Refine listing
Actions for selected content:
141953 results in Open Access
Coping self-efficacy and personal growth in the situation of the COVID-19 threat
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S519-S520
-
- Article
-
- You have access
- Open access
- Export citation
Role of Different Forms and Intensities of Physical Activity in Prevention of Dementia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S200
-
- Article
-
- You have access
- Open access
- Export citation
Lithium nephropathy in Bipolar Disorder: a clinical challenge
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S429-S430
-
- Article
-
- You have access
- Open access
- Export citation
Suicide risk in patient with diabetes varies by the duration of diabetes: The Korea National Health and Nutrition Examination Survey
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S260-S261
-
- Article
-
- You have access
- Open access
- Export citation
Wellbeing after Brief Alcohol Interventions in Male Inpatients in a General Hospital in Singapore
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S414-S415
-
- Article
-
- You have access
- Open access
- Export citation
Exploring the Impact of 2023 Wildfires on Generalized Anxiety Disorder Symptoms among Residents in Alberta and Nova Scotia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S420
-
- Article
-
- You have access
- Open access
- Export citation
The preponderance of major depressive disorder among women of reproductive age and the clinical utility of sertraline
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S535-S536
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Major depressive disorder (MDD) is twice as common in women than men and is more frequently reported during their reproductive years (Shi et al. Front. Psychiatr 2021; 12 589687). MDD affects up to 12.7% of pregnant women and can significantly impact foetal and maternal health. Hence, clinical practice guidelines recommend focused screening and expedited management of MDD in women (Guo et al. Obstet. Gynecol 2018; 131(4) 671-679). Despite this, drug labelling or dosing recommendations rarely account for gender or physiological differences between sexes, even though sex steroid level variations can impact drug absorption, distribution, metabolism, and activity both pharmacokinetically and pharmacodynamically (Soldin et al. Clin Pharmacokinet. 2009; 48(3): 143–157). Sertraline, an SSRI approved for the treatment of MDD, is one of the safer agents which can be given to childbearing or breastfeeding women (Cuomo et al. Expert Opin Drug Saf 2018; 17(7) 719-725). However, studies on the efficacy of sertraline for the treatment of MDD among women of childbearing age are limited.
ObjectivesThis post-hoc pooled analysis evaluated the efficacy of sertraline in women with MDD, with a particular focus on women of reproductive age.
MethodsA pooled data analysis of 8 short-term clinical studies of sertraline in persons with MDD (comprising 1600 participants from North America and Europe, of whom 947 were females; with moderate to severe MDD [mean±SD baseline HAM-D17 score was 23.73±3.58 for sertraline and 23.37± 3.47 for placebo]; sertraline dose, 50-200 mg) was performed. HAM-D17 total score was used to assess the efficacy of sertraline compared with placebo. The study period was 8 weeks. An MMRM method was used to analyse changes over time and ANCOVA to evaluate the change from baseline at week 8 with LOCF employed to manage missing data.
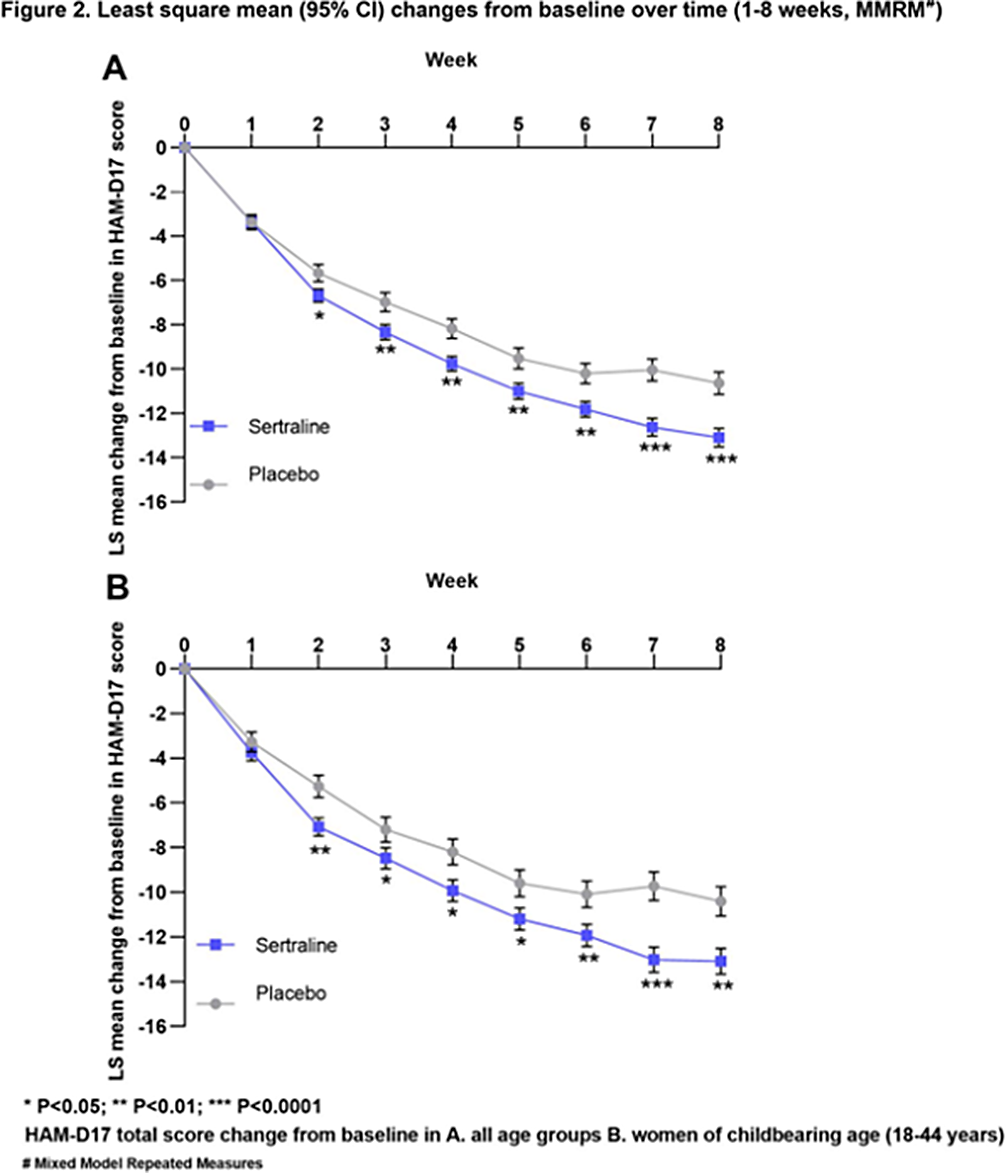
ResultsThe analysis set consisted of 947 women (sertraline, 612; placebo, 335). The change from baseline in HAM-D17 total score was significantly higher for sertraline than for placebo at the end of 8 weeks (LS mean difference, 95% CI: -1.81 [-3.01, -0.62], p=0.0029, Figure 1A). This change from baseline was statistically significant starting from week 2 and increased over time (Week 2-8; Figure 2A).
The analysis set for women of child-bearing age consisted of 572 participants aged 18-44 (sertraline, 359; placebo, 213) from 7 clinical studies. The change from baseline in HAM-D17 total score was significantly higher for sertraline than for placebo at the end of 8 weeks (LS mean difference, 95% CI: -2.08 [-3.52, -0.64], p=0.0047, Figure 1B). This change from baseline was statistically significant starting from week 2 (Figure 2B).
Image:
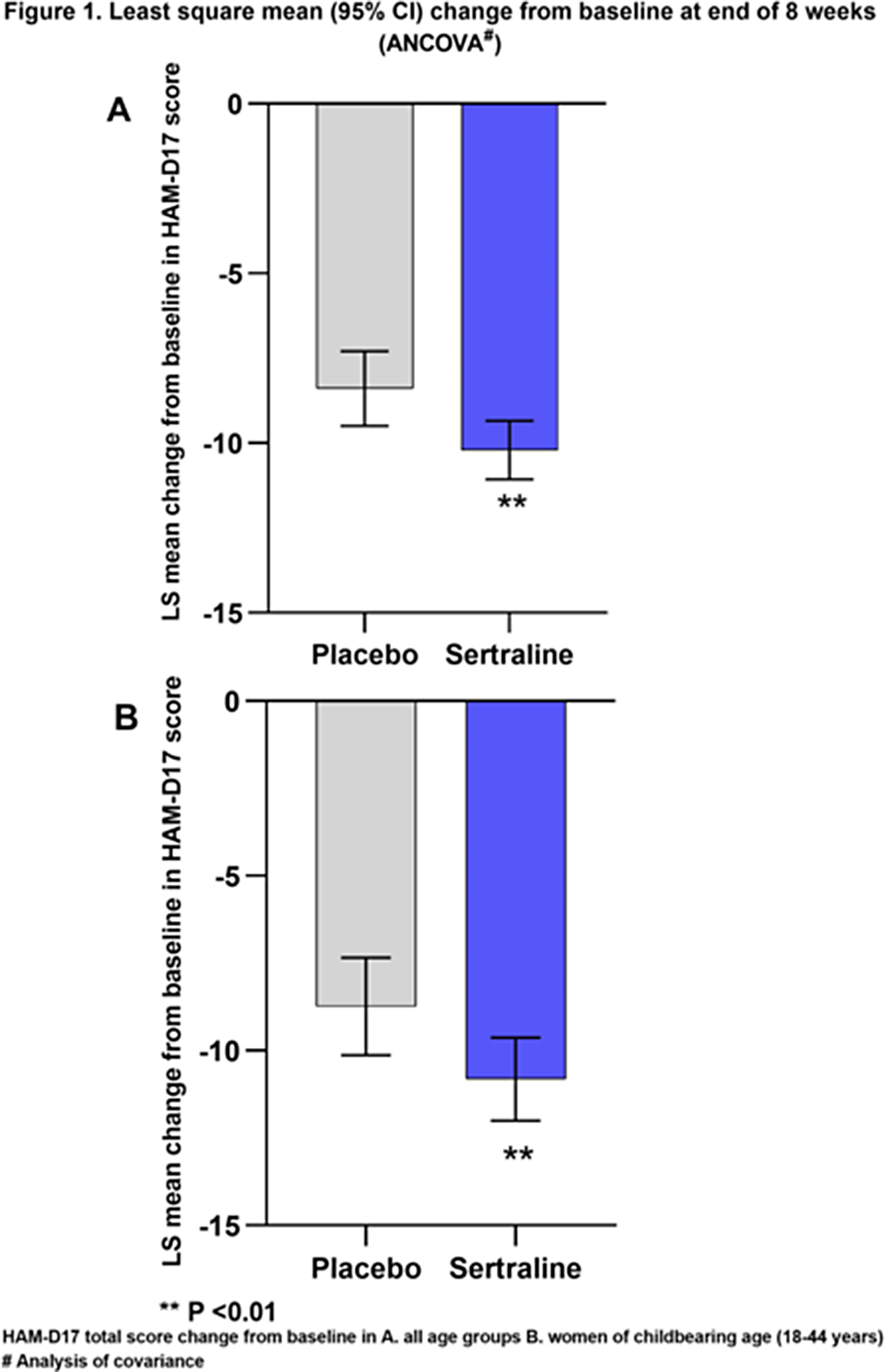
Image 2:
 Conclusions
ConclusionsSignificant improvement in HAM-D17 scores was observed in the analysis, suggesting that sertraline is efficacious in treating women with MDD, including those in the childbearing age.
Disclosure of InterestA. Fagiolini Grant / Research support from: Angelini, Boheringer Ingelheim, Janssen, Consultant of: Angelini, Biogen, Boheringer Ingelheim, Lundbeck, Janssen, Mylan, Neuraxpharm, Otsuka, Pfizer, Recordati, Rovi, Sanofi Aventis, Viatris, Speakers bureau of: Angelini, Apsen, Biogen, Boheringer Ingelheim, Glaxo Smith Kline, Lundbeck, Janssen, Mylan, Neuraxpharm, Otsuka, Pfizer, Recordati, Rovi, Sanofi Aventis, Viatris, Vifor, M. Mariano Consultant of: Johnson & Johnson, Otsuka Pharmaceutical Inc., Speakers bureau of: Viatris Pharmaceuticals, Inc. Otsuka (Philippines) Pharmaceutical, Inc. H. Lundbeck A/S, Johnson & Johnson Philippines, Inc., E. Biesheuvel Employee of: Viatris Inc. Netherlands, P. Purushottamahanti Employee of: Viatris Inc. India


The Effect of Depression on Smartphone Addiction: The Medicating Effects of Interpersonal Problem in Korean Adolescents
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S137-S138
-
- Article
-
- You have access
- Open access
- Export citation
Lithium withdrawal and relapse in bipolar disorder when kidney function deteriorates
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S427-S428
-
- Article
-
- You have access
- Open access
- Export citation
Clinical and cognitive factors associated to insight in first psychotic episodes
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S746
-
- Article
-
- You have access
- Open access
- Export citation
Preliminary results of “Choose Life!” - a county-wide programme for suicide prevention and mental health awareness
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S245
-
- Article
-
- You have access
- Open access
- Export citation
Insight into Illness Among Inpatients in a National Forensic Mental Health Service: A Dundrum Forensic Redevelopment Evaluation Study (D-FOREST)
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S154-S155
-
- Article
-
- You have access
- Open access
- Export citation
Women with borderline personality disorder and pathophilia: understanding causes of pandemic diffusion of transmissible diseases through samos syndrome
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S807-S808
-
- Article
-
- You have access
- Open access
- Export citation
Difficulties in assessing the medical fitness of workers with mood disorders : A study of 101 cases
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S430-S431
-
- Article
-
- You have access
- Open access
- Export citation
Psychiatrists’ Readiness for Digital Psychiatry in Pakistan: A Multicenter CrossSectional Study with Regression Analysis
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S548-S549
-
- Article
-
- You have access
- Open access
- Export citation
Clinical Benefits, efficacy and tolerability of slowly titrated vortioxetine oral drops solution
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S544-S545
-
- Article
-
- You have access
- Open access
- Export citation
Alzheimer’s and Parkinson’s disease drugs side effects
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S633-S634
-
- Article
-
- You have access
- Open access
- Export citation
Recovery in schizophrenia: conceptualization and factors implicated
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S14
-
- Article
-
- You have access
- Open access
- Export citation
Breath Gas Markers in Depression and Their Relationship with Brain Metabolism
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S537
-
- Article
-
- You have access
- Open access
- Export citation
Sleeping Problems or Emerging Psychosis? A Review of Emerging Literature
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S770-S771
-
- Article
-
- You have access
- Open access
- Export citation
