Refine listing
Actions for selected content:
142351 results in Open Access
Perception of Violence by Psychiatric Nurses: Behind the scenes
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S594
-
- Article
-
- You have access
- Open access
- Export citation
SCHIZOPHRENIC DREAMS: A Brief Description of Sleep Disturbances in Schizophrenia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S774
-
- Article
-
- You have access
- Open access
- Export citation
Divergent risk of SARS-CoV-2 infection, severe COVID-19 and mortality across psychiatric disorders: analysis from electronic health records in Catalonia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S264-S265
-
- Article
-
- You have access
- Open access
- Export citation
Research of cognitive disorders and quality of life in patients, who are receiving methadone replacement maintenance therapy
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S134-S135
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Important goals of substitution therapy include: reducing the desire to use opioids - methadone enters the brain with a minimal euphoric effect, reduce the desire to use opioids, allowing to avoid the risk of overdose and control their addiction; prevention of withdrawal syndrome; improving the quality of life - can contribute to the restoration of patients, allowing them to return to a normal life, improve their social, professional and family situation; reducing the risk of transmission of infections HIV and hepatitis; reducing crime - control addiction can reduce related crime and to illicitly obtain opioids; psychosocial support helps patients develop coping strategies and increases their chances of long-term recovery.
The goal of substitution therapy is not to completely get rid of addiction, but it can help stabilize the patient’s life and facilitate the recovery process.
ObjectivesMany patients receiving MT also have mental disorders such as cognitive decline, depression, anxiety, PTSD, or even bipolar disorder. These conditions can greatly affect the course and results of treatment.They may also have problems with employment, housing, family conflicts, and legal issues.
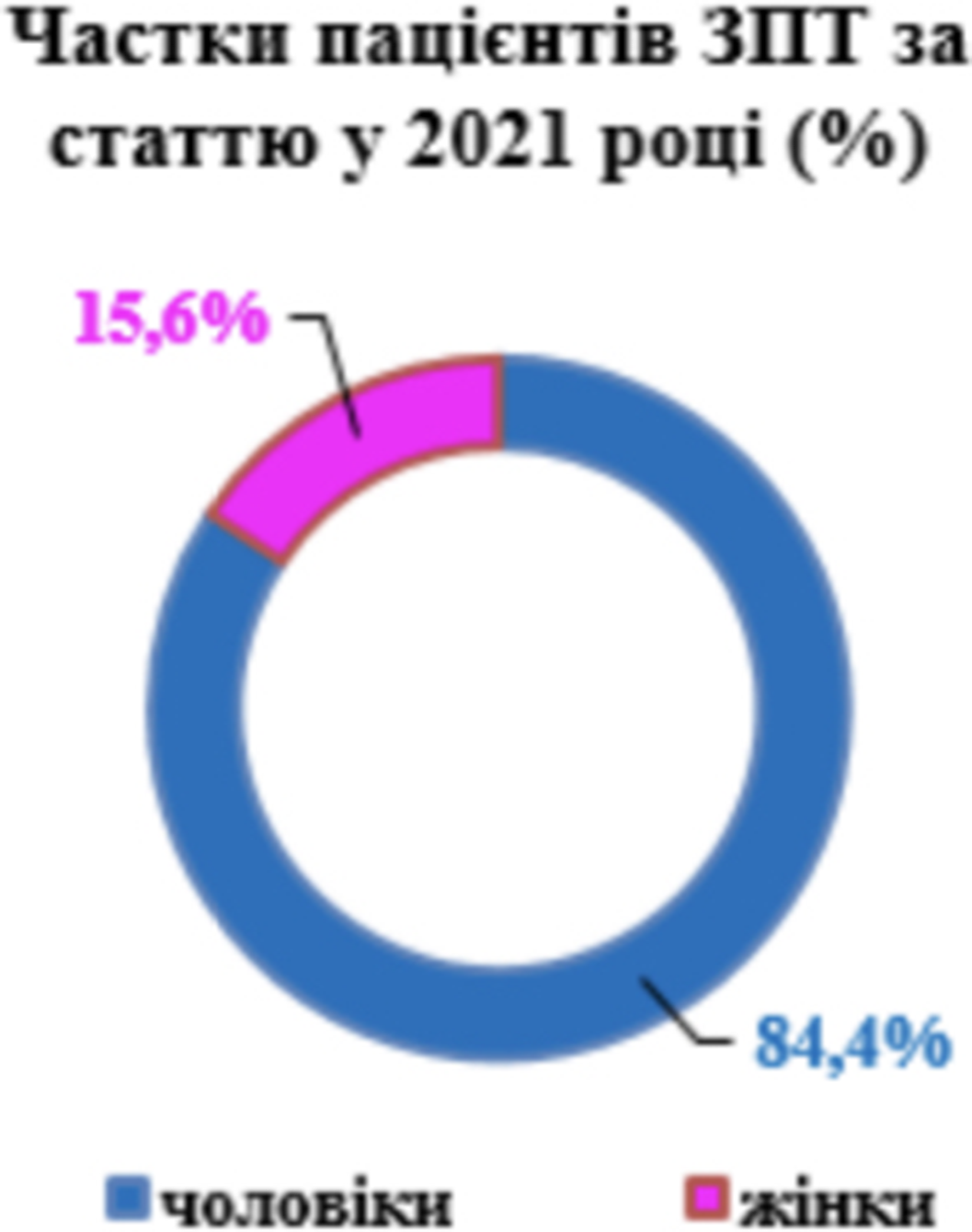
MethodsIn the course of the study, 134 patients aged 26 to 64 years (105 men and 29 women) with a diagnosis of opioid addiction and receiving methadone therapy were examined. Of them, 48 patients had a period of stay at MT of up to three years and 86 – more than three years. The Montreal Cognitive Scale (MoCA) was used to assess comorbid cognitive impairments. The WHOQOL-BREF questionnaire was used to assess the quality of life.
ResultsThe range of indicators of cognitive functions varied from 21 to 29 points (average - 25.3). 61 patients (46%) showed a result of 26 and above, indicating the absence of cognitive impairment, 51 patients (38%) received from 24 to 21, indicating moderate cognitive impairment. 22 patients (16%) had borderline indicators.
When assessing the level of quality of life, indicators of physical and psychological components varied from 12 to 31; self-perception in the range from 10 to 27 points; microsocial support from 3 to 14 points; social well-being from 11 to 36. In general, the level of satisfaction with the quality of life was in the range of 38-83%.
Image:

Image 2:
 Conclusions
ConclusionsOpioid addiction therapy should be consist of an assessment of physical and psychological status, comorbid disorders, quality of life, etc. We can see, MT does not significantly affect the cognitive functions. The differences in the assessment of the quality of life were noted in the components of microsocial support and social well-being, which indicates the vulnerability of patients in these areas. Duration of opioid dependence, availability of psychosocial support, presence of comorbid conditions affect the quality of life. It is important that treatment is tailored to individual needs of patients.
Disclosure of InterestNone Declared


The Influence of Depression in the Evolution of Parkinson’s Disease: A Psychiatric Perspective
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S302
-
- Article
-
- You have access
- Open access
- Export citation
Deliberate self-poisoning in children and adolescents
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S791
-
- Article
-
- You have access
- Open access
- Export citation
Importance of the type of pharmacological treatment in patients with severe mental disorder
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S698-S699
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
The use of long-acting treatments is a common clinical practice in psychiatry. No disease insight and the risk of treatment discontinuation in a significant portion of our patients, increase the demand for psychiatric emergency and hospital admissions. Treatment adherence must be facilitated, taking into account possible side effects and patient´s subjective satisfaction.
Objectives-Evaluate the type of long-acting intramuscular treatment in selected patients. -Evaluate the differences in treatment satisfaction between different types of long-acting intramuscular treatments as well as frequency of psychiatric emergency and hospital admissions in the last year.
MethodsWe select patients with different severe mental disorders who stay in a Medium Stay Unit, Sociosanitary Community Residence, Supervise house and Residence for the elderly in Albacete (Spain); all of them, with intramuscular neuroleptic treatment (zuclopenthixol dihydrochloride, aripiprazole long acting, palmitate paliperidone monthly, 3-monthly and 6-monthly) at least 1 year.
We evaluate their sociodemographic characteristics, the satisfaction questionnaire with the treatment (TSQM-9) and the rate of psychiatric emergencies and admissions after current intramuscular treatment in last year.
ResultsWe have selected 57 patients with an average age of 45.86. 78.94% with a diagnosis of schizophrenia, 12.28% with schizoaffective disorder, 5.26% bipolar disorder and 3.5% unspecified psychotic disorder.
We can see in the graphics below that the longer duration of the intramuscular treatment, the greater satisfaction in all the items of the TSQM-9 questionnaire.
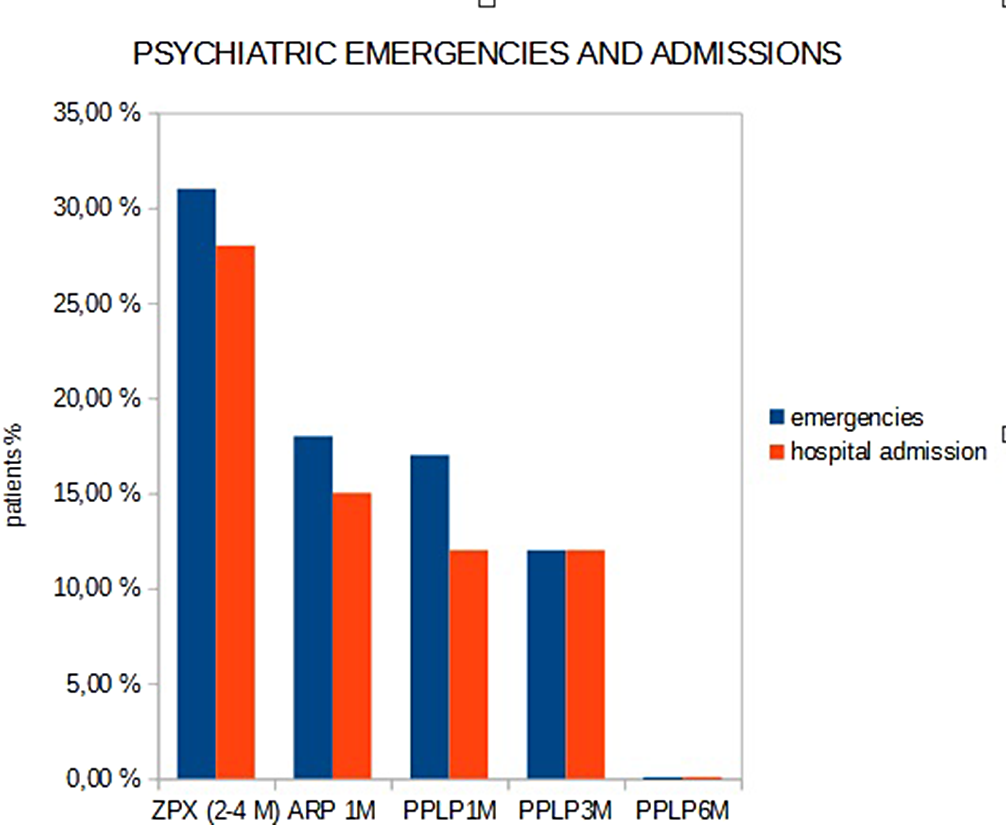
31% of the patients with zuclopenthixol dihydrochloride treatment, have gone to psychiatric emergencies and 28% of psychiatric admissions in the last year.18% of the patients with aripiprazole long acting, 17% with paliperidone palmitate long acting-monthly and 12% de 3-monthly have gone to psychiatric emergencies and 15%, 12% and 12% needed psychiatric admissions respectively. Patients with palmitate long acting-monthly have not emergencies or psychiatric admissions in the last year.
Image:
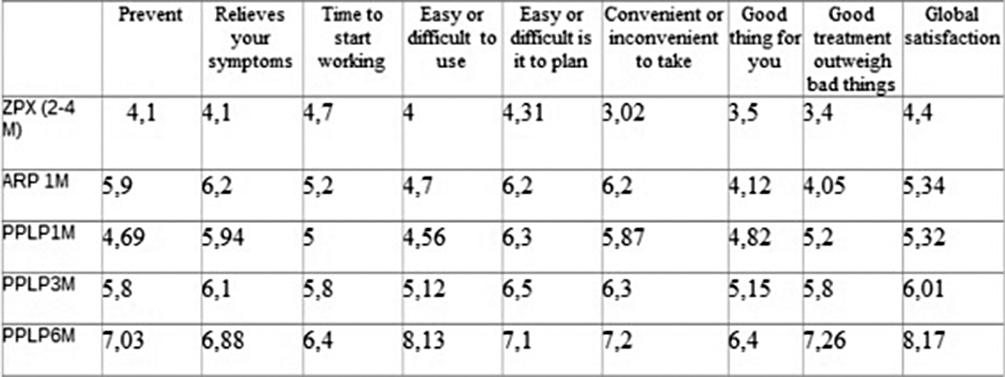
Image 2:
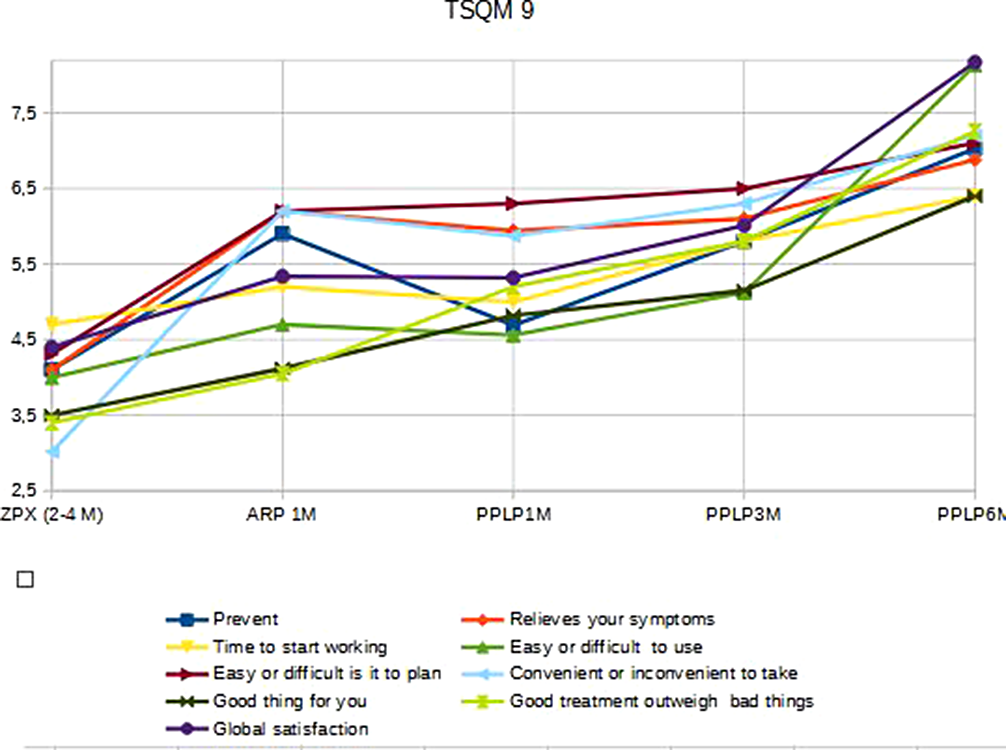
Image 3:
 Conclusions
Conclusions- The longer long acting of the intramuscular treatments, the better patient satisfaction.
- With the longer duration treatment (Palmitate paliperidone LD 6 month), we have lower psychiatric emergencies and hospital admissions.
Disclosure of InterestNone Declared



Multifactorial etiology of manic episodes. About a case
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S433
-
- Article
-
- You have access
- Open access
- Export citation
Christian Humanitarianism, Violence and the Debate over Empire
-
- Journal:
- The Journal of Ecclesiastical History / Volume 75 / Issue 4 / October 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. 758-768
- Print publication:
- October 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The association between glucose 6-phosphate dehydrogenase (G6PD) deficiency and attention deficit/hyperactivity disorder (ADHD)
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S75
-
- Article
-
- You have access
- Open access
- Export citation
A randomized controlled trial comparing trauma-focused treatment with and without concurrent personality disorder treatment in patients with posttraumatic stress disorder and comorbid borderline personality disorder
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S667
-
- Article
-
- You have access
- Open access
- Export citation
Artificial Intelligence in Psychiatry: A Comprehensive Literature Review
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S61
-
- Article
-
- You have access
- Open access
- Export citation
Effectiveness of AI-driven Individualized Learning Approach for Children with Autism Spectrum Disorder (ASD)
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S77
-
- Article
-
- You have access
- Open access
- Export citation
Eating disorder and bipolar mental illness through genome wide association studies
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S555
-
- Article
-
- You have access
- Open access
- Export citation
Improving the Sexual Wellbeing of Patients with Psychotic Illness
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S738-S739
-
- Article
-
- You have access
- Open access
- Export citation
Predictors for Burnout Among Healthcare Workers in a Post -Covid Era
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S499
-
- Article
-
- You have access
- Open access
- Export citation
Haloperidol induced Pisa syndrome in a patient with treatment resistant schizophrenia
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S759
-
- Article
-
- You have access
- Open access
- Export citation
A scoping review of the literature on interventions to reduce stress and burnout among teachers.
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S206-S207
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Experience of chronic stress among professionals is a risk factor for poor mental and physical well-being. There is limited knowledge regarding the kinds of interventions, and outcomes achieved using different modalities to address stress and burnout among teachers.
ObjectivesTo undertake a scoping review of recent literature to determine psychological interventions and reported outcomes related to stress and burnout among teachers.
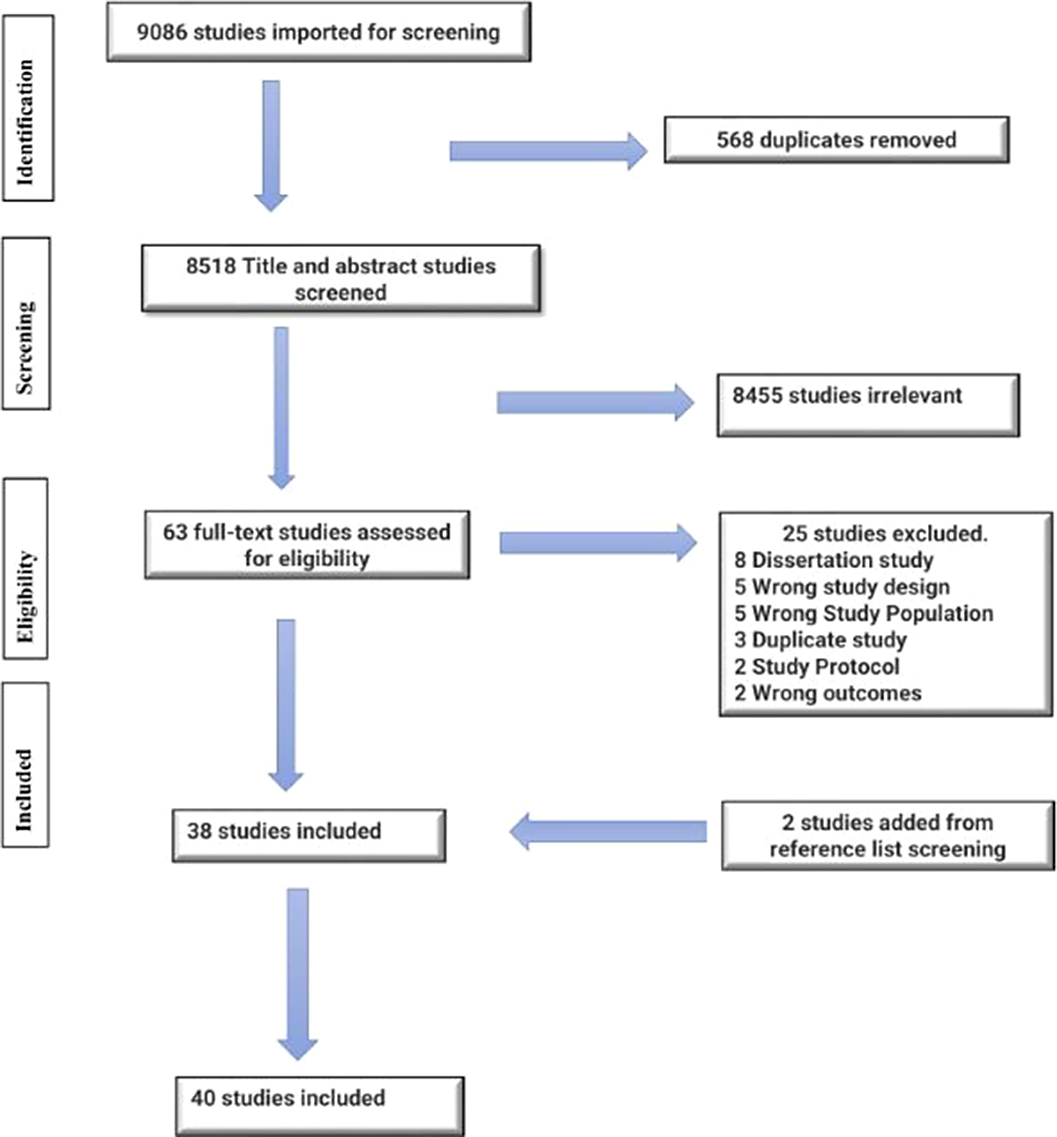
MethodsThe PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews was followed. Relevant search terms were used to determine different interventions adopted to reduce teachers’ stress and burnout. Articles published between 2018 and 2022 were identified using five bibliographic databases. Relevant articles were extracted, reviewed, collated, and thematically analyzed, and findings s were summarized.
ResultsForty studies conducted in Asia, North America, Oceania, Europe, and Africa, met the inclusion criteria. Sixteen kinds of burnout and stress-reduction interventions were identified. The most popularly studied intervention were Mindfulness-Based Interventions alone or in combination with yoga or Cognitive Behavioural Therapy (CBT), followed by Rational Emotive Behavioral Therapy (REBT). Mindfulness-Based Interventions led to decreased overall Teacher Stress Inventory (TSI) and emotional exhaustion subscale scores. REBT, primarily used with special education teachers, especially in Africa, has also shown positive results. Other interventions reporting positive outcomes include Inquiry-Based Stress Reduction (IBSR), the Stress Management and Resiliency Training Program (SMART), Cyclic Meditation, Group Sandplay, Progressive Muscle Relaxation, Autogenic Training, Sport-Based Physical Activity, Emotional Intelligence Ability Models and Christian Prayer and Prayer-Reflection
Image:
 Conclusions
ConclusionsStress and burnout can have a negative impact on teachers and, very often, on the students they teach. Implementing suitable school-based interventions are necessary to improve teachers’ stress-coping ability, reduce the likelihood of burnout and improve general well-being. Policymakers, governments, school boards and administrators should prioritize the implementation of school-based awareness and intervention programs to mitigate teacher stress and burnout.
Disclosure of InterestNone Declared

Psychopathological characterization of nomophobia in a sample of patients with severe mental illness
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, p. S375
-
- Article
-
- You have access
- Open access
- Export citation
Anticipatory competence of adolescents with movement disorders in the prevention of deviations
-
- Journal:
- European Psychiatry / Volume 67 / Issue S1 / April 2024
- Published online by Cambridge University Press:
- 27 August 2024, pp. S659-S660
-
- Article
-
- You have access
- Open access
- Export citation
