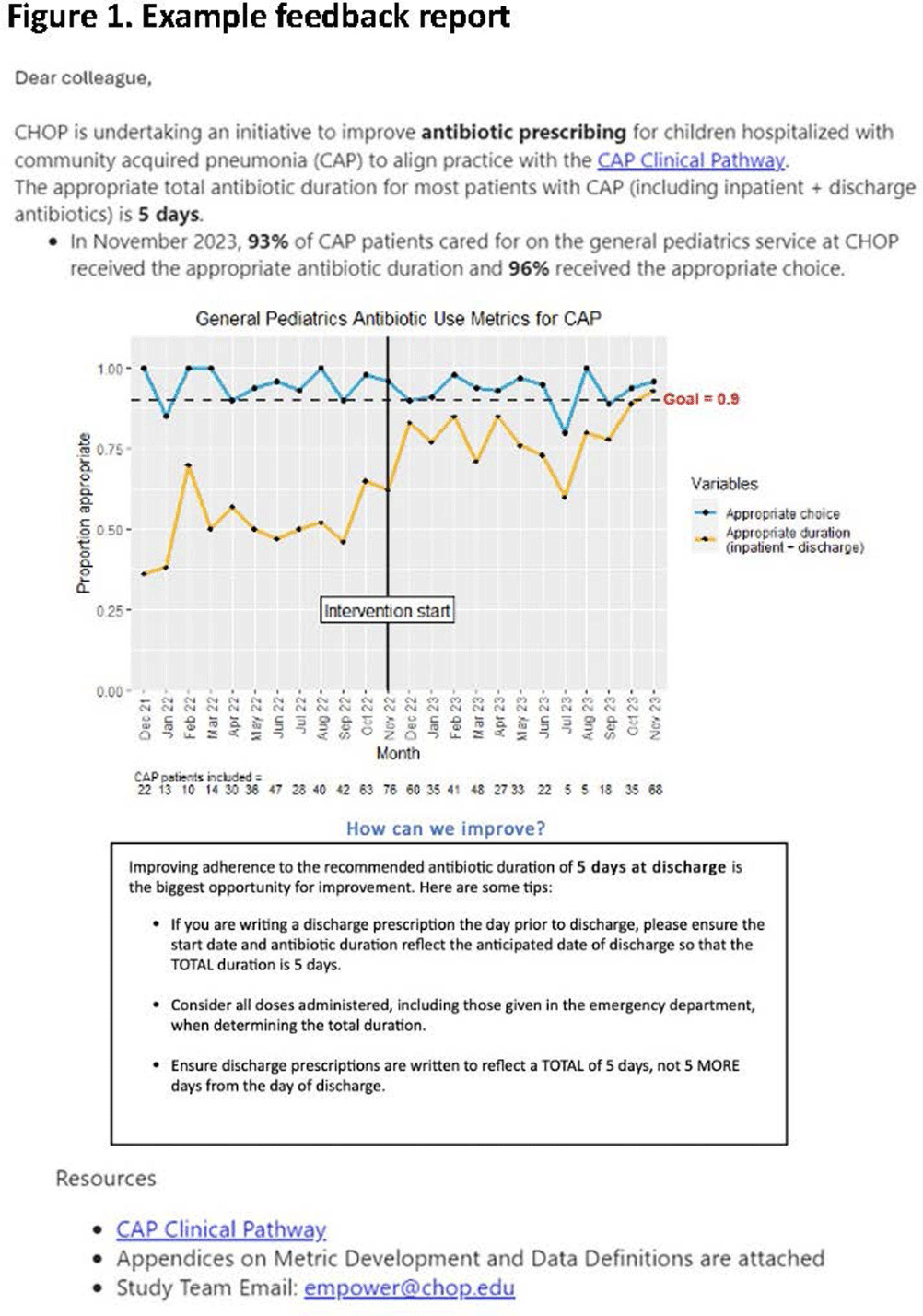
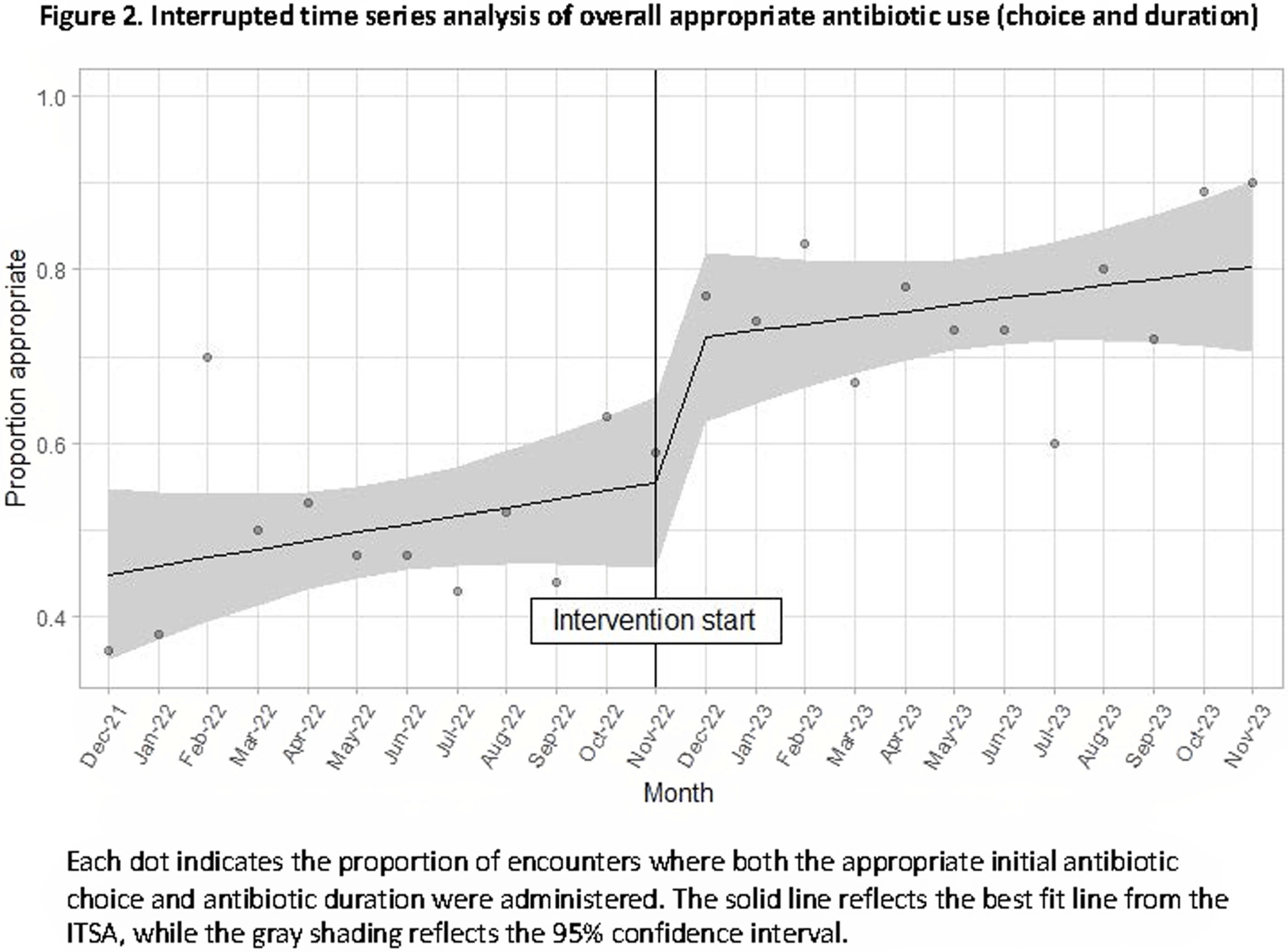
Background: Feedback reports summarizing clinician performance are effective tools to improve antibiotic stewardship in the ambulatory setting, but few studies have evaluated their effectiveness for pediatric inpatients. We developed and implemented feedback reports reflecting electronically-derived measures of appropriate antibiotic choice and duration for community acquired pneumonia (CAP) and measured their impact on appropriate antibiotic use in children hospitalized for CAP. Methods: We performed a single center quasi-experimental study including children 6 months to 17 years hospitalized for CAP between 12/1/2021-11/30/2023. Children with chronic medical conditions, ICU stays >48 hours, and outside transfers were excluded. The intervention occurred in 11/2022 and included clinician education, a monthly group-level feedback report disseminated by email (Figure 1), and a monthly review of clinician performance during a virtual quality improvement meeting. Patient characteristics were compared using chi-square or Wilcoxon rank sum tests. Interrupted time series analysis (ITSA) was used to measure the immediate change in the proportion of CAP encounters receiving both the appropriate antibiotic choice and duration, as well as the change in slope from the preintervention to the postintervention periods. Choice and duration were analyzed separately using ITSA as a secondary analysis. Results: There were 817 CAP encounters, including 420 preintervention and 397 postintervention. Patients admitted in the postintervention period were older (median age 2 years vs 3 years, P=0.03), but otherwise there were no differences in race, ethnicity, sex, ICU admission, or complicated pneumonia. Preintervention, 52% of encounters received both the appropriate antibiotic choice and duration; 96% of encounters received the appropriate antibiotic choice and 54% received the appropriate duration. The ITSA demonstrated an immediate 16% increase in the proportion of patients receiving both appropriate antibiotic choice and duration (95% confidence interval, 1-31%; P = 0.047) and no significant further increase over time following the intervention (P = 0.84) (Figure 2). When antibiotic choice was analyzed separately by ITSA, there was no immediate change or change over time in the proportion of patients receiving the appropriate antibiotic choice. In the ITSA of duration alone, there was an immediate 17% increase in the proportion receiving the appropriate duration (95% confidence interval, 2-33%; P = 0.03) and no change over time. Conclusion: Feedback reports generated from electronically-derived metrics of antibiotic choice and duration, combined with ongoing clinician education, increased the proportion of children with CAP treated with the appropriate antibiotic duration. Electronic feedback reports are a scalable and impactful intervention to improve antibiotic use in children hospitalized with CAP.
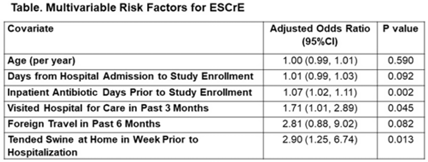
Background: The epidemiology of extended-spectrum cephalosporin-resistant Enterobacterales (ESCrE) in hospitalized patients in low- and middle-income countries (LMICs) is poorly described. Although risk factors for ESCrE clinical infection have been studied, little is known of the epidemiology of ESCrE colonization. Identifying risk factors for ESCrE colonization, which can predispose to infection, is therefore critical to inform antibiotic resistance reduction strategies. Methods: This study was conducted in 3 hospitals located in 3 districts in Botswana. In each hospital, we conducted ongoing surveillance in sequential units hospitalwide. All participants had rectal swabs collected which were inoculated onto chromogenic media followed by confirmatory testing using MALDI-TOF MS and VITEK-2. Data were collected via interview and review of the inpatient medical record on demographics, comorbidities, antibiotic use, healthcare exposures, invasive procedures, travel, animal contact, and food consumption. Participants with ESCrE colonization (cases) were compared to noncolonized participants (controls) using bivariable and multivariable analyses to identify risk factors for ESCrE colonization. Results: Enrollment occurred from January 15, 2020, to September 4, 2020, and 469 participants were enrolled. The median age was 42 years (IQR, 31–58) and 320 (68.2%) were female. The median time from hospital admission to date of sampling was 5 days (IQR, 3–12). There were 179 cases and 290 controls (ie, 38.2% of participants were ESCrE colonized). Independent risk factors for ESCrE colonization were a greater number of days on antibiotic, recent healthcare exposure, and tending swine prior to hospitalization. (Table). Conclusions: ESCrE colonization among hospitalized patients was common and was associated with several exposures. Our results suggest prior healthcare exposure may be important in driving ESCrE. The strong link to recent antibiotic use highlights the potential role of antibiotic stewardship interventions for prevention. The association with tending swine suggests that animal husbandry practices may play a role in community exposures, resulting in colonization detected at the time of hospital admission. These findings will help to inform future studies assessing strategies to curb further emergence of hospital ESCrE in LMICs.
Disclosures: None
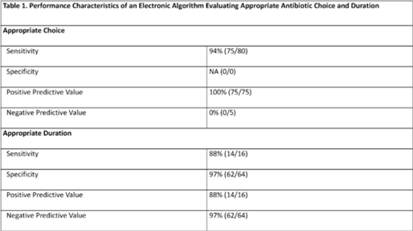
Background: Community-acquired pneumonia (CAP) is a common indication for antibiotic use in hospitalized children and is a key target for pediatric antimicrobial stewardship programs (ASPs). Building upon prior work, we developed and refined an electronic algorithm to identify children hospitalized with CAP and to evaluate the appropriateness of initial antibiotic choice and duration. Methods: We performed a cross-sectional study including children 6 months to 17 years hospitalized for CAP between January 1, 2019, and October 31, 2022, at a tertiary-care children’s hospital. CAP was defined electronically as an International Classification of Disease, Tenth Revision (ICD-10) code for pneumonia, a chest radiograph or chest computed tomography scan (CT) performed within 48 hours of admission, and systemic antibiotics administered within the first 48 hours of hospitalization and continued for at least 2 days. We applied the following exclusion criteria: patients transferred from another healthcare setting, those who died within 48 hours of hospitalization, children with complex chronic conditions, and those with intensive care unit stays >48 hours. Criteria for appropriate antibiotic choice and duration were defined based on established guidelines. Two physicians performed independent medical record reviews of 80 randomly selected patients (10% sample) to evaluate the performance of the electronic algorithm in (1) identifying patients treated for clinician-diagnosed CAP and (2) classifying antibiotic choice and duration as appropriate. A third physician resolved discrepancies. The electronic algorithm was compared to this medical record review, which served as the reference standard. Results: Of 80 children identified by the electronic algorithm, 79 (99%) were diagnosed with CAP based on medical record review. Antibiotic use was classified as the appropriate choice in 75 (94%) of 80 cases, and appropriate duration in 16 (20%) of 80 cases. The sensitivity of the electronic algorithm for identifying appropriate initial antibiotic choice was 94%; specificity could not be calculated because no events of inappropriate antibiotic choice were identified based on chart review. The sensitivity and specificity for determining appropriate duration were 88% and 97%, respectively (Table 1).
Conclusions: The electronic algorithm accurately identified children hospitalized with CAP and demonstrated acceptable performance for identifying appropriate antibiotic choice and duration. Use of this electronic algorithm may improve the efficiency of stewardship activities and could facilitate alignment with updated accreditation standards. Future studies validating this algorithm at other centers are needed.
Disclosures: None


