Refine listing
Actions for selected content:
141953 results in Open Access
Exploring the associations between involuntary treatment and gender in a portuguese acute psychiatric unit
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S309-S310
-
- Article
-
- You have access
- Open access
- Export citation
An educational program, «Women victims of domestic violence: Detection, clinic, help»: Working with the complexity of teaching and Interpreting practice through research
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S805
-
- Article
-
- You have access
- Open access
- Export citation
Kambó as a drug that can induce psychotic or manic symptoms. A case report
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S419
-
- Article
-
- You have access
- Open access
- Export citation
Perceived parental bonding and cortisol awakening response in people with eating disorders
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S65
-
- Article
-
- You have access
- Open access
- Export citation
A preliminary analysis of clinical characteristics of patient with alcohol use disorder and suicidal ideation
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S132-S133
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Suicidal behaviors are frequently observed among patients with substance use disorder, including suicidal ideation (SI) (1). Alcohol use disorder (AUD) is one of the most prevalent addictions and may be related to suicidal behaviors (2,3). However, the association between AUD and SI requires a deeper analysis which includes several clinical features observed among AUD patients.
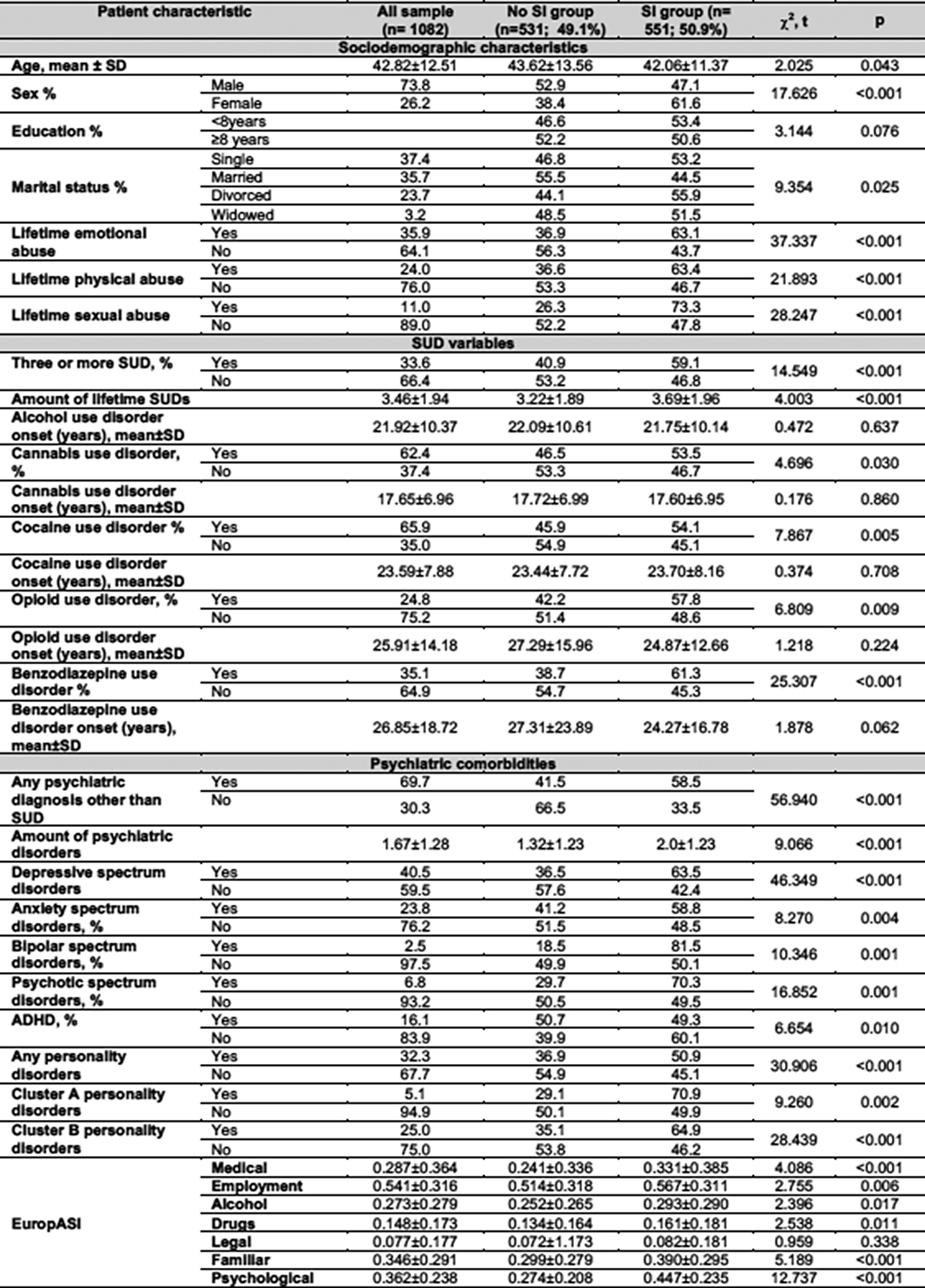
ObjectivesTo analyze the clinical characteristics and features associated with lifetime SI among patients who had AUD.
MethodsThis is a cross-sectional study performed in an outpatient center for addiction treatment in patients seeking for treatment who met the criteria for AUD between 01/01/2010 and 12/31/2021. Patients were evaluated with an ad-hoc questionnaire and the European Addiction Severity Index (EuropASI), SI was evaluated using the item for SI in EuropASI.
ResultsFrom a potential sample of n=3729 patients, only n=1082 (73.8% males; mean age 42.82±12.51) met inclusion criteria and had data for the current analysis. Lifetime SI was present in 50.9% of the AUD patients. Several clinical features were related to SI, including: sex differences, any type of lifetime abuse, polyconsumption, benzodiazepine use disorder, any psychiatric diagnosis aside from SUD, and higher addiction severity according to the EuropASI.
Image:
 Conclusions
ConclusionsSI among AUD patients is related to several clinical features which indicate a higher addiction severity, more polyconsumption, and a higher prevalence of psychiatric comorbidities. These findings may contribute to the understanding of suicidal behaviors in AUD patients but it is required further investigations, including longitudinal studies.
REFERENCES
1 Rodríguez-Cintas L, et al. Factors associated with lifetime suicidal ideation and suicide attempts in outpatients with substance use disorders. Psychiatry Res. 2018;262:440-445. doi:10.1016/j.psychres.2017.09.021
2. MacKillop J, et al. Hazardous drinking and alcohol use disorders. Nat Rev Dis Primers. 2022;8(1):80. doi:10.1038/s41572-022-00406-1
3.Darvishi N, et al. Alcohol-related risk of suicidal ideation, suicide attempt, and completed suicide: a meta-analysis [published correction appears in PLoS One. 2020;15(10):e0241874]. PLoS One. 2015;10(5):e0126870. doi:10.1371/journal.pone.0126870
Disclosure of InterestNone Declared

Medication choice and psychosis Hospital readmissions: A two-year comparative study
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S288
-
- Article
-
- You have access
- Open access
- Export citation
Non-compliance as ethical dilemma for kidney transplantation
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S577
-
- Article
-
- You have access
- Open access
- Export citation
Neuroinflammation in Recent Onset Mental Health Disorders – Developing Multi-level Signatures of Early-stage Depression and Psychosis in Young Adults
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S45-S47
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
An early and comprehensive neurobiological characterization of severe mental disorders could elucidate mechanistic pathways, aid the development of novel therapeutics, and therefore enable timely and targeted intervention in at-risk youth and young adults. Therefore, we present an unsupervised transdiagnostic machine learning approach to investigate shared and distinct patterns of early-stage depressive and psychotic disorders on multiple clinical and neurobiological levels.
ObjectivesTo derive multi-level neurobiological and clinical signatures of early-stage affective and psychotic disorders in adolescents and young adults.
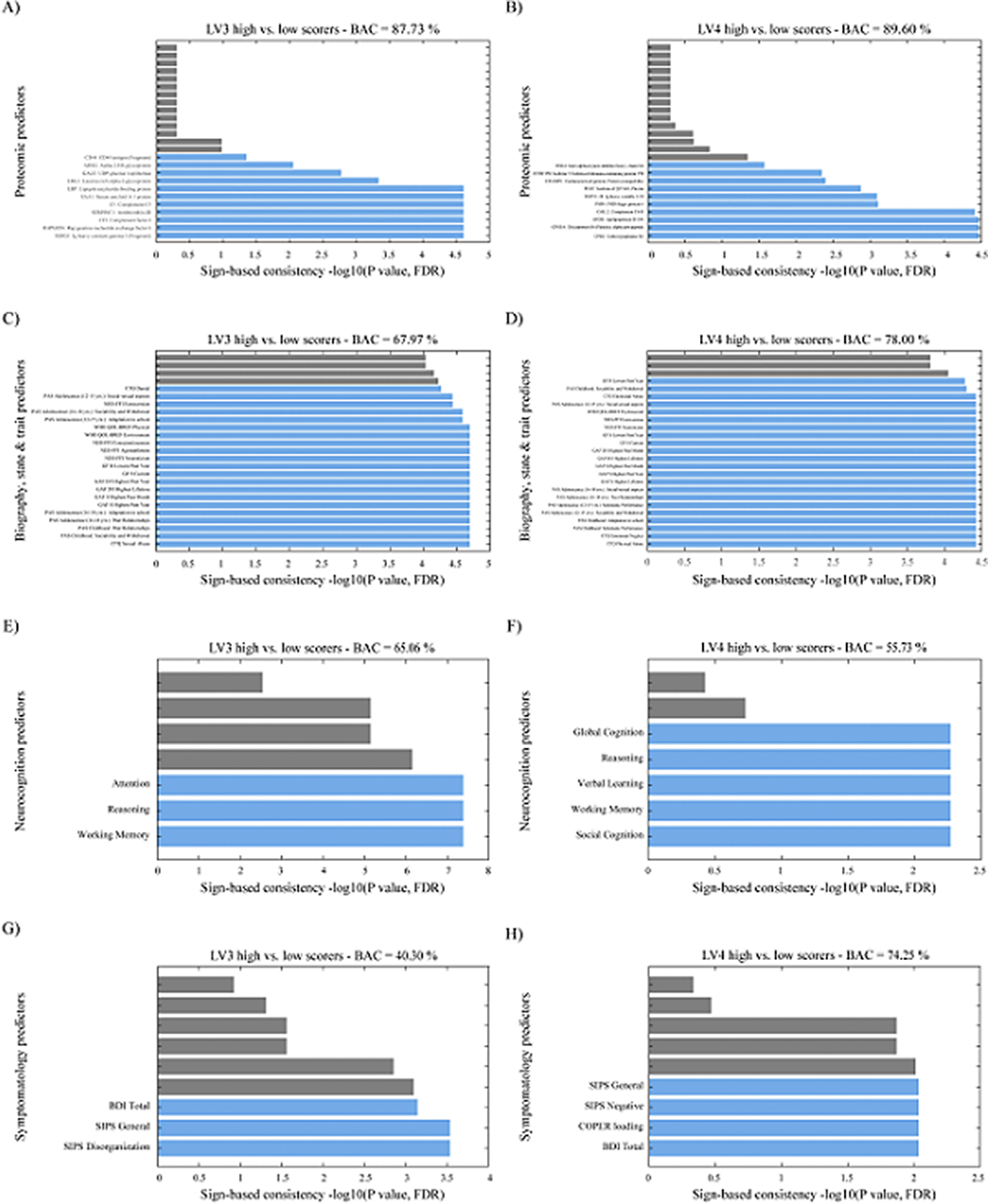
MethodsFrom the multicenter prospective European PRONIA cohort, we acquired data from 678 individuals (51% female) comprising young, minimally medicated in- and outpatients with clinical high-risk (CHR) states for psychosis, with recent-onset depression (ROD) or psychosis (ROP), and healthy control (HC) individuals. Within repeated nested cross-validation frameworks, we employed Sparse Partial Least Squares Analysis to detect associations between blood markers and grey matter volume (GMV), followed by support vector machine prediction of these signatures using biographical, clinical, neurocognitive, proteomic, and functional data.
ResultsOur results demonstrated a psychosis staging signature separating ROP from CHR individuals via GMV patterns in the cortico-thalamo-cerebellar circuitry with a blood marker set of elevated of IL-6, TNF-α and CRP (ρ = 0.272; P = 0.002). A depression signature separated ROD from HC individuals via altered GMV in the limbic system with a blood marker set of elevated IL-1ß, IL-2, IL-4, S100B and BDNF (ρ = 0.186; P = 0.021). Only the psychosis staging signature showed a distinct proteomic enrichment regarding innate immune response, abnormal neutrophil function, cellular senescence, and anti-inflammatory drugs (Balanced Accuracy (BAC) = 87.73%; Area Under the Curve (AUC) = 0.94). Childhood trauma differentially predicted psychosis and depression signatures, while past level of functioning, personality and quality of life was predictive of both signatures (BAC = 67.19-78.00%; AUC = 0.71-0.83).
Image:
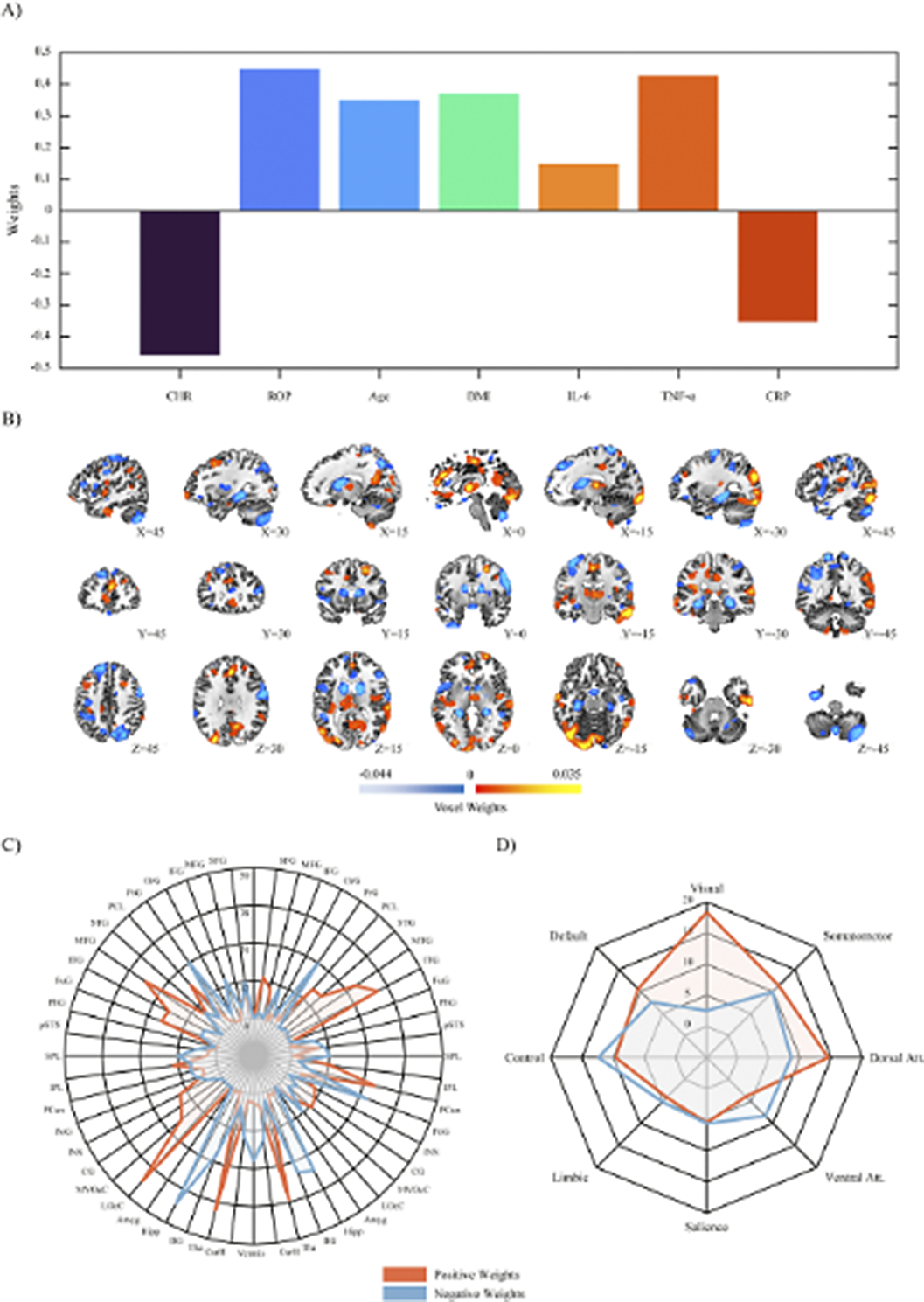
Image 2:
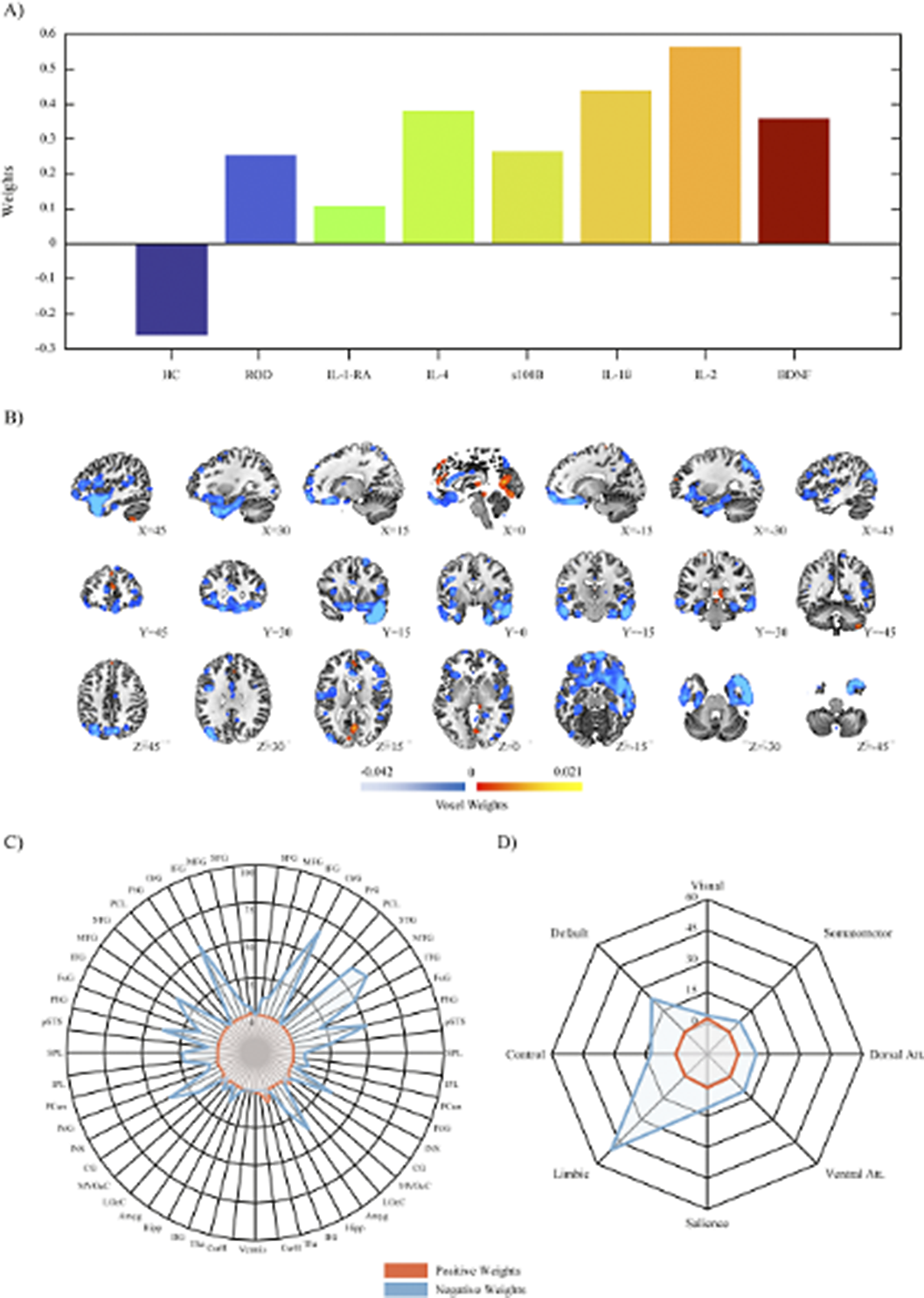
Image 3:
 Conclusions
ConclusionsPsychosis and depression exhibit distinct multi-level signatures evident in early disease stages. Enhanced insight into these signatures could help delineate individual trajectories and potentially new mechanisms for pharmacological treatment.
Disclosure of InterestNone Declared



“Neighbohod Vulnerability and Disability in First Episode of Psychosis”.
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S291-S292
-
- Article
-
- You have access
- Open access
- Export citation
The level of consciousness and mental reactions of children after acute brain injury (interdisciplinary rehabilitation)
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S713
-
- Article
-
- You have access
- Open access
- Export citation
Ethnic differences in pathways to obtain care, maintain care and engage to Early Intervention Service in Spain
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S165
-
- Article
-
- You have access
- Open access
- Export citation
Symptoms of anxiety and depression among osteoporotic women
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S486
-
- Article
-
- You have access
- Open access
- Export citation
Sodium oxybate – new views on an old candidate This presentation will outline the outcome of a clinical development program, including a Phase 3 study, on sodium oxybate in the treatment of alcohol dependence
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S6
-
- Article
-
- You have access
- Open access
- Export citation
When sleep disorders in patients with bipolar disorder indicate a risk of suicidal behavior
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S786
-
- Article
-
- You have access
- Open access
- Export citation
Predictors of Adherence and Response to Exercise Interventions in Schizophrenia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S11
-
- Article
-
- You have access
- Open access
- Export citation
From guided self-help to comprehensive ED treatment
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S308
-
- Article
-
- You have access
- Open access
- Export citation
Changing Tactics? Optimizing ECT in difficult-to-treat depression (ChaT): study protocol
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S123-S124
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Electroconvulsive therapy (ECT) is an evidence-based treatment for difficult-to-treat depression, in which an electrical stimulus is applied via right unilateral (RUL) (Fig 1) or bitemporal (BT) electrodes (Fig 2). Current guidelines recommend to start ECT with RUL placement, except for cases where rapid response is needed. BT ECT has the reputation of exerting a stronger and faster antidepressive effect, but is associated with more pronounced cognitive side effects, as compared to RUL ECT. Recent studies, however, suggest comparable outcomes. In patients responding to ECT, most of the improvement in depressive symptom severity is witnessed early in the treatment course. In case of non-response, it is common practice to switch from RUL to BT electrode placement, although scientific evidence is lacking. As an answer to this research gap, the ChaT-trial was designed: a randomized controlled trial (RCT) to address which treatment strategy (either continue RUL ECT or switch to BT ECT) speeds up recovery with the least impact on cognitive function, in case of early non-response after 4 ECT sessions.
Objectives1) To compare the antidepressant efficacy and cognitive effects of continuing RUL ECT vs switching to BT ECT.
2) To assess group and subject-specific trajectories of depressive symptom severity and neurocognitive performance during the acute ECT course and up to 3 months post-treatment.
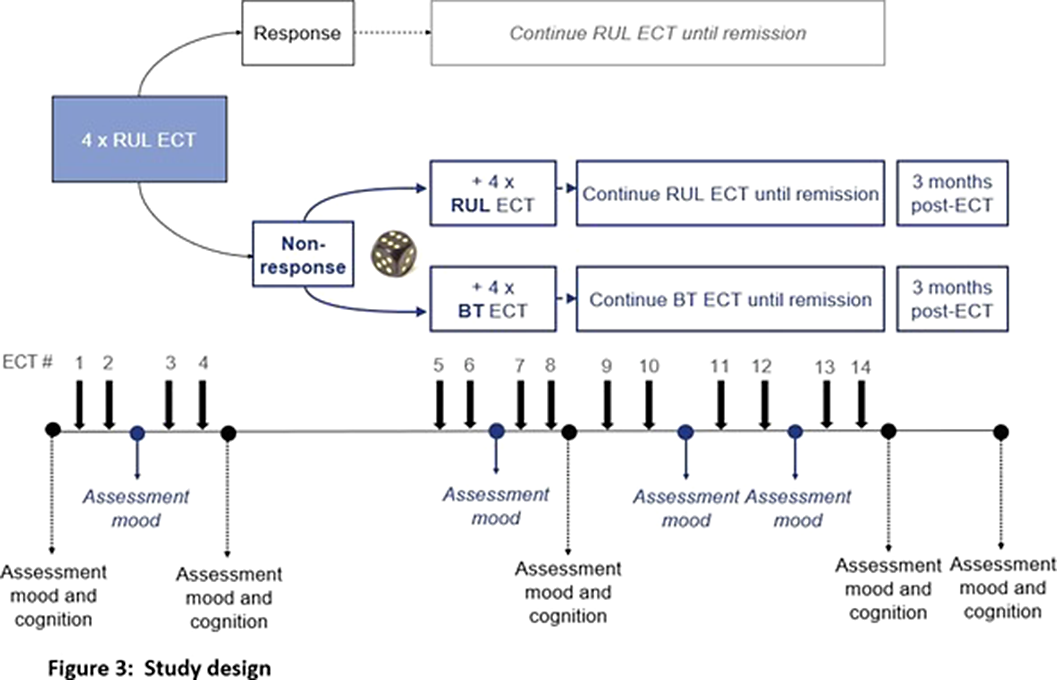
MethodsThis multi-center double-blind RCT includes adult patients with a uni- or bipolar depression. In case of non-response (<50% decrease of IDS-CR score (Inventory of Depressive Symptomatology-Clinician Rated)) after 4 sessions of brief-pulse high-dose RUL ECT, patients are randomized to either continue RUL ECT, or switch to brief-pulse moderate dose BT ECT until remission. Depressive symptoms are assessed by IDS-CR, Psychotic Depression Assessment Scale (PDAS) and CORE assessment of psychomotor change. An extensive neuropsychological test battery is used to assess different domains of cognitive functioning, e.g., autobiographical memory using the Colombia University- Autobiographical Memory Interview Short- Form (CU-AMI-SF)(Fig 3).
ResultsOur hypotheses are: (1) continuing RUL ECT is non-inferior to switching to BT ECT in terms of depressive symptom severity, and (2) continuing RUL ECT is superior to switching to BT ECT in terms of cognitive side effects.
Image:
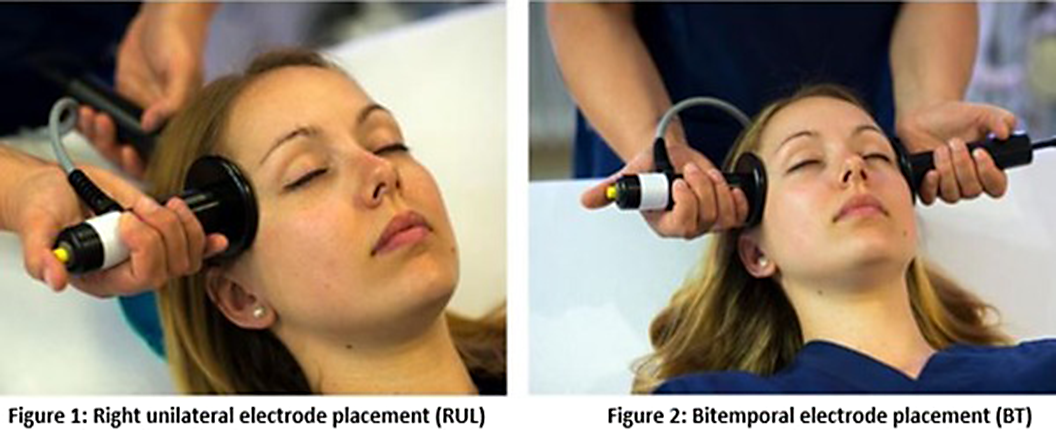
Image 2:
 Conclusions
ConclusionsThe ChaT-trial is the first RCT comparing antidepressant efficacy and cognitive effects of continuing RUL ECT with switching to BT ECT in case of early non-response during an acute ECT-course. The results may optimize clinical decision making, speeding up recovery, while minimizing cognitive side effects.
Disclosure of InterestNone Declared


Adaptation and analysis of the Hungarian version of the Snaith-Hamilton Pleasure Scale
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S536-S537
-
- Article
-
- You have access
- Open access
- Export citation
Platelet enzymatic activities in patients with late-onset schizophrenia spectrum disorders
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S643
-
- Article
-
- You have access
- Open access
- Export citation
Adverse childhood experiences and 8-year trajectories of depressive symptoms in community-dwelling older adults: Results from the English Longitudinal Study of Ageing
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S333-S334
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
The negative impact of adverse childhood experiences (ACEs) on mental health has been well documented. While most of the evidence comes from samples of adolescents and young adults, few studies have investigated whether ACEs contribute to poorer mental health among older adults. In particular, depressive symptoms are common in old age, and they display heterogeneous patterns of development across individuals. Therefore, it is important to examine if ACEs are predictive of distinct trajectories of depressive symptoms among older adults.
ObjectivesUsing longitudinal data from the English Longitudinal Study of Ageing (ELSA), we aimed to examine if ACEs could differentiate between distinct trajectories of depressive symptoms over eight years in community-dwelling older adults.
MethodsParticipants from ELSA aged 60 or above who reported no psychiatric diagnoses and completed the items of ACEs at baseline (wave 3) were included in the current study. Nine items of ACEs were subject to a principal component analysis to identify the underlying subtypes. Data of depressive symptoms from waves 3 to 7 (2-year apart), assessed with the 8-item Centre for Epidemiological Studies Depression Scale, were extracted for modelling the distinct trajectories using latent class growth analysis. The trajectories were predicted by subtypes of ACEs using multinomial logistic regression, adjusting for childhood socioeconomic status, sex, age and ethnicity.
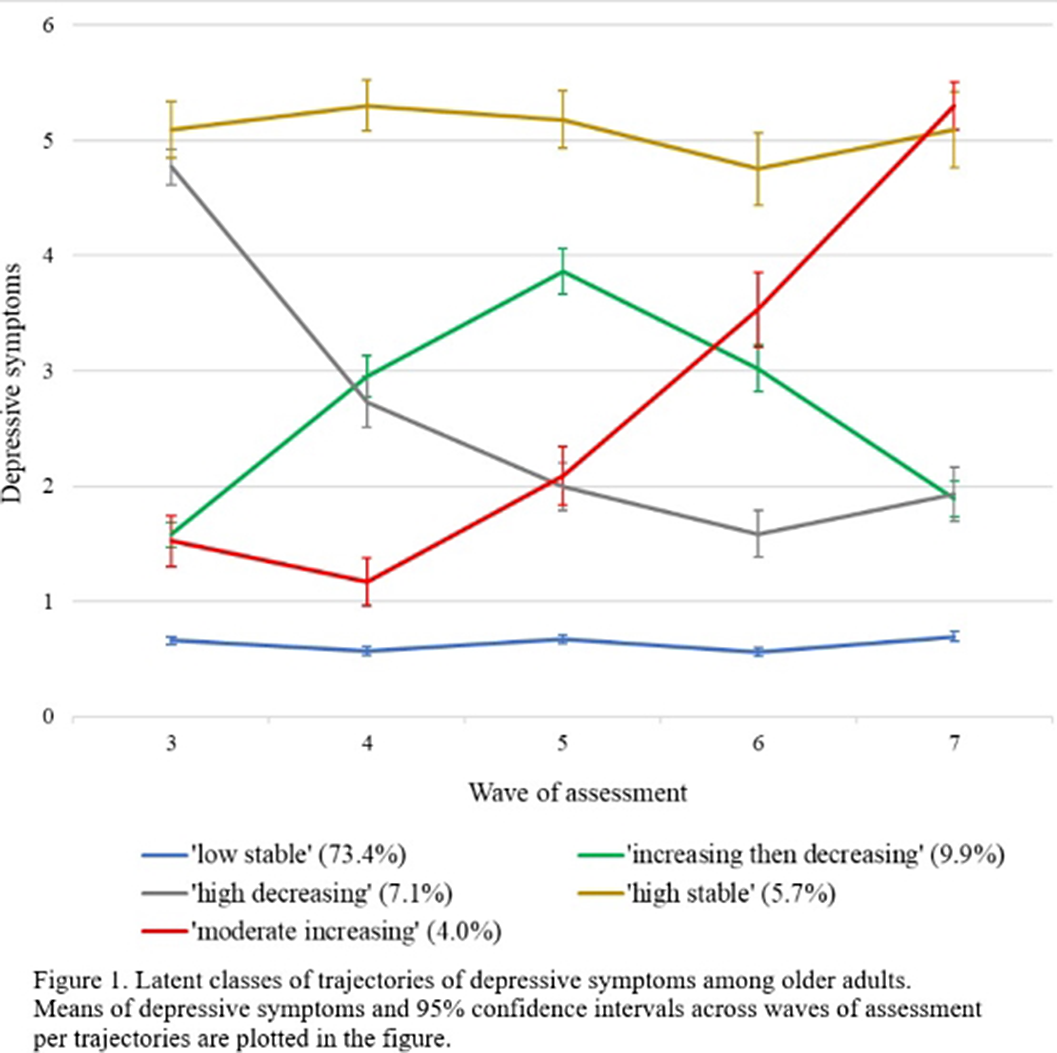
ResultsThe final sample consisted of 4057 participants (54.4% female, mean age= 71.34 (SD= 8.14)). We identified five trajectories of depressive symptoms (Figure 1): ‘low stable’ (73.4%), ‘increasing then decreasing’ (9.9%), ‘high decreasing’ (7.1%), ‘high stable’ (5.7%) and ‘moderate increasing’ (4.0%). Four subtypes of ACEs (i.e., sexual abuse, separation from natural parents, family dysfunction and physical assault) were evident. Compared to the ‘low stable’ group, higher levels of family dysfunction were reported in the ‘increasing then decreasing’ (aOR = 1.35, 95% CI [1.10 - 1.66], p = .012), ‘high stable’ (aOR = 1.59, 95% CI [1.30 - 1.96], p < .001) and ‘moderate increasing’ (aOR = 1.55, 95% CI [1.18 - 2.04], p = .011) groups. The ‘high stable’ group also reported a higher level of separation from natural parents than the ‘low stable’ group (aOR = 1.34, 95% CI [1.04 - 1.72], p = .047). Sexual abuse and physical assault did not predict any group differences.
Image:
 Conclusions
ConclusionsDistinct trajectories of depressive symptoms among older adults were predicted by family dysfunction in childhood. Our findings suggested that the negative impact of ACEs on mental health may extend beyond adolescence and young adulthood into the old age.
Disclosure of InterestNone Declared

