EHRs contain a rich source of real-world data that can support evidence generation to better understand mental disorders and improve treatment outcomes. However, EHR datasets are complex and include unstructured free text data that are time consuming to manually review and analyse. We present NeuroBlu, a secure, cloud-based analytic tool that includes bespoke NLP software to enable users to analyse large volumes of EHR data to generate real-world evidence in mental healthcare.

(i) To assemble a large mental health EHR dataset in a secure, cloud-based environment.
(ii) To apply NLP software to extract data on clinical features as part of the Mental State Examination (MSE).
(iii) To analyse the distribution of NLP-derived MSE features by psychiatric diagnosis.
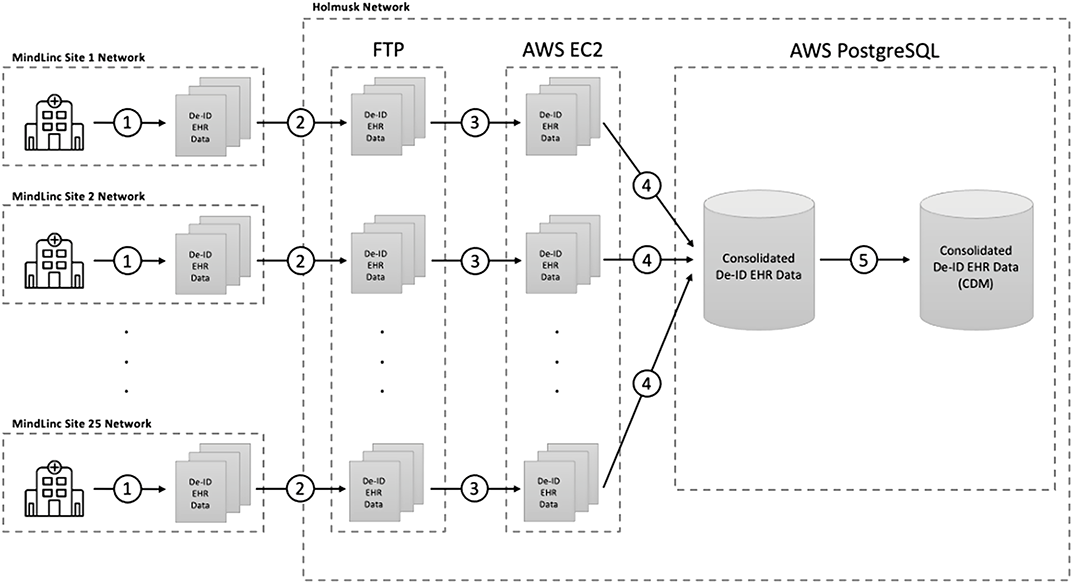
EHR data from 25 U.S. mental healthcare providers were de-identified and transformed into a common data model. NLP models were developed to extract 241 MSE features using a deep learning, long short-term memory (LSTM) approach. The NeuroBlu tool (https://www.neuroblu.ai/) was used to analyse the associations of MSE features in 543,849 patients.
The figure below illustrates the percentage of patients in each diagnostic category with at least one recorded MSE feature.
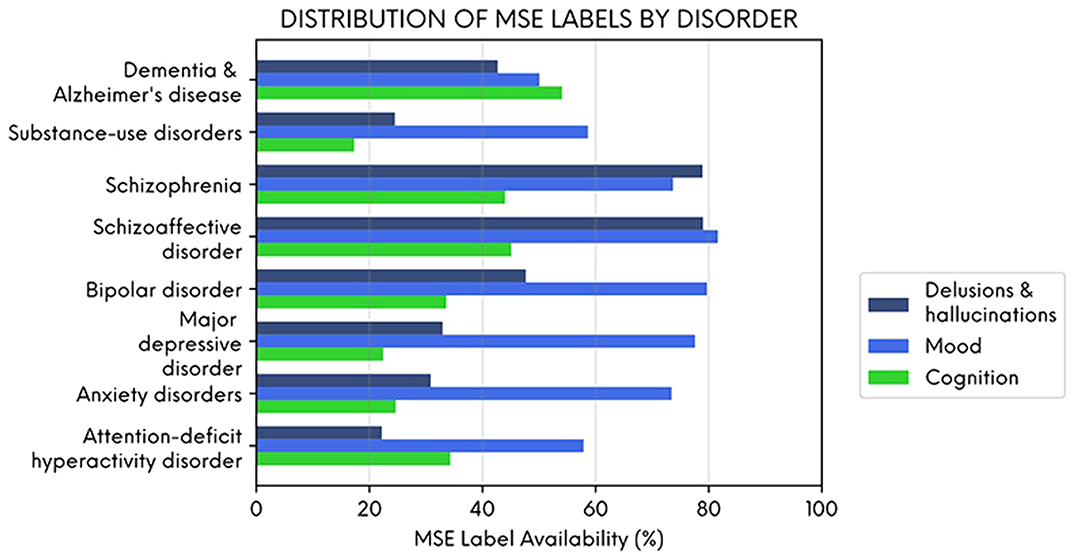
Delusions and hallucinations were more likely to be recorded in people with schizophrenia and schizoaffective disorder, and cognitive features were more likely to be recorded in people with dementia. However, mood symptoms were frequently recorded across all diagnoses illustrating their importance as a transdiagnostic clinical feature. NLP-derived clinical information could enhance the potential of EHR data to generate real-world evidence in mental healthcare.
This study was funded in full by Holmusk.
Anticholinergic medications block cholinergic transmission. The central effects of anticholinergic drugs can be particularly marked in patients with dementia. Furthermore, anticholinergics antagonise the effects of cholinesterase inhibitors, the main dementia treatment.
This study aimed to assess anticholinergic drug prescribing among dementia patients before and after admission to UK acute hospitals.
352 patients with dementia were included from 17 hospitals in the UK. All were admitted to surgical, medical or Care of the Elderly wards in 2019. Information about patients’ prescriptions were recorded on a standardised form. An evidence-based online calculator was used to calculate the anticholinergic drug burden of each patient. The correlation between two subgroups upon admission and discharge was tested with Spearman’s Rank Correlation.
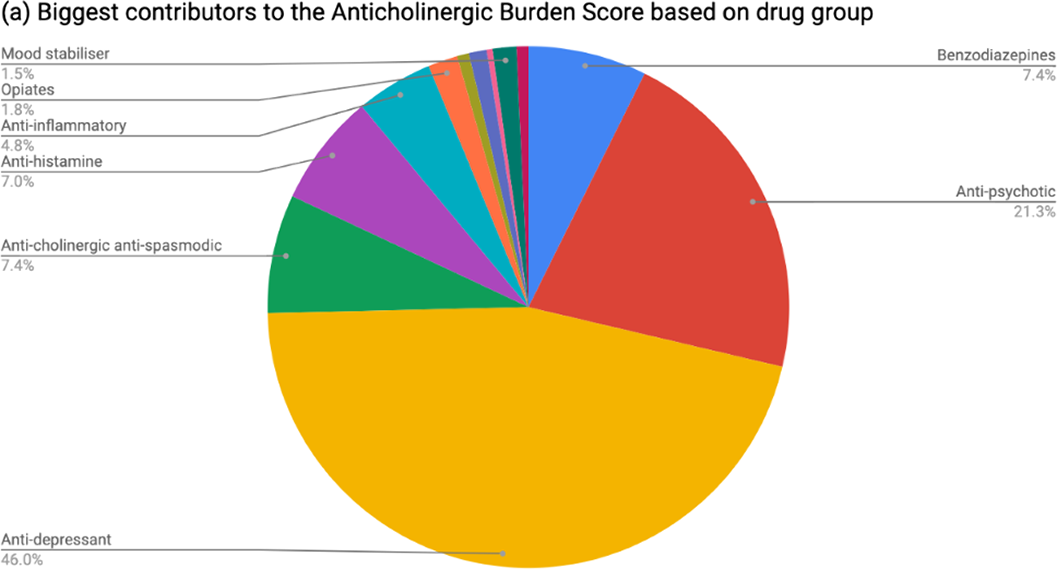
Table 1 shows patient demographics. On admission, 37.8% of patients had an anticholinergic burden score ≥1 and 5.68% ≥3. At discharge, 43.2% of patients had an anticholinergic burden score ≥1 and 9.1% ≥3. The increase was statistically significant (rho 0.688; p=2.2x10-16). The most common group of anticholinergic medications prescribed at discharge were psychotropics (see Figure 1). Among patients prescribed cholinesterase inhibitors, 44.9% were also taking anticholinergic medications.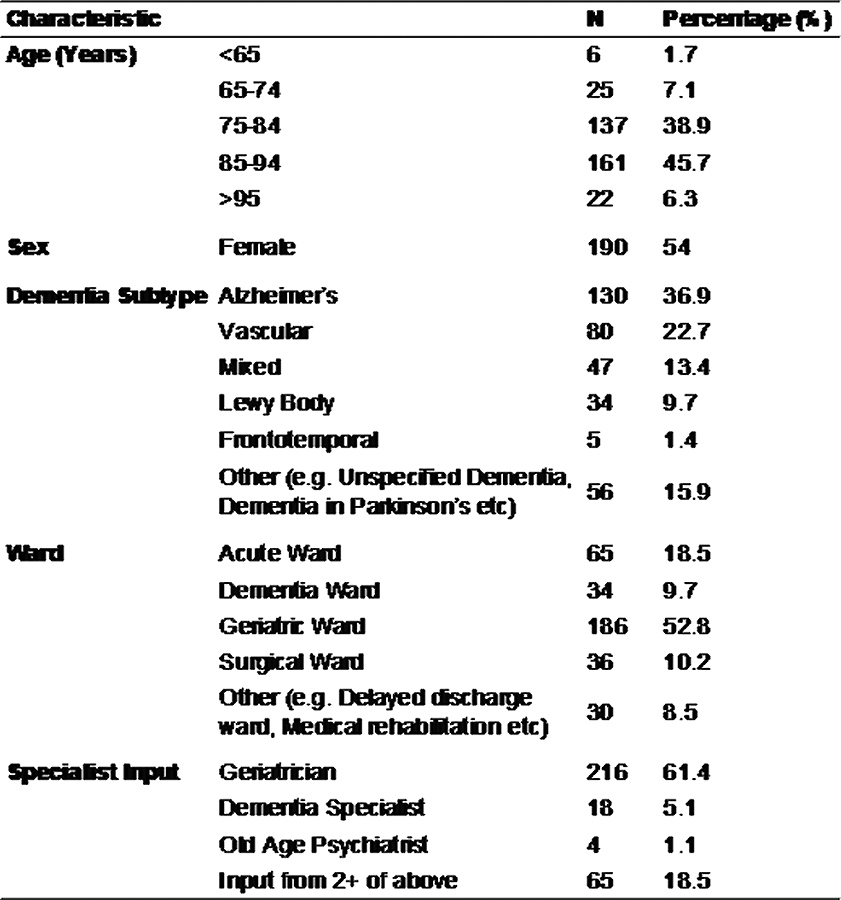
This multicentre cross-sectional study found that people with dementia are frequently prescribed anticholinergic drugs, even if also taking cholinesterase inhibitors, and are significantly more likely to be discharged with a higher anticholinergic drug burden than on admission to hospital.
This project was planned and executed by the authors on behalf of SPARC (Student Psychiatry Audit and Research Collaborative). We thank the National Student Association of Medical Research for allowing us use of the Enketo platform. Judith Harrison was su

