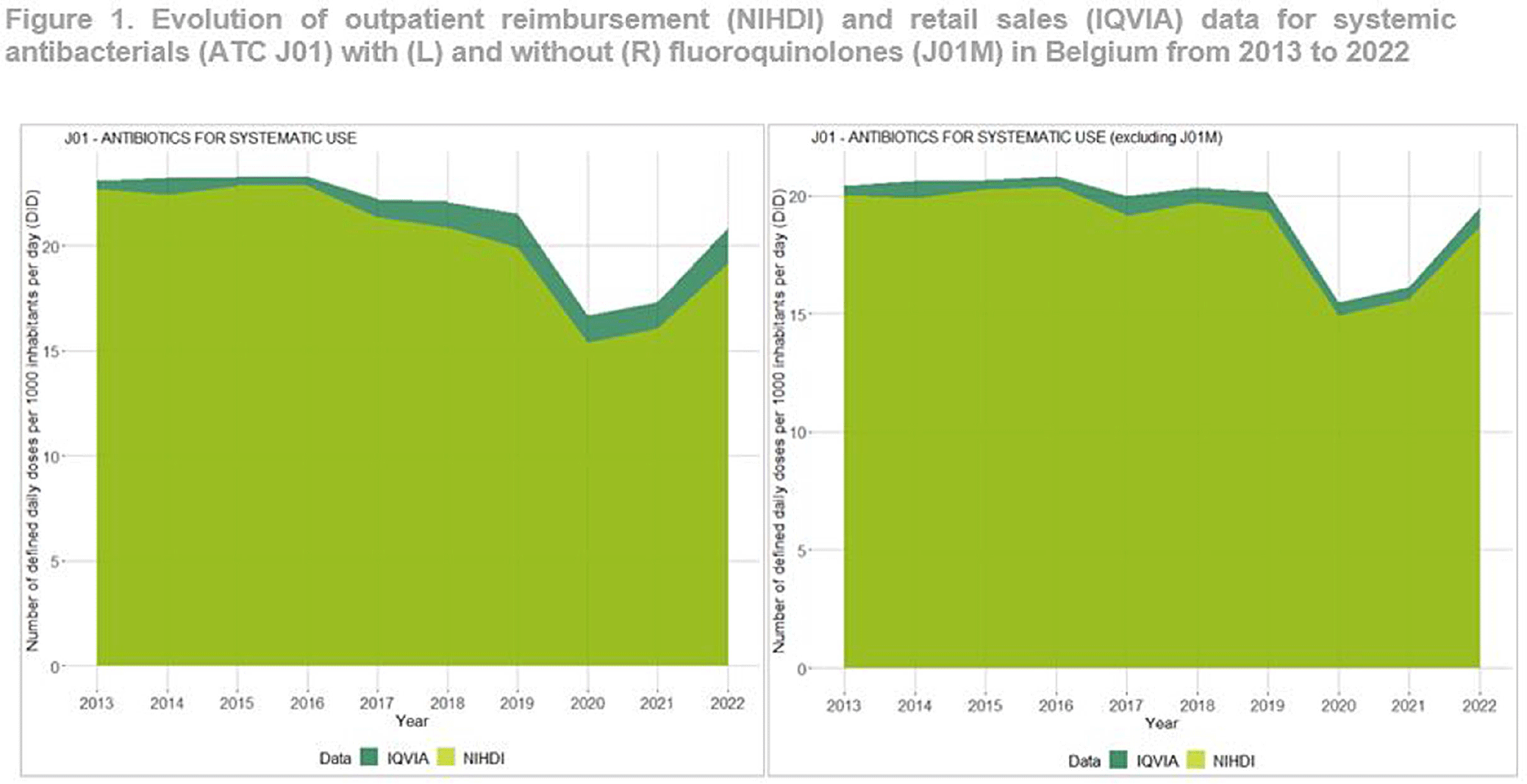
Background: Antimicrobial resistance (AMR) is a global public health concern, necessitating close and timely monitoring of antibiotic consumption (AMC). In Belgium, AMC surveillance traditionally relies on reimbursement data, excluding over-the-counter non-reimbursed or imported products and involving a time lag. This study investigates disparities in AMC between reimbursement data and retail data, providing insights into AMC variations. Additionally this study seeks to critically evaluate the validity and representativeness of the reimbursed data in accurately reflecting the true extent of AMC in the country. Method: Utilizing reimbursement data from the National Institute for Health and Disability Insurance (NIHDI) and retail data (IQVIA Sales data; www.iqvia.com) for systemic antibacterials (ATC Group J01), outpatient consumption was estimated for the period 2013-2022. Volume of antimicrobials was measured in Defined Daily Doses (DDDs - WHO ATC/DDD Index 2023), while population data were extracted from Eurostat. Relative differences (RDs) in DDDs per 1000 inhabitants per day (DID) were computed, and validated through correlation analysis (Pearson’s r) and Bland–Altman plots. Result: J01 antibacterial sales declined from 23.10 DID (2013) to 20.85 (2022). Non-linear decreases, notably during the Covid-19 pandemic (21.54 DID in 2019 to 16.69 in 2020), followed by a rebound to pre-pandemic quantities in 2022 were observed (Figure 1). Reimbursement NIHDI data slightly underestimated IQVIA sales, with RDs ranging from 2% (2013) to 9% (2022). Notable differences, especially in recent years were attributed to quinolone reimbursement criteria changes implemented by law in Belgium in 2018, reducing the reimbursed proportion from 99% (2017) to 35% (2022). ATC-3 level analysis revealed disparities in low-DID groups (J01B, J01E and J01G). Notably, a small proportion of amphenicols (J01B) were reimbursed ( < 1 0%), with a congestion relieving combination product of tiamphenicol (+ N-acetylcysteine; Fluimucil®) frequently bought and remaining unreimbursed. Overall and across ATC3 groups, the correlation between NIDHI and IQVIA estimates was almost perfect across years and the Bland–Altman plots showed high agreement. Conclusion: Reimbursement data are reliable for outpatient AMC monitoring with slightly lower estimates than retail data across most categories. The 2018 quinolone reimbursement criteria change highlights the necessity of incorporating retail data for accurate assessments in this specific category. The synergistic use of reimbursement and retail datasets is crucial for a comprehensive understanding of consumption patterns, supporting effective AMR mitigation strategies in Belgium.
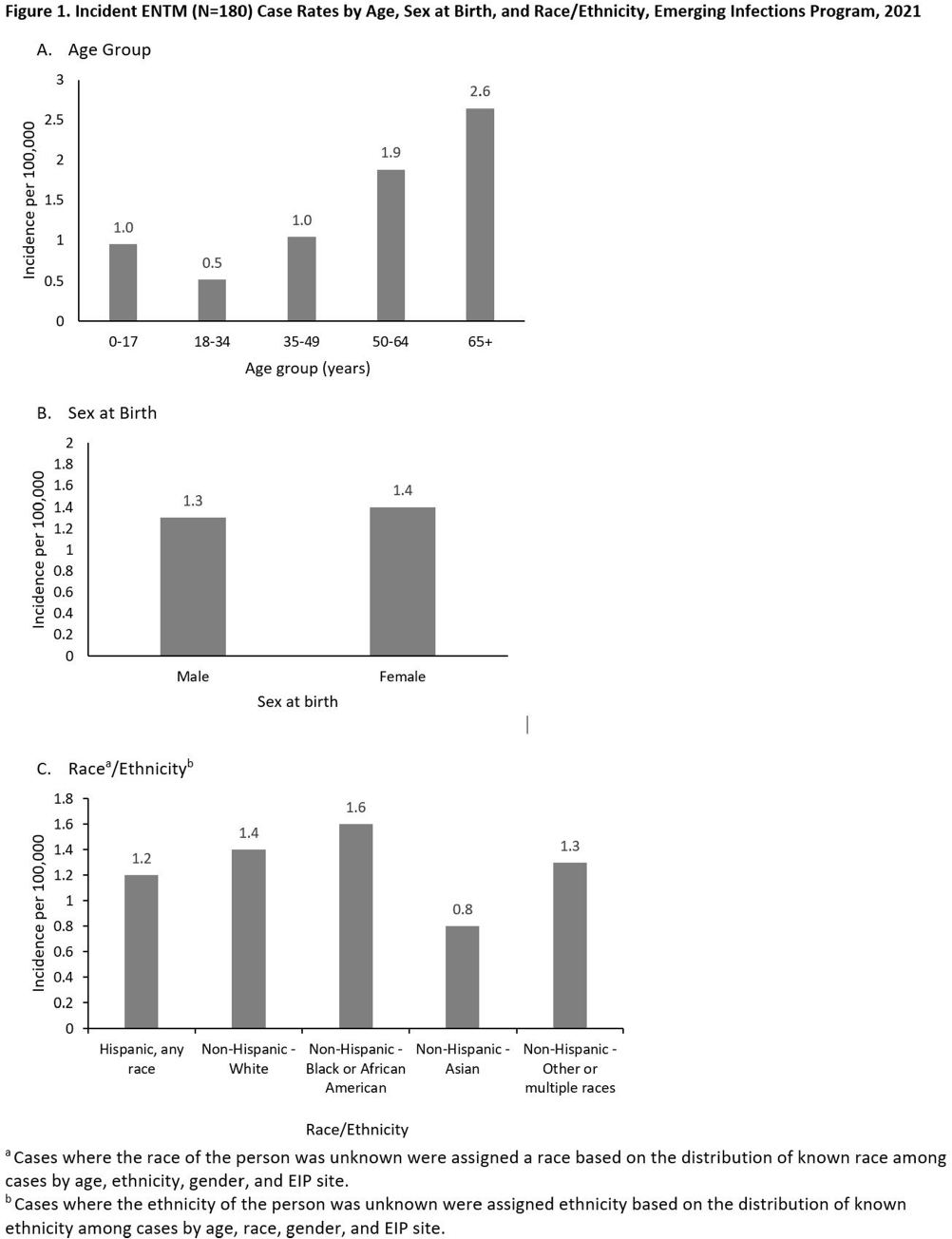
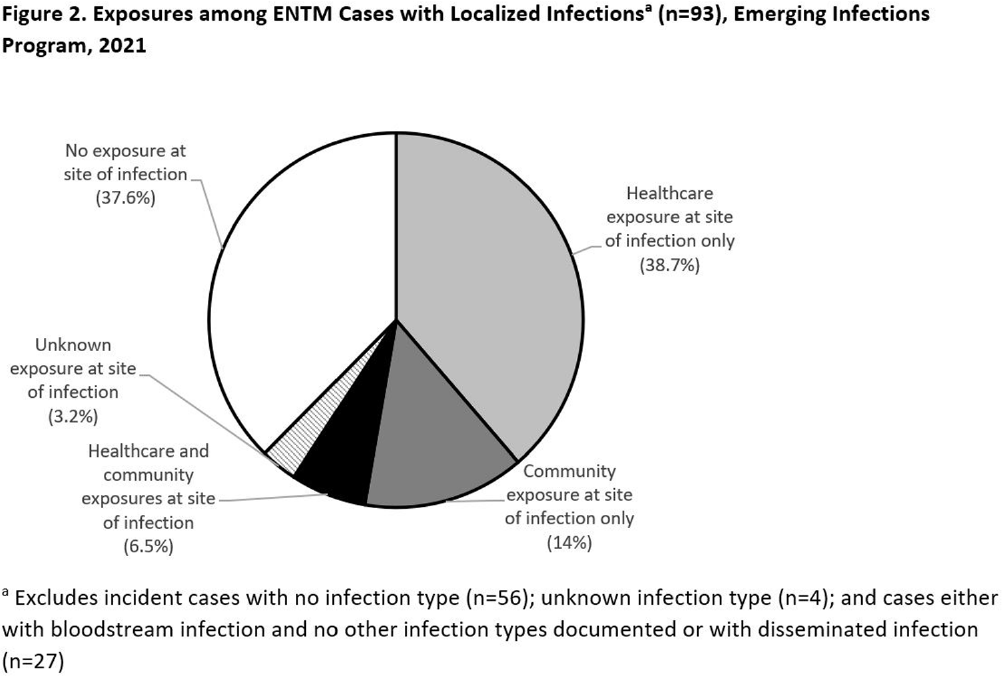
Background: Extrapulmonary nontuberculous mycobacteria (ENTM) infections are difficult to treat and often require prolonged therapy or surgery. Few population-based studies describe ENTM epidemiology, though well-known healthcare-associated outbreaks have occurred. Using the first year of multi-site ENTM surveillance, we characterized rates and how frequently ENTM infections may be related to healthcare. Methods: CDC’s Emerging Infections Program conducted active, laboratory- and population-based surveillance for ENTM cases in 4 sites (Colorado [5 counties], Minnesota [statewide], New York [1 county], and Oregon [statewide]) in 2021. An incident ENTM case was NTM isolation from a non-pulmonary specimen, excluding stool or rectal swabs, in a resident of the surveillance area without either medical record documentation of prior ENTM infection or isolation of ENTM in the prior 12 months. Demographic, clinical, information on selected healthcare and community exposures, and laboratory data were collected via medical record review. We calculated incidence per 100,000 population using U.S. Census population estimates and performed descriptive analyses. Results: A total of 180 incident ENTM cases were reported in 2021. The crude annual incidence rate was 1.3 per 100,000 persons. Incidence increased with age (from 0.95 per 100,000 among 0–17 year-olds to 2.65 per 100,000 among persons ≥65), ranged from 0.8 among non-Hispanic Asian persons to 1.6 per 100,000 in non-Hispanic Black persons, and was similar among males (1.3 per 100,000) and females (1.4 per 100,000; Figure 1). Mycobacterium avium complex (64 [35.6%]) was the most frequently isolated species group, followed by Mycobacterium chelonae complex (31 [17.2%]). Skin and soft tissue infections were the most frequent infection type (37 [20.6%]); 27 cases (15.0%) were associated with disseminated and/or only bloodstream infection, and 56 cases (31.1%) had no infection type documented. Among 93 cases with localized ENTM infections (i.e., infections that were not disseminated and/or only bloodstream infections), 38.7% had only healthcare-related exposures, 14% had only community-related exposures and 6.5% had both exposure types at the site of infection (Figure 2). Healthcare-related exposures at the infection site included surgery (23.7%), injection/infusion (21.5%), and medical devices (18.3%). The most frequent community-related exposure at the infection site was trauma (17.2%). Only one case was part of a known outbreak, which was healthcare-associated. Conclusions: ENTM infections are relatively rare, but nearly half of patients with localized ENTM infections had prior healthcare-related exposures. This indicates that the burden of ENTM infections related to healthcare may be much larger than what has been suggested from reported outbreaks.
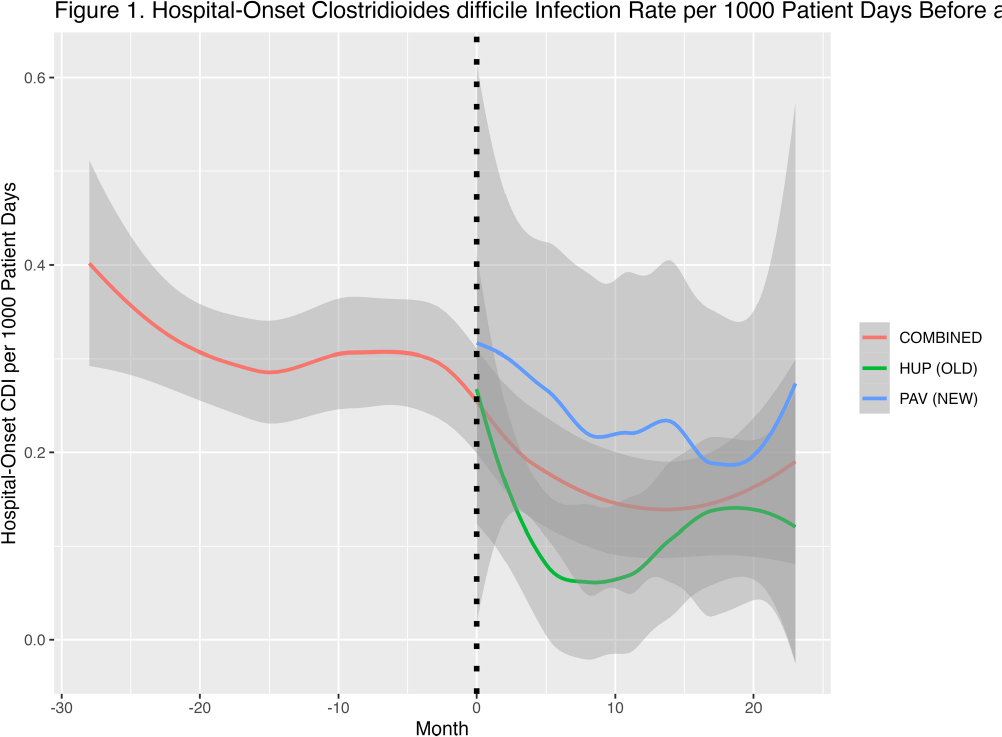
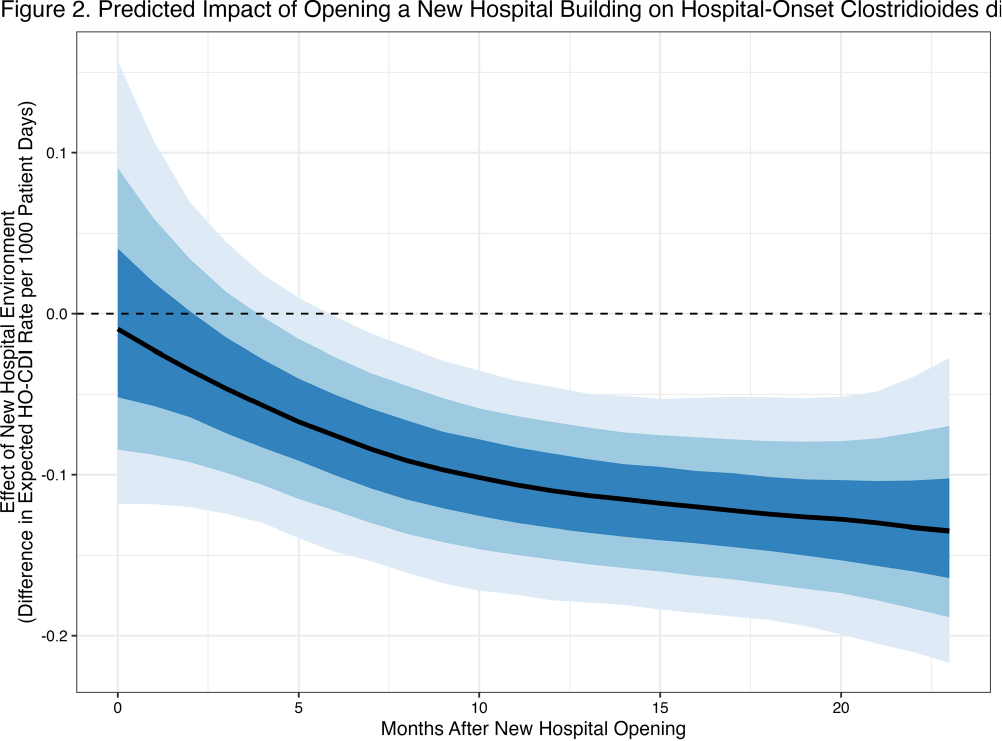
Background: Prior research has implicated contaminated surfaces in the transmission of Clostridioides difficile within the hospital. To reduce the risk of transmission, enhanced environmental hygiene is performed in rooms of patients with known C.difficile infection (CDI). We wished to evaluate the residual impact of environmental surfaces on hospital-onset CDI (HO-CDI) by comparing HO-CDI rates before and after the opening of a new 504-bed hospital building, HUP Pavilion (PAV). We hypothesized that we would observe a reduction in HO-CDI after opening of PAV due to a reduced burden of C.difficile spores in the environment. Methods: We included NHSN reported HO-CDI rates for 28 months prior and 24 months after opening of PAV. Upon opening, patients were divided between the old building (HUP) and PAV. We included all patient units before and after opening. We created hierarchical models of HO-CDI rates using Stan Hamiltonian Monte Carlo (HMC) version 2.30.1, via the “cmdstanr” and “brms” packages with a GAM smooth function by month and intervention period with default, weakly-informative priors. Results: At baseline, there was an average of approximately 20,100 patient days per month, subsequently divided between HUP and PAV (mean 10,100 and 12,100 patient days per month). After opening of PAV, we observed a reduced HO-CDI rate (mean 0.21 vs 0.31 per 1000 patient days, P=0.01). When comparing the two specific buildings after opening of PAV, there was a greater reduction noticed in the old building (HUP) as compared to the new building (PAV) (0.12 vs 0.29 per 1000 patient days) (Figure 1). The predicted contrast in HO-CDI rate (Figure 2), shows no immediate change in HO-CDI after opening, however a sustained reduction estimated at 0.1 HO-CDI events per 1000 patient days for the duration of follow-up. Conclusions: We observed a reduction in HO-CDI rates after the opening of a new hospital building. The difference in HO-CDI rates between hospital buildings after the move is likely due to the concentration of high-risk patient cohorts within this building. Our findings suggests that there remains an opportunity to reduce HO-CDI through environmental hygiene. However, it is possible that other factors beyond surface environment contributed to an observed reduction in HO-CDI, including other concurrent infection control interventions that focused on smaller populations within the hospital. In future work we will investigate the durability of this observed effect with additional analyses including patient-level risk for HO-CDI.