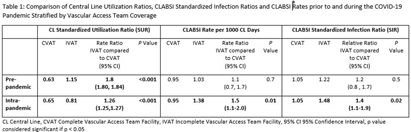
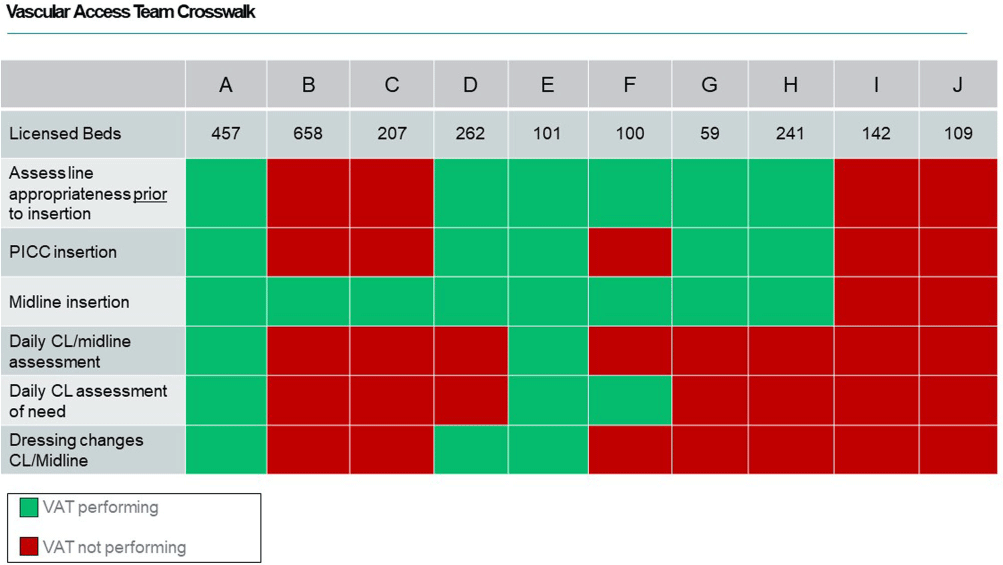
Background: During the COVID-19 pandemic, rates of central line bloodstream infections (CLABSI) increased nationally. Studies pre-pandemic showed improved CLABSI rates with implementation of a standardized vascular access team (VAT).[PL1] [PL2] [mi3] Varying VAT resources and coverage existed in our 10 acute care facilities (ACF) prior to and during the pandemic. VAT scope also varied in 1) process for line selection during initial placement, 2) ability to place a peripherally inserted central catheter (PICC), midline or ultrasound-guided peripheral IV in patients with difficult vascular access, 3) ownership of daily assessment of central line (CL) necessity, and 4) routine CL dressing changes. We aimed to define and implement the ideal VAT structure and evaluate the impact on CLABSI standardized infection ratios (SIR) and rates prior to and during the pandemic. Methods: A multidisciplinary workgroup including representatives from nursing, infection prevention, and vascular access was formed to understand the current state of VAT responsibilities across all ACFs. The group identified key responsibilities a VAT should conduct to aid in CLABSI prevention. Complete VAT coverage[mi4] was defined as the ability to conduct the identified responsibilities daily. We compared the SIR and CLABSI rates between hospitals who had complete VAT (CVAT) coverage to hospitals with incomplete VAT (IVAT) coverage. Given this work occurred during the pandemic, we further stratified our analysis based on a time frame prior to the pandemic (1/2015 – 12/2019) and intra-pandemic (1/2020 - 12/2022). Results: The multidisciplinary team identified 6 key components of complete VAT coverage: Assessment for appropriate line selection prior to insertion, ability to insert PICC and midlines, daily CL and midline care and maintenance assessments, daily assessment of necessity for CL, and weekly dressing changes for CL and midlines[NA5] . A cross walk of VAT scope (Figure 1) was performed in October 2022 which revealed two facilities (A and E) which met CVAT criteria. Pre-pandemic, while IVAT CLABSI rates and SIR were higher than in CVAT units, the difference was not statistically significant. During the pandemic, however, CLABSI rates and SIR were 40-50% higher in IVAT compared to CVAT facilities (Incident Rate Ratio 1.5, 95% CI 1.1-2.0 and SIR Relative Ratio 1.4, 95% CI1.1-1.9 respectively) (Table 1). Conclusions: CLABSI rates were lower in facilities with complete VAT coverage prior to and during the COVID-19 pandemic suggesting a highly functioning VAT can aid in preventing CLABSIs, especially when a healthcare system is stressed and resources are limited.
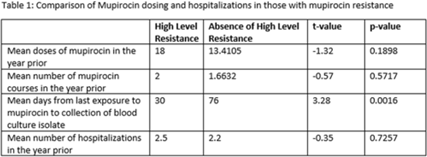
Methicillin-resistant Staphylococcus aureus (MRSA) is a common etiology of hospital-acquired infections (HAIs). One strategy to reduce HAIs due to MRSA involves a multistep decolonization process. This often involves nasal application of mupirocin 2% ointment. In our institution, when individuals meet criteria for decolonization, we recommend 5 days of treatment given twice daily. High levels of mupirocin resistance have been reported in some hospital systems, with >80% of tested isolates being resistant. To better understand our resistance levels, we selected 238 MRSA isolates from blood cultures to be tested for mupirocin resistance to correlate the presence of resistance and use of mupirocin for decolonization. We choose to assess MRSA blood isolates rather than nasal swabs given that we aim to prevent invasive MRSA infections, including blood stream infections, with decolonization. The blood cultures were collected from 11 acute-care facilities within our system from March 2021 through June 2022. High-level resistance was defined as an MIC >1,024 μg/mL according to Clinical and Laboratory Standards Institute guidelines. Of those, 7.14% showed high level resistance, and 76.47% occurred in those who were exposed to mupirocin and 23.53% occurred in those without mupirocin exposure (P = .0094). On average, those with high-level resistance had had more recent exposure to mupirocin compared to those without resistance, which was statistically significant. Also, those with high resistance, on average, received more doses of mupirocin, although this was not statistically significant. Conclusions: More recent and higher number of doses of mupirocin were associated with the development of resistance, which is consistent with what we know from pharmacodynamics of antibiotic resistance with other agents. These findings may be particularly important for those patients who have frequent hospitalizations and often require decolonization. Understanding baseline mupirocin resistance levels in an institution can assist with determining decolonization strategies.
Disclosures: None

