colonization for patient risk groups adjusting for patient age, sex, race, and length of NH stay (LOS). The risk classification tool developed using Pathways data was also tested among a sample of NH residents from Veterans Administration (N=190). Results: The patient sample (Pathways data) was 43.2% male, 37.2% Black with a mean age 74 years. 69.3% were colonized with a MDRO during the study. In unadjusted regression, recent antibiotic use (p<.001), open wounds (p<.05), use of urinary catheter or feeding tube (p<.001), functional disability (p<.001), diabetes (p<.01), and preadmission hospital stay over 14 days (p<.001) were associated with colonization, while Charlson comorbidity score, age, sex, and race were not. In adjusted analysis (c-statistic=0.75), a patient’s colonization risk increased with the number of risk factors (Figure 1), with 47.2% expected colonization among patients with none of the risk factors and 86.7% expected colonization among patients with four or more risk factors. The risk classification model had similar performance among male and female patients, and among Black and White patients (Figure 2). Secondary analysis using data obtained from separate, Veterans Administration facilities provided preliminary validation of the risk scoring tool. The model had acceptable fit (c-statistic=0.71). Veterans with four or more risk factors had 87.8% expected probability of MDRO colonization compared with 39.6% colonization among those without any risk factors. Veterans with less than four risk factors also had higher colonization, but these differences were not statistically significant. Conclusions. Despite system-wide efforts to reduce MDRO burden, prevalence of MDRO colonization remains high in NHs. The risk classification tool can assist in early identification of most vulnerable NH patients to direct targeted interventions such as education, enhanced environmental cleaning, and active surveillance.
Disclosure: Lona Mody: NIH, VA, CDC, Kahn Foundation; Honoraria: UpToDate; Contracted Research: Nano-Vibronix



Twenty-four hour urinary sodium and potassium excretion in adult population of Slovenia: results of the Manjsoli.si/2022 study
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 16 September 2024, e163
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Differential viral load of surgical masks worn by patients infected with respiratory viruses
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s141
-
- Article
-
- You have access
- Open access
- Export citation
Does Urinary Catheter Replacement Prior To Obtaining Urine for Culture Make a Difference?
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s69-s70
-
- Article
-
- You have access
- Open access
- Export citation
A Comparison of Variable Input Strategies used for Risk-adjustment Models of Antimicrobial Use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s30-s31
-
- Article
-
- You have access
- Open access
- Export citation
-
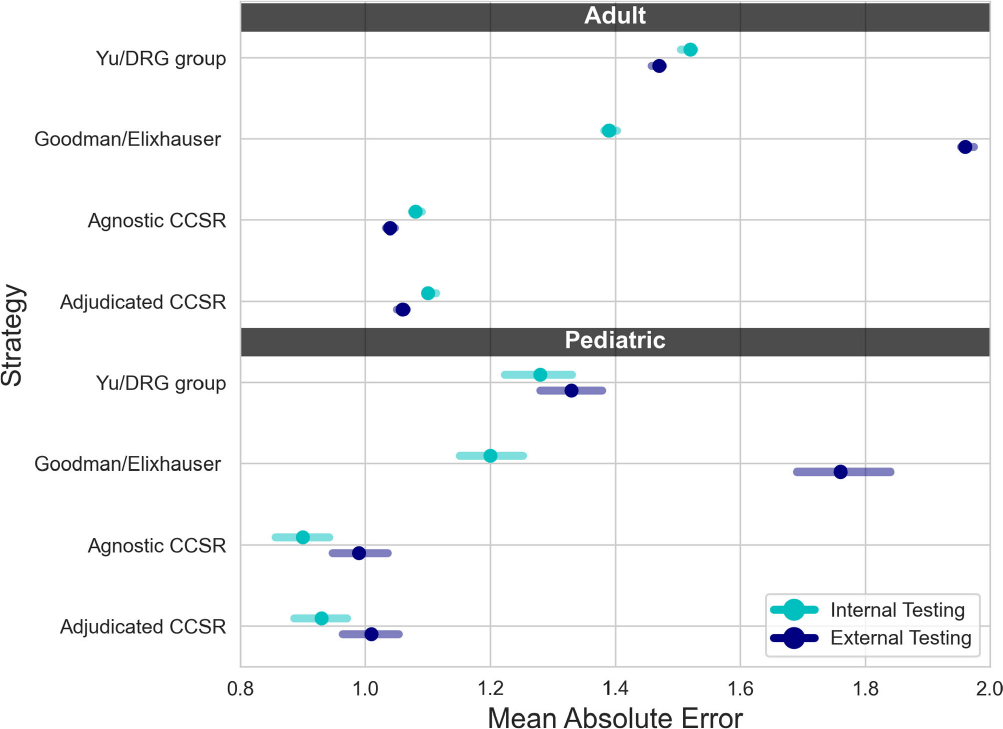
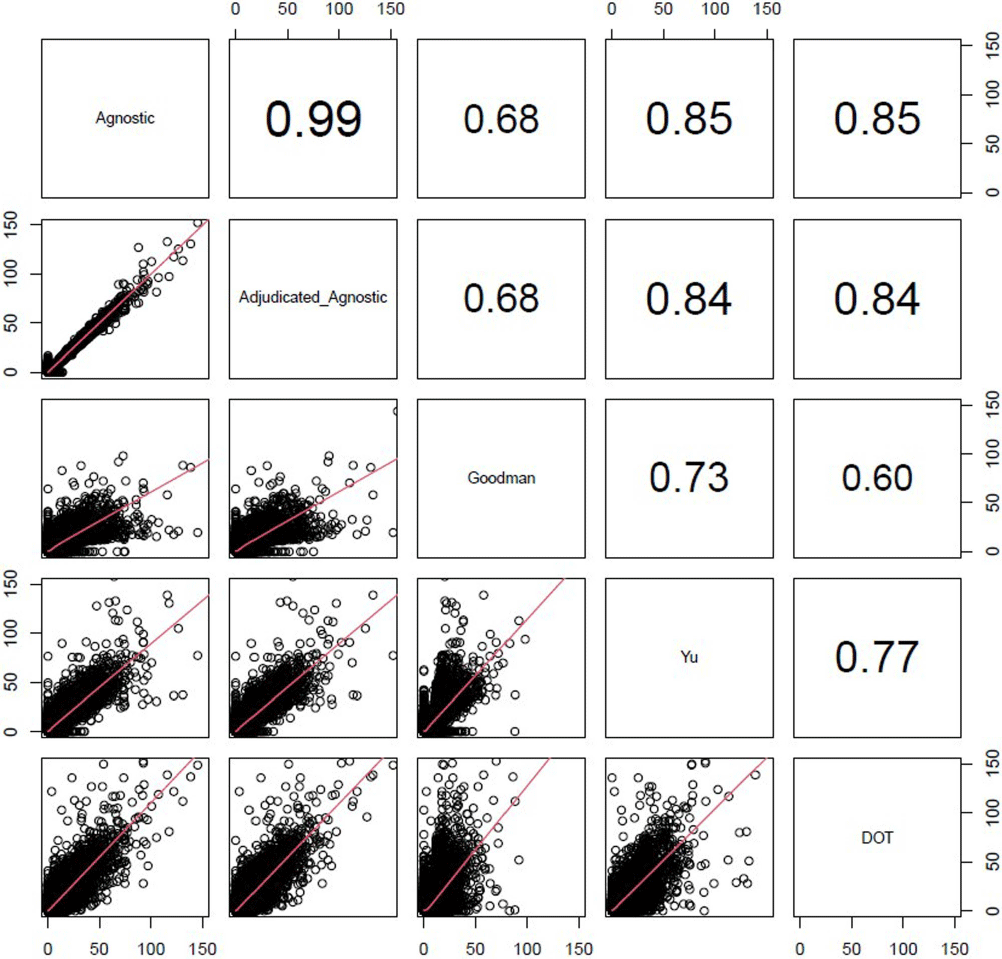
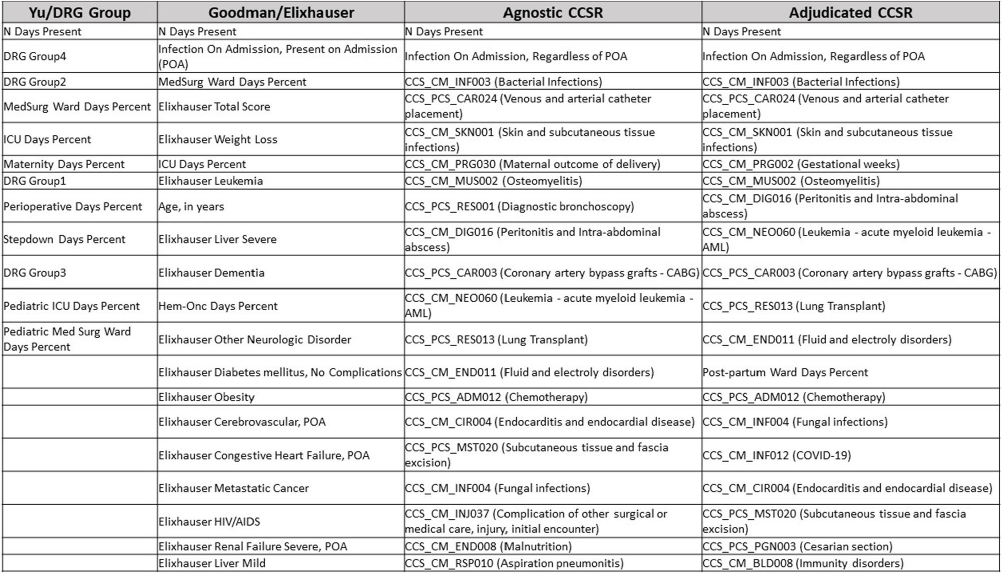
Background: External comparisons of antimicrobial use (AU) may be more informative if adjusted for encounter characteristics. Optimal methods to define input variables for encounter-level risk-adjustment models of AU are not established. Methods: This retrospective analysis of electronic health record data included 50 US hospitals in 2020-2021. We used NHSN definitions for all antibacterials days of therapy (DOT), including adult and pediatric encounters with at least 1 day present in inpatient locations. We assessed 4 methods to define input variables: 1) diagnosis-related group (DRG) categories by Yu et al., 2) adjudicated Elixhauser comorbidity categories by Goodman et al., 3) all Clinical Classification Software Refined (CCSR) diagnosis and procedure categories, and 4) adjudicated CCSR categories where codes not appropriate for AU risk-adjustment were excluded by expert consensus, requiring review of 867 codes over 4 months to attain consensus. Data were split randomly, stratified by bed size as follows: 1) training dataset including two-thirds of encounters among two-thirds of hospitals; 2) internal testing set including one-third of encounters within training hospitals, and 3) external testing set including the remaining one-third of hospitals. We used a gradient-boosted machine (GBM) tree-based model and two-staged approach to first identify encounters with zero DOT, then estimate DOT among those with >0.5 probability of receiving antibiotics. Accuracy was assessed using mean absolute error (MAE) in testing datasets. Correlation plots compared model estimates and observed DOT among testing datasets. The top 20 most influential variables were defined using modeled variable importance. Results: Our datasets included 629,445 training, 314,971 internal testing, and 419,109 external testing encounters. Demographic data included 41% male, 59% non-Hispanic White, 25% non-Hispanic Black, 9% Hispanic, and 5% pediatric encounters. DRG was missing in 29% of encounters. MAE was lower in pediatrics as compared to adults, and lowest for models incorporating CCSR inputs (Figure 1). Performance in internal and external testing was similar, though Goodman/Elixhauser variable strategies were less accurate in external testing and underestimated long DOT outliers (Figure 2). Agnostic and adjudicated CCSR model estimates were highly correlated; their influential variables lists were similar (Figure 3). Conclusion: Larger numbers of CCSR diagnosis and procedure inputs improved risk-adjustment model accuracy compared with prior strategies. Variable importance and accuracy were similar for agnostic and adjudicated approaches. However, maintaining adjudications by experts would require significant time and potentially introduce personal bias. If findings are confirmed, the need for expert adjudication of input variables should be reconsidered.
Disclosure: Elizabeth Dodds Ashley: Advisor- HealthTrackRx. David J Weber: Consultant on vaccines: Pfizer; DSMB chair: GSK; Consultant on disinfection: BD, GAMA, PDI, Germitec



UTI Symptomatology and Antibiotic Prescribing among US Veterans Seen in Outpatient Clinics
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s80
-
- Article
-
- You have access
- Open access
- Export citation
-
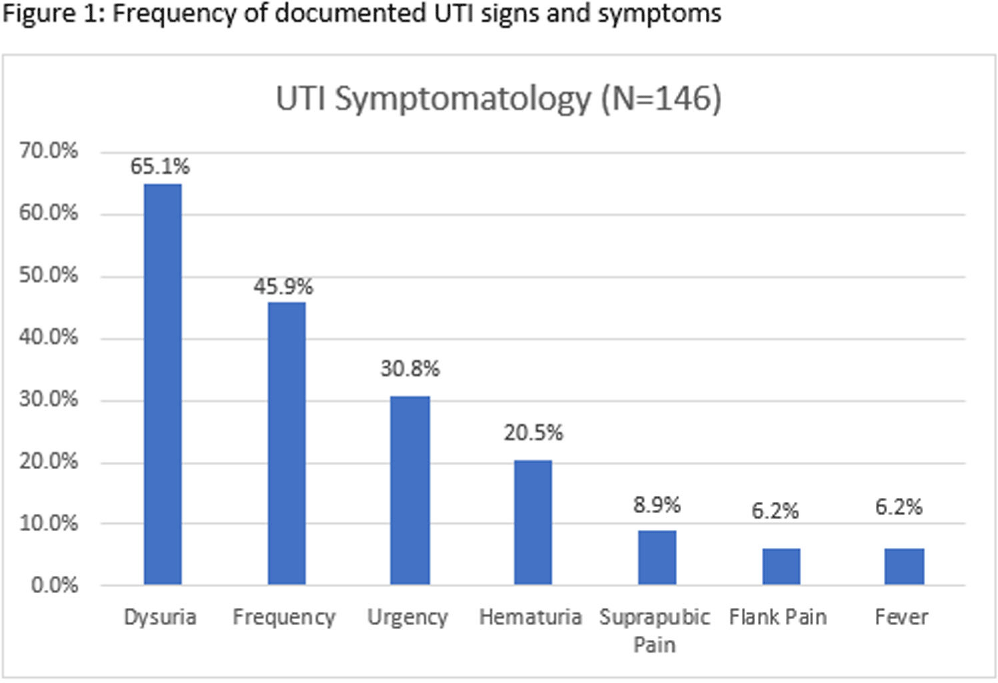
Background: Infectious Diseases Society of America guidelines recommend antibiotic prescribing for urinary tract infections (UTIs) when there is a positive culture and signs and symptoms of infection. Despite these guidelines, prescribing for asymptomatic bacteriuria remains prevalent. We conducted a chart review of UTI outpatient encounters to determine the prevalence of antibiotic prescribing as well as patient and provider factors associated with inappropriate prescribing for UTIs. Methods: Patients who were seen at any Department of Veterans Affairs (VA) outpatient clinic with a positive urine culture from 1/1/2019-12/31/2022 were evaluated for inclusion. Exclusion criteria were pregnancy, neutropenia, neurogenic bladder, spinal cord injury/disorder, chronic kidney disease stage III and above, and those undergoing urologic surgical procedures within 7 days. Inappropriate prescribing was defined as an antibiotic prescription given for UTI treatment when no signs or symptoms of infection were recorded during the patient encounter. Chi-square, Fisher’s exact and t-tests were used to evaluate the association between patient and provider characteristics and antibiotic prescribing. Results: Among 341 visits, most patients were male (70%), White (40%), older (mean age of 65.8 ± 15.9 years) and treated at an urban facility (57%). Antibiotics were prescribed for 67% (229/341) of visits. Of the 229 antibiotic courses prescribed, 119 (52%) were appropriate; issued to patients with > = 1 sign or symptom consistent with a urinary tract infection. The most common symptom recorded was dysuria, followed by frequency, urgency, and hematuria (Figure 1). The remaining 110 (48%) antibiotic prescriptions were inappropriate; given to patients without documented UTI-related signs or symptoms. The proportion of inappropriate prescribing was higher among advanced practice practitioners (39/56; 69%) compared to physicians (68/113; 60%; P < 0 .0001). Prescribing of an antibiotic did not differ by gender (p-value=0.3779), race (p-value=0.3972), age (p-value=0.7461) or urban versus rural geography (p-value=0.3647). Discussion: In outpatient clinics, nearly half of antibiotics prescribed to patients with a positive urine culture occurred in the absence of documented of signs or symptoms of a UTI. These results suggest that interventions to improve antibiotic use for UTI-related concerns in the outpatient setting should address UTI-related signs and symptoms as well as asymptomatic bacteriuria. Advanced practice practitioners were more likely to prescribe without documentation of relevant signs or symptoms than physicians. Improving meaningful documentation about the presence or absence of signs and symptoms of a UTI may help reduce inappropriate antibiotic prescriptions in the outpatient setting.
Disclosure: Robin Jump: Research support to my institution from Merck and Pfizer; Advisory boards for Pfizer

Does Serial Procalcitonin Monitoring predict Clinical Outcomes in Children with Sepsis? A diagnostic stewardship study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s82
-
- Article
-
- You have access
- Open access
- Export citation
-
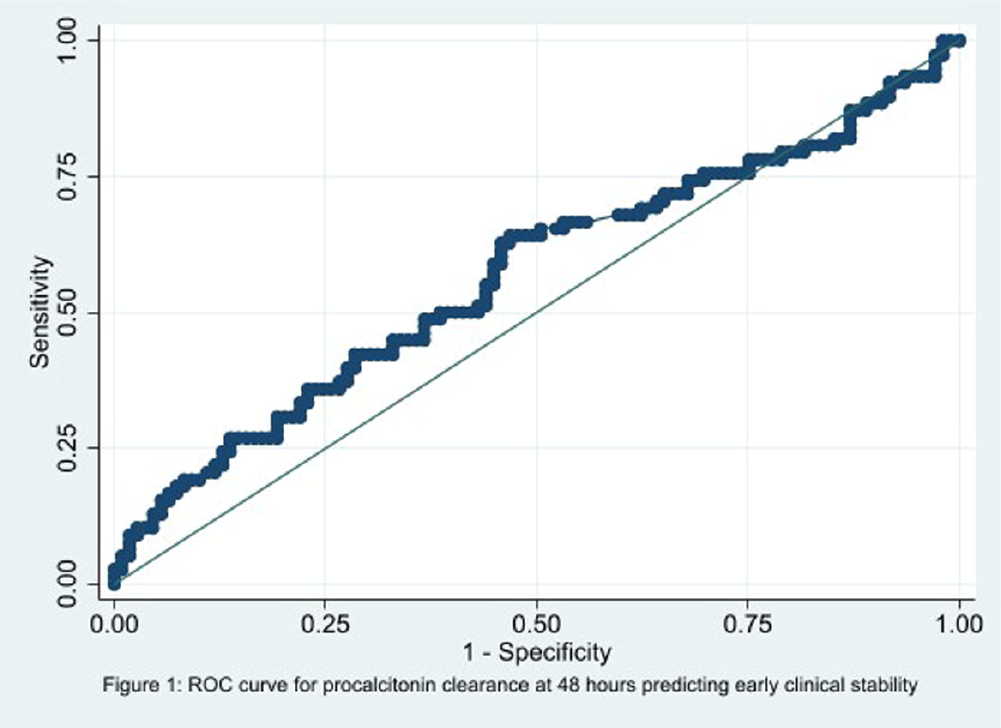
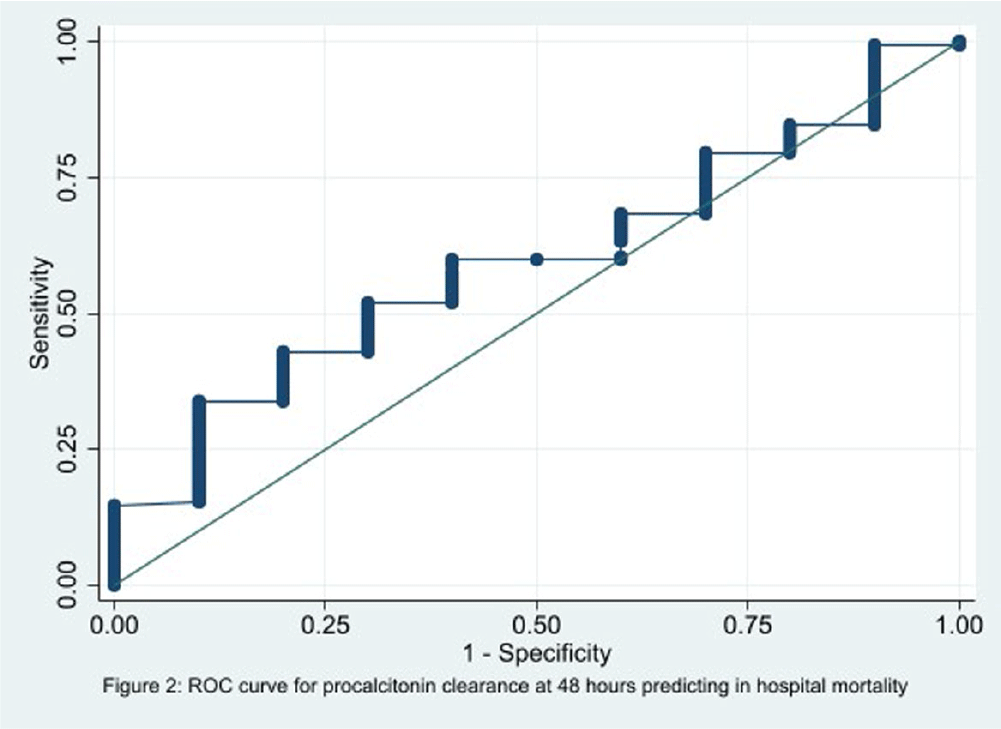
Background: In the management of children with sepsis, inflammatory markers are often obtained upon admission and repeated frequently. It is unclear if serial monitoring of procalcitonin is useful for predicting patient outcomes. The focus of our study is to identify if the trend of procalcitonin levels was predictive of the clinical outcomes in children with sepsis. Methods: We performed a retrospective diagnostic study to evaluate the association between change in procalcitonin levels and clinical outcomes. Encounters for children 1 to 8 years old with a sepsis ICD 10 diagnosis code and meeting the clinical sepsis criteria from May 2020 to May 2022 at one quaternary care pediatric hospital were included. Encounters with fewer than two procalcitonin values and children with autoimmune diseases, trauma, new onset malignancy, and fungal infections were excluded. Procalcitonin clearance at 48 hours (CL-PCT48) was defined as the difference in procalcitonin values drawn on admission and at 48 hours divided by initial procalcitonin value. The primary outcome was good early clinical response, defined as composite measure of temperature, hemodynamic stability, supplemental oxygen requirement, and need for renal replacement therapy at 120 hours of admission. All-cause in-hospital mortality was a secondary outcome. ROC analysis was performed to measure the correlation of CL-PCT48 and initial procalcitonin value (PCT0) with the outcome. Result: There were 320 unique encounters for children who met the clinical criteria of sepsis. The median number of procalcitonin measurements was 4 (Range 2 – 111). Of these encounters, 187 had procalcitonin measurements done at eligible times. The mean age of the study participants was 9 years and 8 months, 103 (55%) were male, and the majority (54%) were Caucasian. Fifty-seven (30%) individuals had bacterial growth from a culture from sterile body fluid or urine. 78 (41.7%) individuals had good early clinical response and 177 (94.7%) survived to hospital discharge. There was no correlation identified between CL-PCT48 and good early clinical response (area under ROC curve [AUC] = 0.57, 95% CI 0.48-0.65, Figure 1) or mortality (AUC = 0.60, 95% CI 0.43-0.76, Figure 2). There was also no correlation between PCT0 and good early clinical response (AUC = 0.47, 95% CI 0.39-0.56) or and mortality (AUC = 0.50, 95% CI 0.29-0.72). Conclusion: Procalcitonin clearance at 48 hours after admission did not predict early clinical response in children with sepsis.


Situations Predisposing Primary Care Patients to Use Antibiotics Without a Prescription in the United States
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s22
-
- Article
-
- You have access
- Open access
- Export citation
-
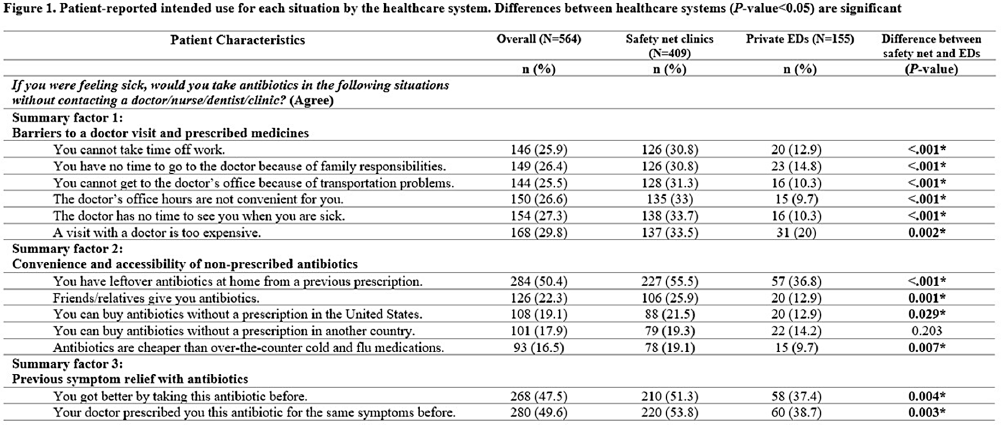
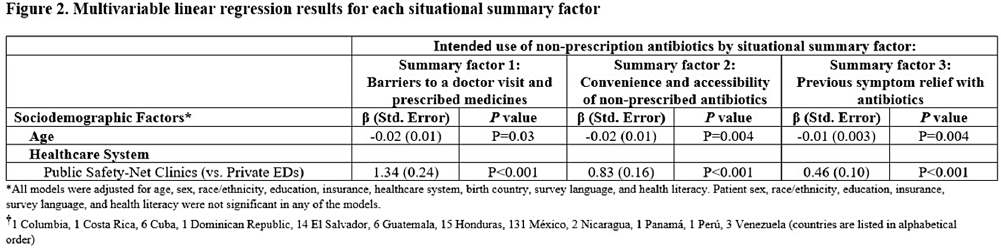
Background: Using antibiotics without medical guidance (non-prescription use) is a potential safety threat to individual and public health. Patients' situations can impact their intentions to use non-prescription antibiotics in the future (intended use). This survey (1) explores the dimensionality of 13 predefined situations to identify ‘summary factor,’ which include conceptually similar situations that influence patients’ intended use of non-prescription antibiotics, and (2) identifies the sociodemographic predictors associated with these summary factors. Methods: A cross-sectional survey was conducted from January 2020–June 2021 in the waiting rooms of six safety-net primary care clinics and two private emergency departments. We used principal component analysis as a data reduction technique and confirmed the factor structure of the situations (identifying three situational summary factors). Multivariate linear regression identified the sociodemographic predictors (e.g., age, gender, race, education, insurance, healthcare system, language preference, birth country, and health literacy) associated with each summary factor. Results: Of the 564 patients surveyed, the majority were female (72%), Hispanic or Latinx (47%), college-educated (44%), and received public health insurance (e.g., Medicaid or County Financial Assistance) (56%). The largest proportion of patients endorsed intended non-prescription antibiotic use for situations involving high doctor visit costs (29.8%), having leftover prescription antibiotics (50.4%), and experiencing symptom relief with prior use of antibiotics (47.5%) (Figure 1). We identified three situational summary factors: (1) perceived barriers to a doctor visit and receiving a prescription (Cronbach’s alpha [α]=0.96), (2) convenience and accessibility of non-prescription antibiotics (α=0.81), and (3) previous symptom relief with antibiotics (α=0.95). After controlling for gender, race, education, insurance, language preference, birth country, and health literacy, our multivariate regression results revealed that younger patients (P < 0 .04) and patients attending the safety-net health system (P < 0 .001) had more intended use of non-prescription antibiotics for all three summary factors (Figure 2). Conclusions: Our study revealed that younger patients and individuals receiving care from the safety-net clinics had an increased risk of intended non-prescription antibiotic use across all summary factors. Future stewardship interventions should consider the types of situations that drive patients' decisions to use antibiotics without a prescription. Interventions aimed at reducing barriers to healthcare (e.g., high costs and long waits associated with doctor appointments) and educating individuals on the risks associated with inappropriate antibiotic use while providing alternative (non-antibiotic) treatment options may reduce antibiotic use and antimicrobial resistance. Acknowledgments: This work is supported by grant number R01HS026901 from AHRQ and NRSA T-32 (6T32HC10031).
Disclosure: Barbara Trautner: Stock: Abbvie--sold in December 2023; Abbott Laboratories--sold in December 2023; -Bristol Myers Squibb--sold in December 2023; Pfizer--sold in December 2023; Consultant--Phiogen—consultant. Contracted research through NIAID for STRIVE trial, currently testing Shionogi product; Contracted research--Peptilogics; Contracted research--Genentech


A Deeper Look at Proposed Surveillance of Superficial Incision Surgical Site Infections (SSISSIs)
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s142
-
- Article
-
- You have access
- Open access
- Export citation
-
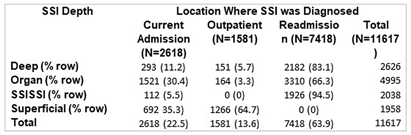
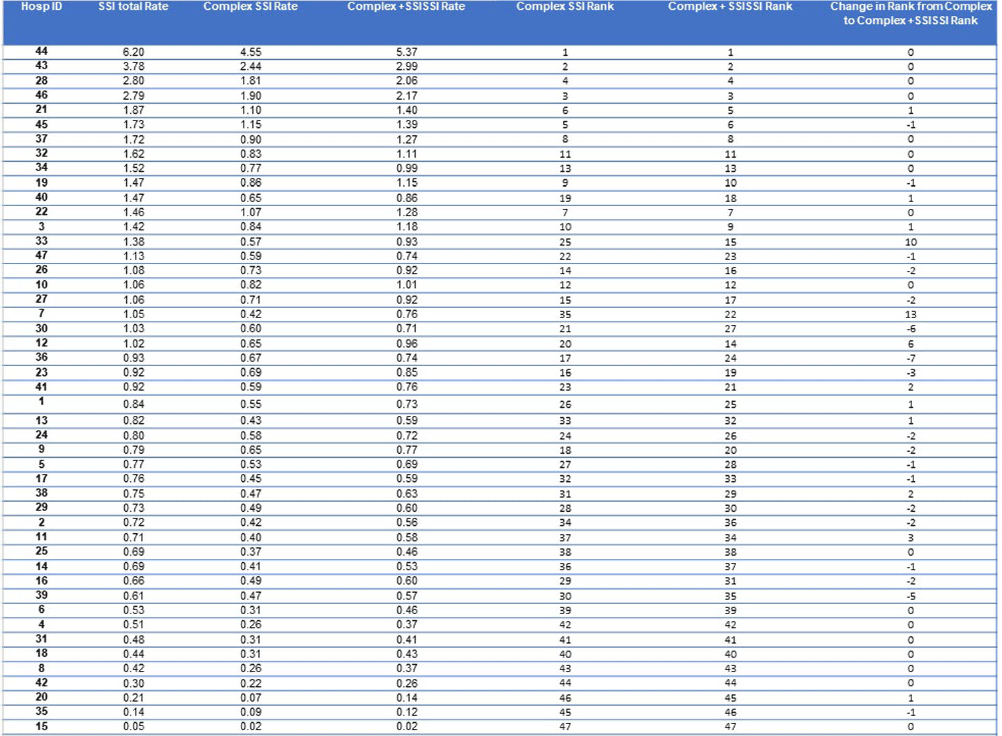
Although the National Healthcare Safety Network (NHSN) recommends the reporting of superficial incisional SSIs, the standardized infection ratio (SIR) models used by the NSHN exclude superficial incisional SSIs cases. Yet, some superficial incisional SSIs may lead to serious adverse patient outcomes. We previously proposed a new category of such infections: serious superficial incisional surgical site infections (SSISSIs), defined as a superficial incisional SSI that (1) required debridement in an operating room and/or (2) led to a hospital readmission within 30 days of surgery. The objective of our study was to determine the prevalence of SSISSIs in a large network of community hospitals and compare hospital rankings of SSI rates of organ/space and deep SSIs (complex SSIs) with and without SSISSIs. We performed a retrospective descriptive analysis of prospectively collected data on 35 NHSN surgical categories in 47 community hospitals within the Duke Infection Control Outreach Network (DICON) from 1/1/2013-12/31/2022. All hospitals used standardized surveillance and data collection strategies throughout the study period. The Wilcoxon rank-sum was used to test for differences in performance rankings of hospitals sorted by rates of complex SSIs alone compared to complex and SSISSI rates. A two-tailed P value of .05 or less was considered significant. Overall, 11,617 SSIs occurred after 1,272,257 surgeries (0.91 SSIs/100 procedures). Out of 3,996 superficial SSIs, 2,038 (17.5% overall, 51.0% of superficial incisional) met criteria for SSISSI. 112 (5.5%) were diagnosed during the current admission and required takeback to the OR for infection; 1,926 (94.5%) were diagnosed during a readmission; and 3841 (33.1%) were diagnosed during readmission and returned to the OR. (Table1) The highest proportion of SSISSIs was diagnosed in patients who underwent gastrointestinal surgery (32.0%) or orthopedic surgery (24.0%). (Table2) Performance ranking of individual hospitals based on rates of complex SSIs, differed significantly when including SSISSIs (p= 0.02). (Table3) Discussion Our findings suggest that SSISSIs make up a moderate but important proportion of SSIs in community hospitals. SSISSIs can be identified through established database surveillance looking at objective measures of returning to the OR for debridement and/or readmission within 30 days. Hospital rankings differed significantly when SSISSIs were added to complex SSIs to calculate SSI rates. As such, including SSISSIs likely provides a more accurate depiction of SSIs with important outcomes and is not as subjective to surveillance bias. Next steps would be specifically to look at outcomes data for complex SSIs compared to SSISSIs to fully evaluate the
Disclosure: Jessica Seidelman: UptoDate- Section Editor; BoneSupport- Consultant




Efficacy of Empiric Contact Precautions for Patients from High Risk Facilities
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s150
-
- Article
-
- You have access
- Open access
- Export citation
CAPILLARY LEVELLING OF THIN LIQUID FILMS OF POWER-LAW RHEOLOGY
- Part of
-
- Journal:
- The ANZIAM Journal / Volume 66 / Issue 1 / January 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. 62-76
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Impact of Universal Masking by Healthcare Personnel on Non-SARS-CoV-2 Healthcare-Associated Viral Respiratory Infections
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s141
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The impact of universal masking on transmission of endemic respiratory viruses in children’s hospitals is unknown. Our objective was to measure the association between universal masking by healthcare personnel and the incidence of non-SARS-CoV-2 healthcare-associated viral respiratory infections (HA-VRIs) in a free-standing academic pediatric medical center during the COVID-19 pandemic. Methods: In this quasi-experimental study, we measured the incidence rate of non-SARS-CoV-2 HA-VRIs (VRI diagnosed on or after hospital day 3 by one of several molecular assays) during three time periods: prior to the COVID-19 pandemic (pre-intervention: September 2013 - February 2020); during universal masking (intervention: May 2021 - March 2023); and after universal masking was lifted (post-intervention: April 2023 - November 2023). Although universal masking was implemented in late March 2020, we exclude the lockdown period of strict COVID-19-related public health mitigations (i.e., school closures and shelter-in-place advisories) during which community prevalence of non-SARS-CoV-2 respiratory viruses was minimal in our region (March 2020 to April 2021). By negative binomial regression analysis, we compared the level and trend of HA-VRIs between the pre-intervention and intervention periods. Results: Figure 1 illustrates the incidence rate of non-SARS-CoV-2 HA-VRI during the pre-intervention, lockdown, intervention, and post-intervention periods. The aggregate non-SARS-CoV-2 HA-VRI incidence rate during the pre-intervention, intervention, and post-intervention periods was 1.25, 1.84, and 1.96 HA-VRIs per 1000 patient days, respectively. There was no significant difference in the level (p = 0.96) or trend (p = 0.67) of HA-VRI incidence rate between the pre-intervention and intervention periods. Conclusion: Universal masking was not associated with a decrease in the incidence rate of non-SARS-CoV-2 HA-VRIs at our children’s hospital during the COVID-19 pandemic. These findings suggest that universal masking may not be an effective infection prevention measure in children’s hospitals during periods of increased endemic respiratory viral transmission in the community.
Disclosure: Larry Kociolek: Research Support - Merck


Improving Data Quality from a Hematology Unit Hand Hygiene Observation Program
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s99-s100
-
- Article
-
- You have access
- Open access
- Export citation
-
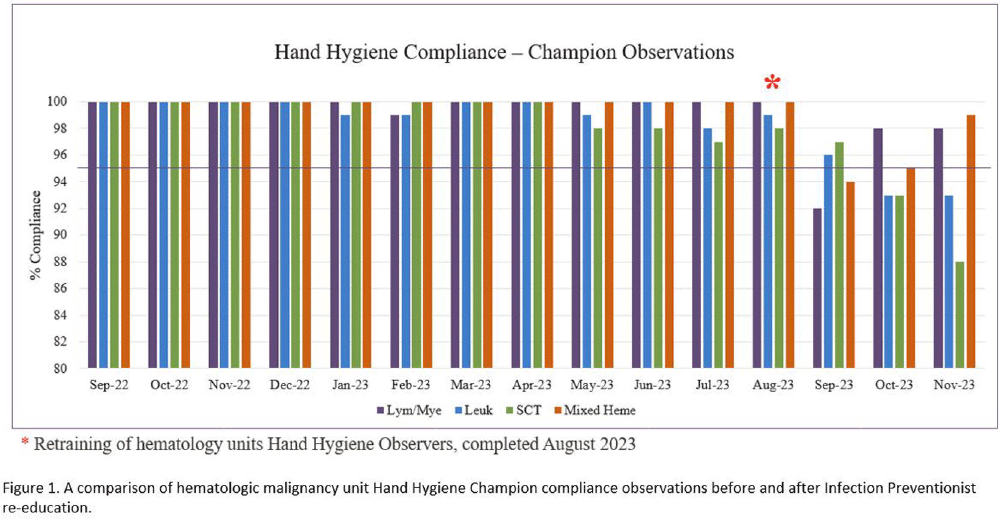
Background: For United States healthcare programs to be fully compliant with Joint Commission National Patient Safety Goal (NPSG) #7, organizations must implement and maintain a hand hygiene (HH) program that follows either the current Centers for Disease Control and Prevention (CDC) or the current World Health Organization (WHO) HH guidelines. Joint Commission standard IC.03.01.01 requires these organizations to provide metrics that evaluate the effectiveness of their program and program goals. Our center utilizes the direct observation method with the use of over 550 Hand Hygiene Observers (HHO) to collect our HH compliance. HHO are trained with a computer-based course that requires passing a post-education test. During fiscal year 2023 (FY23), Infection Control surveillance noted an increase in hospital-acquired infections (HAI) Clostridioides difficile infections (CDI), catheter-associated urinary tract infections (CAUTI), and multidrug-resistant organisms (MDRO) on our hematologic malignancy units (HM), which initiated an Infection Control (IC) investigation into possible causes. Increased rounding by our Infection Preventionist (IP) observed that HH compliance was much lower than unit HHO reported rates. Inquiries into this data discrepancy revealed barriers to accurate reporting, including HHO having low confidence in identifying and reporting non-compliant behavior. To that end, we conducted mandatory re-training of all HM HHO with the primary goal of improving the quality of our HH compliance data and addressing barriers with non-compliance reporting. Our secondary goal was to identify areas of improvement in institutional HH rates. Methods: In August 2023, 252 HM staff and HHO received detailed, in-person retraining by the HM IP. Training included reviewing the discrepancy in HHO and IP observations, potential causes of discrepancy, most commonly missed HH opportunities, examples of correct and incorrect HH practices, and addressing staff questions. Results: Following mandatory re-training of HM HHO, HH compliance for our HM units from September 2023 – December 2023 ranged from 89% to 98%, with increased reporting of non-compliance (Figure 1). A detailed dashboard was created that focused on HM HH compliance, containing the HHO observations and non-compliant reports. Conclusion: A one-time in-person retraining of HM HHO by our IP has led to an improvement in data quality, which is imperative for future quality improvement initiatives. Improving our HH data quality allowed IC to identify and provide actionable feedback to HM leaders, create targeted interventions to improve HAI rates, and improve patient safety. Future goals include retaining of all HHO and a HH campaign to ensure patient safety across our institution.

Carbapenemase-Producing Enterobacteriaceae detected in a Large Canadian Tertiary Care Hospital: Five-year retrospective study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, p. s157
-
- Article
-
- You have access
- Open access
- Export citation
