Data from an RCT of IAPT Norway (“Prompt Mental Health Care” [PMHC]) were linked to several administrative registers up to five years following the intervention. The aims were to (1) examine the effects of PMHC compared to treatment-as-usual (TAU) on work-related outcomes and health care use, (2) estimate the cost–benefit of PMHC, and (3) examine whether clinical outcomes at six-month follow-up explained the effects of PMHC on work−/cost–benefit-related outcomes.
RCTs with parallel assignment were conducted at two PMHC sites (N = 738) during 2016/2017. Eligible participants were considered for admission due to anxiety and/or depression. We used Bayesian estimation with 90% credibility intervals (CI) and posterior probabilities (PP) of effects in favor of PMHC. Primary outcome years were 2018–2022. The cost–benefit analysis estimated the overall economic gain expressed in terms of a benefit–cost ratio and the differences in overall public sector spending.
The PMHC group was more likely than the TAU group to be in regular work without receiving welfare benefits in 2019–2022 (1.27 ≤ OR ≤ 1.43). Some evidence was found that the PMHC group spent less on health care. The benefit–cost ratio in terms of economic gain relative to intervention costs was estimated at 5.26 (90%CI  $ - $1.28, 11.8). The PP of PMHC being cost-beneficial for the economy as a whole was 85.9%. The estimated difference in public sector spending was small. PMHC effects on work participation and cost–benefit were largely explained by PMHC effects on mental health.
$ - $1.28, 11.8). The PP of PMHC being cost-beneficial for the economy as a whole was 85.9%. The estimated difference in public sector spending was small. PMHC effects on work participation and cost–benefit were largely explained by PMHC effects on mental health.
The results support the societal economic benefit of investing in IAPT-like services.

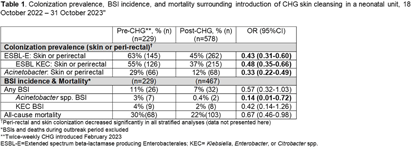
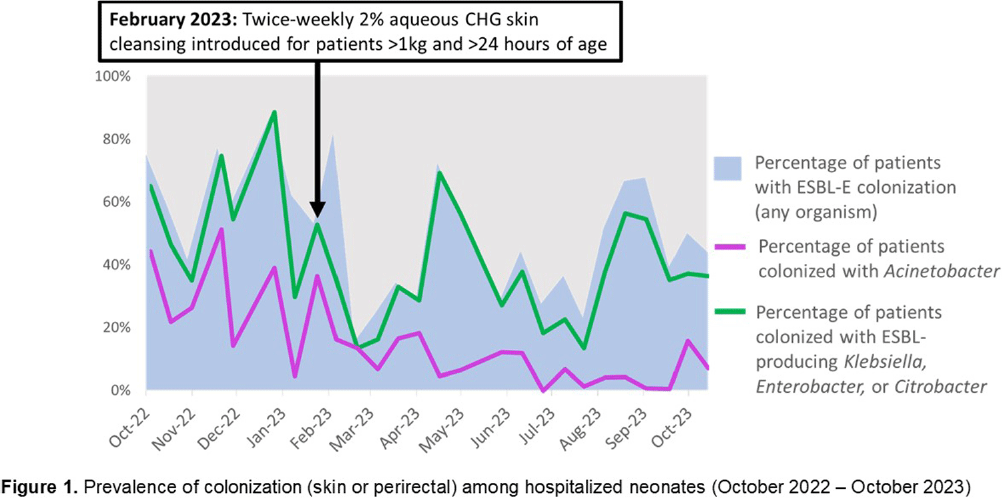
Background: Multidrug-resistant Gram-negative bacteria are a major cause of sepsis among hospitalized neonates globally. Aqueous chlorhexidine gluconate (CHG) skin antisepsis has been shown to be safe for use in infants; however, its sustained effectiveness in preventing Gram-negative pathogen colonization, bloodstream infection (BSI), and mortality is unclear. Methods: We conducted a period prevalence survey, with 26 sampling events over 12 months (18 October 2022 – 31 October 2023) at a 33-bed neonatal unit in a tertiary public hospital in Botswana where ESBL-producing Klebsiella pneumoniae and carbapenem-resistant Acinetobacter baumannii are leading causes of BSI. Perirectal and periumbilical skin swabs were collected every two weeks from all inpatients. Swabs were inoculated onto chromogenic media selective and differential for extended-spectrum beta-lactamase producing Enterobacterales (ESBL-E) and Acinetobacter spp. (CHROMagar™ ESBL, Acinetobacter). Colonization status was determined based on culture growth and colony morphology. Contemporaneous data on all-cause mortality and BSI were abstracted from routine surveillance records. Pre- and post-CHG prevalences were compared using a simple Chi-square test. During the surveillance period, an outbreak of K. pneumoniae linked to contaminated multi-use vials was detected, thus BSIs and deaths during the outbreak period (2 February–6 April, 2023) were excluded. In February 2023, the hospital infection prevention and control (IPC) team introduced twice-weekly whole-body cleansing with commercially available 2% aqueous CHG, performed by caregivers and healthcare workers on neonates >24 hours old and weighing ≥1 kg until discharge. Results: There were significant decreases in ESBL-E and Acinetobacter skin and perirectal colonization following the CHG intervention (Table 1; Figure 1). After the CHG intervention, the incidence of Acinetobacter BSIs declined significantly and there was a trend toward a decline in other BSIs and mortality. No adverse events associated with CHG were reported. Conclusions: Twice-weekly CHG application was temporally associated with significant reductions in neonatal ESBL-E and Actinetobacter skin and perirectal colonization and Acinetobacter BSI. This analysis was limited by a short pre-intervention surveillance period and thus may have been influenced by confounders such as seasonality, and intensified IPC efforts following the outbreak. Analysis of the routine CHG use in other settings and over longer surveillance periods are needed to better understand its effectiveness as an IPC strategy in settings where neonatal sepsis incidence is high. Table 1. Colonization prevalence, BSI incidence, and mortality surrounding introduction of CHG skin cleansing in a neonatal unit, 18 October 2022 – 31 October 2023.
Background: A vital role of hospital employee health is the management, characterization, and targeted prevention of bloodborne pathogen exposures (BPPE) among healthcare workers. A comprehensive review of a health center’s BPPE over time was conducted to identify areas for improvement and target education and training, given changes in BBPE standard operating procedures (SOPs) over time. Methods: A retrospective descriptive analysis was conducted on deidentified BBPE cases reported to employee health at VA Connecticut Healthcare System from 1995-2023 (N=296) using R statistical software. Results: The highest number of BBPE occurred among trainee physicians (N=103, 34.8%, especially surgery and internal medicine), registered nurses (N=60, 20.3%), and non-trainee physicians (N=45, 15.2%). The most frequently implicated devices were hollow-bore (N=103, 34.8%) and suture needles (N=60, 20.3%). Most BBPE occurred during surgical procedures (N=114, 38.5%) or medication administration (N=52, 17.6%). Over half of BBPE occurred during afternoons/nights (N=172, 58.1%). Over half occurred with use of personal protective equipment (PPE) (N=181, 61.1%). The majority of BBPE implicated finger injuries (N=220, 74.3%). Blood was the most frequently reported exposure (N=127, 42.9%), a similar percentage of records did not specifically name a body fluid type (N=121) or whether PPE was used (N=110). In most cases, the source patient was identified (N=282, 95.3%) and tested (N=272, 91.9%). Forty-three sources (14.5%) had positive BBP testing, which included HIV (N=14, 4.7%), hepatitis C (N=23, 7.8%), and hepatitis B (N=6, 2.0%). Most employees presented to employee health for initial evaluation (N=231, 78%) and underwent post-exposure testing (N=266, 89.9%); most had evidence of immunity to hepatitis B (N=246, 83.1%). Eighty-three employees (28%) received HIV PEP (average=1.9 days). Most records did not indicate if this was a first-time BBPE (N=250, 84.5%). No employee records indicated seroconversion for a bloodborne pathogen. Conclusions: Physicians and RNs, those performing surgical procedures and administering medications, and those on second and third shifts are at highest risk and may benefit from additional interventions such as exposure assessment or education. Required recordkeeping has been variable over time. Updated national SOPs have been adapted to employee health, though additional details could be considered for quality improvement purposes, such as duration of employment, level of training, and prior BBPE prevention education. It is unclear if some information such as history of BBPE or PPE use was elicited but not documented – this information could be helpful in management of BBPEs.






