Refine listing
Actions for selected content:
141953 results in Open Access
Motivation to Motivate: Pilot of motivational interview training in a tertiary university hospital
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S181
-
- Article
-
- You have access
- Open access
- Export citation
Comparison of Staging Methods for Treatment-Resistant Depression: Chart Review
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S255-S256
-
- Article
-
- You have access
- Open access
- Export citation
Late-onset mania as a manifestation of neurosyphilis: A Case Report
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S497
-
- Article
-
- You have access
- Open access
- Export citation
Long-Term Trends in Psychiatric Day Hospitalization: A Retrospective Study in Algarve, Portugal
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S718
-
- Article
-
- You have access
- Open access
- Export citation
Is body image misperception associated with sociodemographic factors and life habits? a cross-sectional study 1399 Tunisian school-adolescents
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S469
-
- Article
-
- You have access
- Open access
- Export citation
Navigating Information Technologies in Everyday Psychiatry Practice: A Guide for Early Career Psychiatrists
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S37
-
- Article
-
- You have access
- Open access
- Export citation
Elevated herpesvirus antibody levels linked to schizophrenia and bipolar disorder
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S47
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
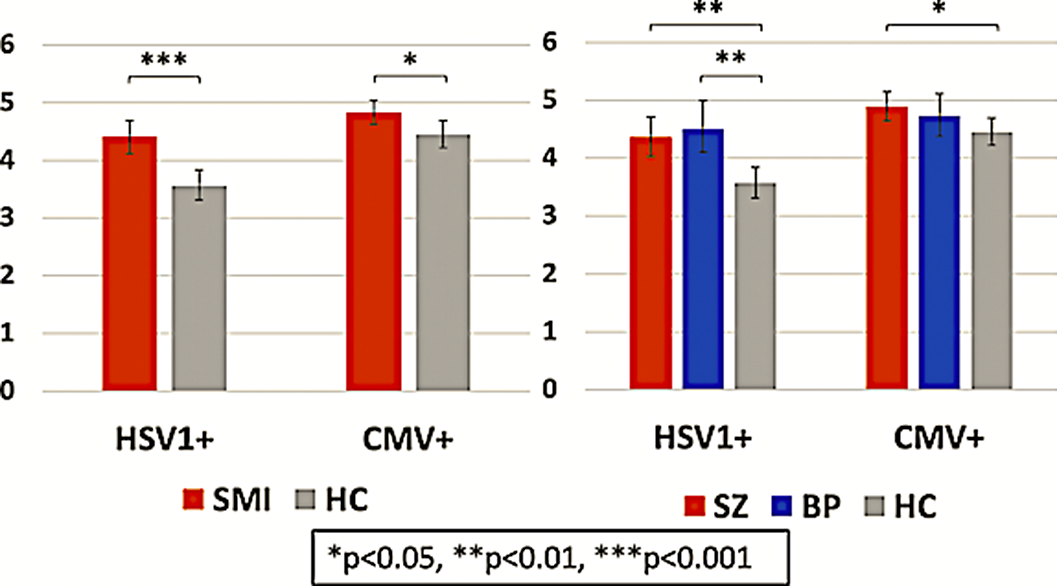
Previous research has implicated herpes simplex virus 1 (HSV1) and cytomegalovirus (CMV) in severe mental illness (SMI) with conflicting results. Both pathogens have high universal seroprevalence, are neurotropic and after the primary infection typically establish a persistent latent infection with periodic reactivations. Increased immunoglobin G (IgG) concentrations are considered to be attributable to an increased infection severity with more frequent reactivations or host immune system alterations.
ObjectivesWe assessed the HSV1 and CMV IgG concentrations in previously infected (seropositive) patients with SMI and healthy controls (HC). We hypothesized that seropositive patients would show higher IgG concentrations than seropositive HC.
MethodsWe included 765 patients, 515 with schizophrenia (SZ) and 250 with bipolar disorder (BP), and 541 HC. HSV1 and CMV IgG seropositivity and concentrations were measured with immunoassays. 355 patients, mean age 33 years, 45% females, and 238 HC, mean age 35 years, 44% females, were HSV1 seropositive (HSV1+) while 447 patients, mean age 33 years, 50% females, and 296 HC, mean age 34 years, 47% females, were CMV seropositive (CMV+). In our main analysis among seropositive participants, we investigated the main effect of patient/control status on HSV1 and CMV IgG concentrations.
ResultsThere were no significant differences in CMV or HSV1 seropositivity frequencies between patients with SZ, patients with BP and HC. Among seropositive participants, patients had higher HSV1 (p<0.001) and CMV (p=0.018) IgG concentrations than HC; stratifying by diagnosis, both patients with SZ (p=0.001) and patients with BP (p=0.001) had higher HSV1 IgG concentrations than HC, while patients with SZ, but not BP, had higher CMV (p=0.045) IgG concentrations than HC (Image). For HSV1, higher IgG concentrations were associated with higher general (p=0.017), negative (p=0.041) and positive (p=0.028) psychotic symptom scores.
Image:
 Conclusions
ConclusionsSeropositive patients with SMI showed higher HSV1 and CMV IgG concentrations than seropositive HC suggesting that patients suffer a more severe infection or exhibit an altered immune response when contracting the pathogens. For HSV1, higher IgG concentrations were linked to more psychotic symptoms.
Disclosure of InterestD. Andreou: None Declared, N. E. Steen: None Declared, K. N. Jørgensen: None Declared, T. Ueland: None Declared, L. Wortinger: None Declared, L. Mørch-Johnsen: None Declared, R. Yolken: None Declared, O. Andreassen Consultant of: Consultant to HealthLytix, Speakers bureau of: Received speaker’s honorarium from Lundbeck and Sunovion, I. Agartz Speakers bureau of: Received speaker’s honorarium from Lundbeck

Multifaceted Impact of the COVID-19 Pandemic and Lockdown on Physical and Mental Health: Insights from a Cross-Sectional Study
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S516
-
- Article
-
- You have access
- Open access
- Export citation
Updating the WHO Model Lists of Essential Medicines to promote global access to the most cost-effective and safe medicines for mental disorders
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S65-S66
-
- Article
-
- You have access
- Open access
- Export citation
Use of aripiprazole long-acting injectable release as a stabiliser. About a case
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S435-S436
-
- Article
-
- You have access
- Open access
- Export citation
Orthorexia Nervosa and exercise addiction in a sample of Tunisian athlete students
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S408
-
- Article
-
- You have access
- Open access
- Export citation
Prevalence of diabetes and insulin resistance in patients with diagnosis of schizophrenia or other psicotic disorders
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S741
-
- Article
-
- You have access
- Open access
- Export citation
Mental health in challenging times: Psychological perspectives for practitioners and society
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S6-S7
-
- Article
-
- You have access
- Open access
- Export citation
Depression: Biological Non-Pharmacological Interventions. A Review.
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S538-S539
-
- Article
-
- You have access
- Open access
- Export citation
How digital technology can contribute to timely and effective recognition and response to opioid overdose events
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S12-S13
-
- Article
-
- You have access
- Open access
- Export citation
The relation between autism and psychosis: overlapping and differing features
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S460-S461
-
- Article
-
- You have access
- Open access
- Export citation
Endometriosis and depressive symptoms: The role of quality of life in endometriosis, chronic illness-related shame, self-compassion, and psychological flexibility
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S230
-
- Article
-
- You have access
- Open access
- Export citation
Cardiovascular and metabolic issues in the treatment of schizophrenia: focus on the management of negative symptoms
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S18
-
- Article
-
- You have access
- Open access
- Export citation
Emotional non‐acceptance mediates the relationship between insecure attachment and specific psychopathology in women with eating disorders
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S558
-
- Article
-
- You have access
- Open access
- Export citation
The role of long-acting antipsychotics in illness relapse: an observational study
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S391-S392
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
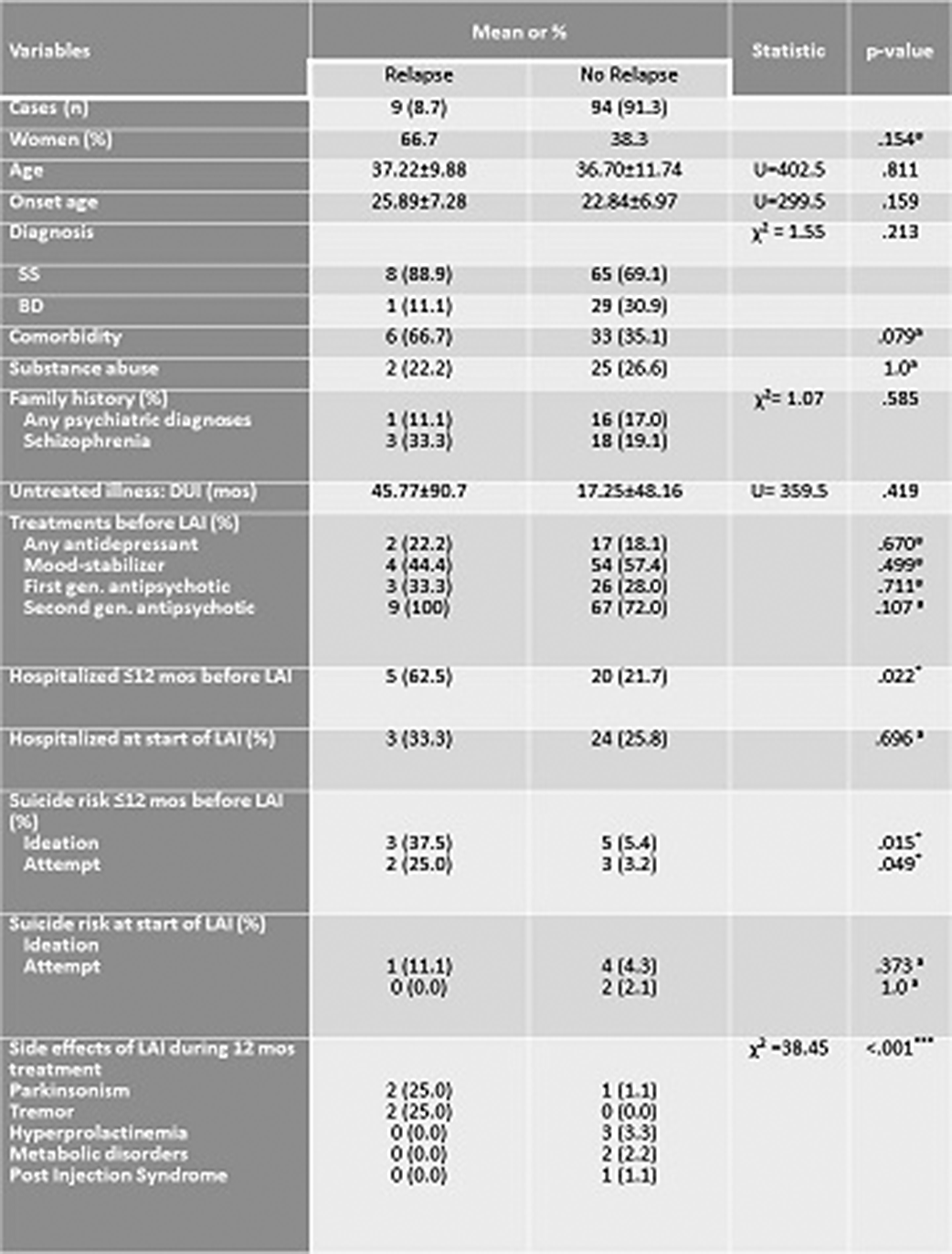
In patients affected by Schizophrenia and Bipolar Disorder disorders the use of antipsychotic drugs is essential in preventing the exacerbation of symptoms. The use of long-acting injectable (LAI) antipsychotics is considered an important treatment option. The aim of this study was to evaluate the incidence and predictors of relapse during antipsychotic treatment with LAIs in a sample of psychiatric outpatients up to a year after the start of long-acting therapy.
ObjectivesThe study included 103 adult patients admitted to the psychiatric unit of Sant’Andrea University Hospital in Rome.
MethodsWe evaluated duration of untreated illness, previous treatments, substance abuse, suicidal status, LAI dose, and use of other medicines for association with new episodes of illness or of symptomatic worsening as well as hospitalization, using bivariate and multivariate analyses.
ResultsSeventy-three patients were diagnosed with schizophrenia spectrum and 30 with bipolar disorders. Age at study entry averaged 36.7 years (SD= 11.55). 40.8% of patients were women. The mean age at onset were 23.11 (SD= 7.0). All the other information were reported in Table 1. On 103 patients undergoing with LAI treatment for a year only 9 (8.7%) patients had a relapse during the study period. The two groups differed according to the presence of hospitalization during the 12 months before the LAI treatment (p = .022), in particular patients with relapse were more hospitalized than patients with no relapse (62.5% vs. 21.7%). Moreover, group with relapse were more at risk of suicide during the 12 months before the LAI treatment than the other group, for both suicidal ideation (11.1% vs. 4.3%; p= .015) and attempt (25.0% vs. 3.2%; p= .049). Finally, the two groups differed according to the side effects reported during the year of LAI treatment (χ² =38.48; p< .001). Specifically, patients’ group with relapse reported more side effects caused by parkinsonism (25.0% vs. 1.1%) and tremor (25.0% vs. 0%). No differences were found for the other variables (See table 1).
Image:
 Conclusions
ConclusionsIn conclusion, our observations confirm the importance of LAI therapy in real word. However, our results indicate that these drugs might not prevent subsequent exacerbations for a proportion of individuals whose illness is stabilised on continuous antipsychotic treatment. Extra pyramidal symptoms in particular might have pathophysiological implications for relapse.
Disclosure of InterestNone Declared

