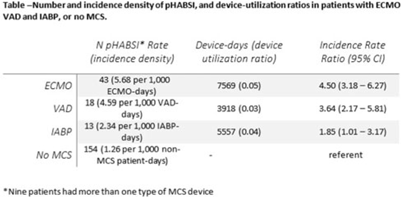
Background: Patients requiring mechanical circulatory support (MCS) during episodes of cardiogenic shock are at risk for hospital-acquired bloodstream infection (HABSI). Clinically MCS devices include extracorporeal membrane oxygenation (ECMO) devices, durable and temporary left ventricular-assist devices (VADs), and intra-aortic balloon pumps (IABPs). However, the MCS exclusion to the NHSN central-line–associated bloodstream infection (CLABSI) surveillance rules in 2018 did not include IABP as a qualifying device. We have described utilization and incidence of primary HABSI (pHABSI) in our patients requiring MCS. Methods: The setting for this study was 9 cardiothoracic and heart failure intensive care units with 131 total beds at the Cleveland Clinic Main Campus. Surveillance for HABSI to include determination of CLABSI was performed prospectively. MCS-associated pHABSI were patients who had ECMO, LVAD, or IABP present for >2 calendar days with device in place on the date of infection or removed the day before. A patient with 2 device types at time of infection was counted as a pHABSI for both groups. Patient, device, and MCS days were extracted from an electronic database. Non-MCS patient days were calculated as the difference between total patient days and total MCS days. The incidence of ECMO-, VAD-, and IABP-associated pHABSI were compared to each other and to non–MCS-associated pHABSI using OpenEpi version 3.01 software. Results: Surveillance results are shown in Table 1. During the observation period, there were 221 pHABSIs and 139,013 patient days. Moreover, 67 pHABSIs were associated with an MCS device over 17,044 total MCS days: 43 ECMO days, 18 VAD days, and 13 IABP days. Also, 9 patients had >1 type of eligible device and 7 (39%) of the IABP-associated pHABSIs were CLABSIs.
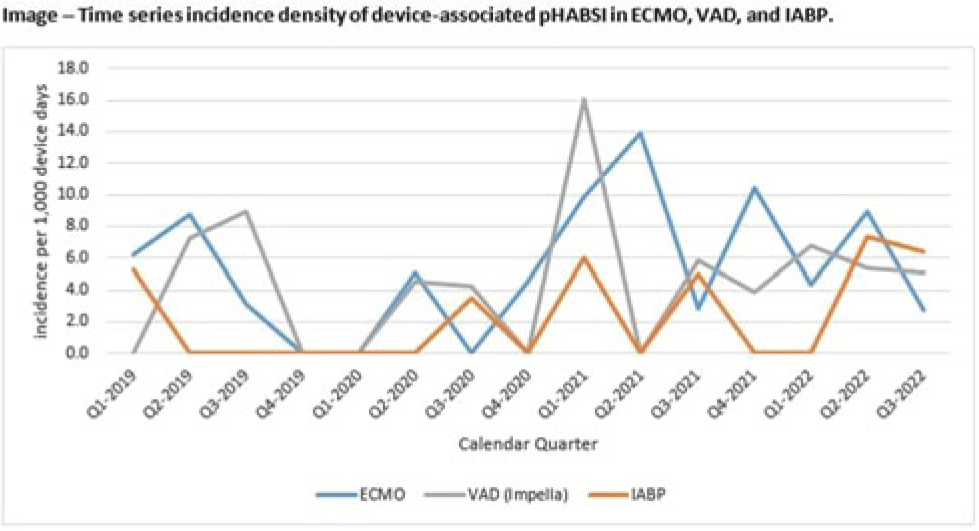
The cumulative incidences of pHABSI associated with ECMO, VAD, and IABP were 5.68, 4.59, and 2.34 per 1,000 MCS days, respectively. The incidence of IABP pHABSI was not significantly different from VAD pHABSI (P = .06), but it was different from ECMO pHABSI (P < .01). The pHABSI rate for non-MCS days was 1.26 per 1,000 patient days. Conclusions: In our patients requiring MCS, the risk of pHABSI associated with IABP was significantly greater than in patients without MCS and was similar to patients with VAD. MCS of all types should be considered a risk for HABSI in patients with cardiogenic shock beyond the presence of a central line. Protocols to further prevent HABSI morbidity in IABP patients are needed.
Disclosure: None
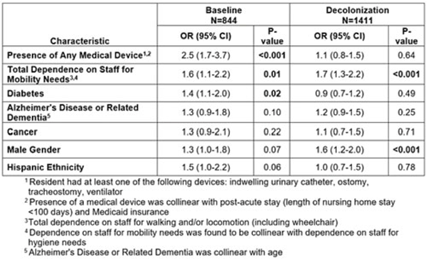
Background: A regional decolonization intervention (SHIELD-OC) involving universal chlorhexidine for routine bathing and 5 days of twice-daily nasal iodophor every other week in nursing homes (NHs) recently demonstrated marked reductions in multidrug-resistant organisms, all-cause hospitalizations, and infection-related hospitalizations in Orange County, California. Specific to methicillin-resistant Staphylococcus aureus (MRSA), NH prevalence (nares, skin, or perirectal) decreased from 43% to 29%. Methods: We conducted a retrospective cohort study evaluating the impact of decolonization on factors associated with MRSA carriage. The cohort included residents from 18 SHIELD-OC NHs who were sampled for MRSA using nares, axilla, groin, and perirectal cultures. A point-prevalence survey was conducted in 2016–2017 (before decolonization, 50 randomly sampled residents per NH) and in 2018–2019 (decolonization, all residents sampled). Resident characteristics were obtained from their most proximal admission, quarterly, and/or discharge assessment using data mandated for NH reporting (CMS minimum data set), and included demographics, medical devices, comorbidities (including Alzheimer’s disease and related dementias or ADRD), and mobility and hygiene needs. We used generalized-linear mixed models stratified by decolonization and clustered by NH to identify differences in factors associated with MRSA carriage. Results: Of the 2,351NH residents, 2,255 (96%) had characteristics available in the CMS data set. Of the 2,255 residents included, 774 (34%) were MRSA carriers. Before decolonization, medical devices (OR, 2.5), limited mobility (OR, 1.6), and diabetes (OR, 1.4) were significantly associated with MRSA carriage in an adjusted model (Table). During decolonization, these effects were mitigated (medical device OR, 2.5–1.1; diabetes OR, 1.4–0.9) and were no longer significantly associated with MRSA carriage. Male sex appeared to have more of an effect in the decolonization phase (OR, 1.3–1.6), but limited mobility remained stable (OR, 1.6–1.7). Several variables were collinear. Presence of a medical device was collinear with postacute stays (<100 days) and Medicaid insurance. Limited mobility was associated with limited ability for hygienic self-care. ADRD was collinear with age. Final adjusted models accounted for medical devices, limited mobility, diabetes, ADRD, cancer, sex, and ethnicity. Conclusions: In a large interventional cohort of 18 NHs, factors associated with MRSA carriage changed after adoption of universal decolonization. Specifically, the increased risk of MRSA associated with medical devices and diabetes were substantially mitigated by decolonization, suggesting that these risks are modifiable. These long-term care findings are consistent with clinical trials showing reductions in MRSA carriage after implementing chlorhexidine bathing in ICUs and in non-ICU patients with devices. The ability of decolonization to attenuate the risk of MRSA carriage among diabetics or other potential high-risk groups deserves further study.
Disclosures: None

