Refine listing
Actions for selected content:
142466 results in Open Access
The opportunity for e-mental health to overcome stigma and discrimination
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S549-S550
-
- Article
-
- You have access
- Open access
- Export citation
Psychosomatic relationships between the state of mental health and the level of vital threat of dermatological disease
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S370-S371
-
- Article
-
- You have access
- Open access
- Export citation
Cognitive complaints in schizophrenia:relationship with clinical symptoms, stigma and insight
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S757
-
- Article
-
- You have access
- Open access
- Export citation
Evaluation of adherence to treatment in patients with anxious-depressive syndrome.
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S674-S675
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Treatment-resistant depression can pose a major challenge to mental health professionals, both in identifying cases and in devising consequent therapeutic strategies (1). However, it is not uncommon that the lack of response to antidepressant treatment is actually due to non-adherence to it in many cases (2).
ObjectivesIn this context, it would be interesting to know the rate of abandonment of antidepressant treatment in patients with anxious-depressive symptomatology, since the patient’s evolution may depend entirely on this.
MethodsTo this end, the psychiatry service of the Hospital Clínico Universitario de Valladolid has collected data on adult patients who come for a first consultation in the mental health team, referred for presenting symptoms of anxiety and depression.
These data have been recorded over the last 2 years, including different socio-demographic and clinical variables. Subsequently, a descriptive analysis was carried out, the preliminary results of which are presented below.
ResultsWe started from a sample of 222 patients at the present time: 69 men and 153 women, which is in accordance with previous data on the prevalence of anxiety disorders and depression by gender (3).
Antidepressant treatment was prescribed (from psychiatry or primary care) in 80% of them. A review 6 months later showed that up to 1/3 of these patients (34%) had abandoned treatment on their own before completing this period, as can be seen in the first graph (image 1), which is contemplated in several guidelines and recommendations in the scientific literature (4). No major differences were observed between genders for treatment indication or treatment abandonment.
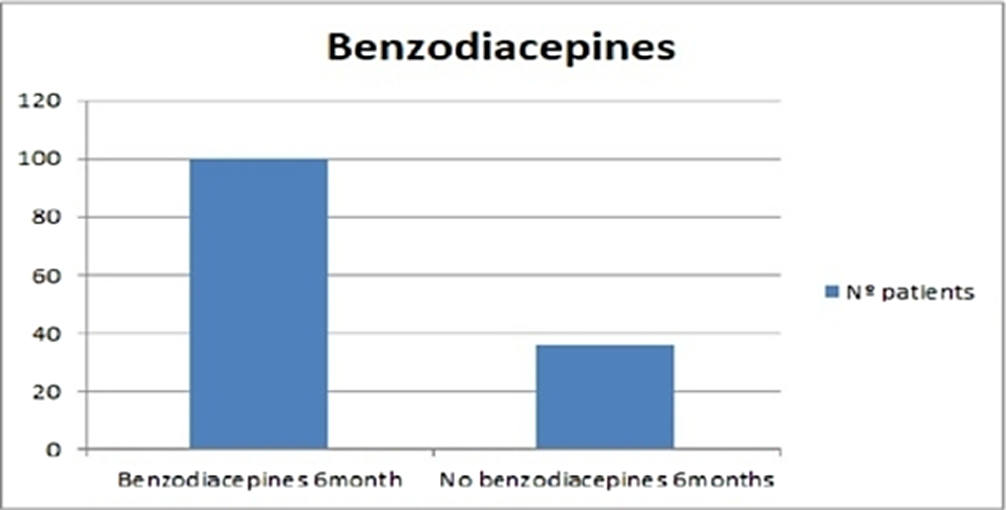
On the other hand, 61% of the patients in the sample had been treated with benzodiazepines. Among them, up to 74% were still taking these drugs 6 months later (image 2). This result is striking, since in reality, the duration of treatment with benzodiazepines should be much shorter, according to the latest reviews (5).
Finally, cross-checking these data, it was observed that for 116 patients (52% of the total) the initial treatment included antidepressants and benzodiazepines. At 6 months, 18 of these patients (16%) had voluntarily discontinued the antidepressant, but continued with benzodiazepines.
Image:
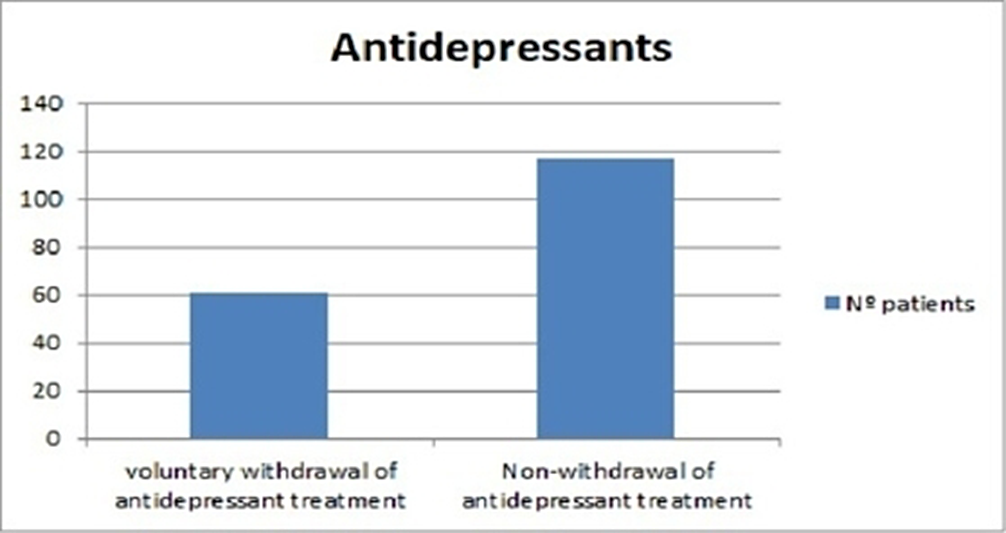
Image 2:
 Conclusions
ConclusionsIt is very important to review adherence to treatment in all patients, especially in those cases in which the persistence of symptoms makes us think of a possible resistant depression. For this reason, it would be advisable to try to establish an adequate doctor-patient relationship that allows trust in the therapist and communication between both and leads to a favorable evolution.
Disclosure of InterestNone Declared


Experience in the Psychotherapeutic Treatment of Eating Disorders in Children and Adolescents: A Brief Approach and EMDR Outcomes
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S460
-
- Article
-
- You have access
- Open access
- Export citation
Do antidepressants lead to weight-increase? Antidepressant therapy and long-term changes in body mass index, waist circumference and fat mass - A prospective, population-based study
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S24-S25
-
- Article
-
- You have access
- Open access
- Export citation
War and Migration – when Mental Health is left behind
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S614
-
- Article
-
- You have access
- Open access
- Export citation
Case Report and Literature review. Neuropsychiatry Manifestation of Frontal Lobe Neoplasm- Meningioma. Prevalence, Presentation and Pathogenesis
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S646
-
- Article
-
- You have access
- Open access
- Export citation
Effects of light therapy in the anxious-depressive clinic
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S533
-
- Article
-
- You have access
- Open access
- Export citation
Typology of hyperthymic personalities with affective phases
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S656-S657
-
- Article
-
- You have access
- Open access
- Export citation
The future of psychiatry and psychotherapy - An Early Career psychiatrist’s view
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S819
-
- Article
-
- You have access
- Open access
- Export citation
Co-design of a digital violence prevention and management tool for psychiatric inpatient care: focus on supporting integration into electronic health record system
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S59
-
- Article
-
- You have access
- Open access
- Export citation
The activity of platelet enzymes and subpopulation composition of monocytes in schizophrenia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S688
-
- Article
-
- You have access
- Open access
- Export citation
Social determinants of involuntary psychiatric hospital admissions in Ontario, Canada
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S335
-
- Article
-
- You have access
- Open access
- Export citation
Exploring the connections between psychiatric disorders and climate change
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S472
-
- Article
-
- You have access
- Open access
- Export citation
Childhood socio-economic disadvantages versus adverse care experiences: Mediation and moderation impacts on late-life depressive symptoms
- Part of
-
- Journal:
- European Psychiatry / Volume 67 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 27 August 2024, e47
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cyber victimisation and depression among adolescents in Tunisia: a case report study and review of literature
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S449-S450
-
- Article
-
- You have access
- Open access
- Export citation
Increased emergency room visits without corresponding rehospitalizations in cannabis users with psychosis
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S388-S389
-
- Article
-
- You have access
- Open access
- Export citation
Short-term memory depends on the level of emotional burnout
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S380
-
- Article
-
- You have access
- Open access
- Export citation
Responses to serious adverse incidents in mental health care settings: a qualitative study of a complex patient safety system
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S610-S611
-
- Article
-
- You have access
- Open access
- Export citation
