Anticholinergic medications block cholinergic transmission. The central effects of anticholinergic drugs can be particularly marked in patients with dementia. Furthermore, anticholinergics antagonise the effects of cholinesterase inhibitors, the main dementia treatment.
This study aimed to assess anticholinergic drug prescribing among dementia patients before and after admission to UK acute hospitals.
352 patients with dementia were included from 17 hospitals in the UK. All were admitted to surgical, medical or Care of the Elderly wards in 2019. Information about patients’ prescriptions were recorded on a standardised form. An evidence-based online calculator was used to calculate the anticholinergic drug burden of each patient. The correlation between two subgroups upon admission and discharge was tested with Spearman’s Rank Correlation.
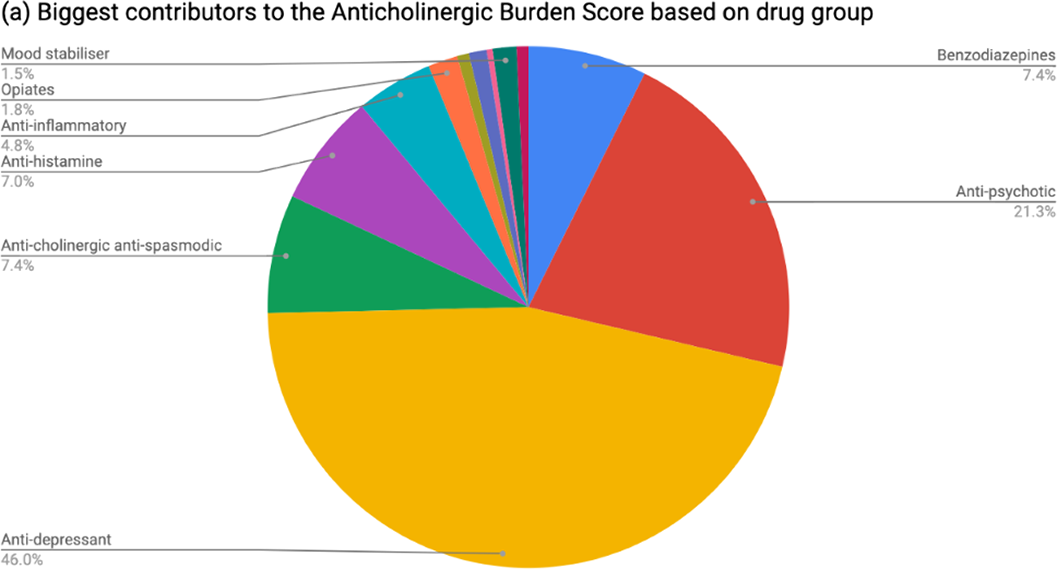
Table 1 shows patient demographics. On admission, 37.8% of patients had an anticholinergic burden score ≥1 and 5.68% ≥3. At discharge, 43.2% of patients had an anticholinergic burden score ≥1 and 9.1% ≥3. The increase was statistically significant (rho 0.688; p=2.2x10-16). The most common group of anticholinergic medications prescribed at discharge were psychotropics (see Figure 1). Among patients prescribed cholinesterase inhibitors, 44.9% were also taking anticholinergic medications.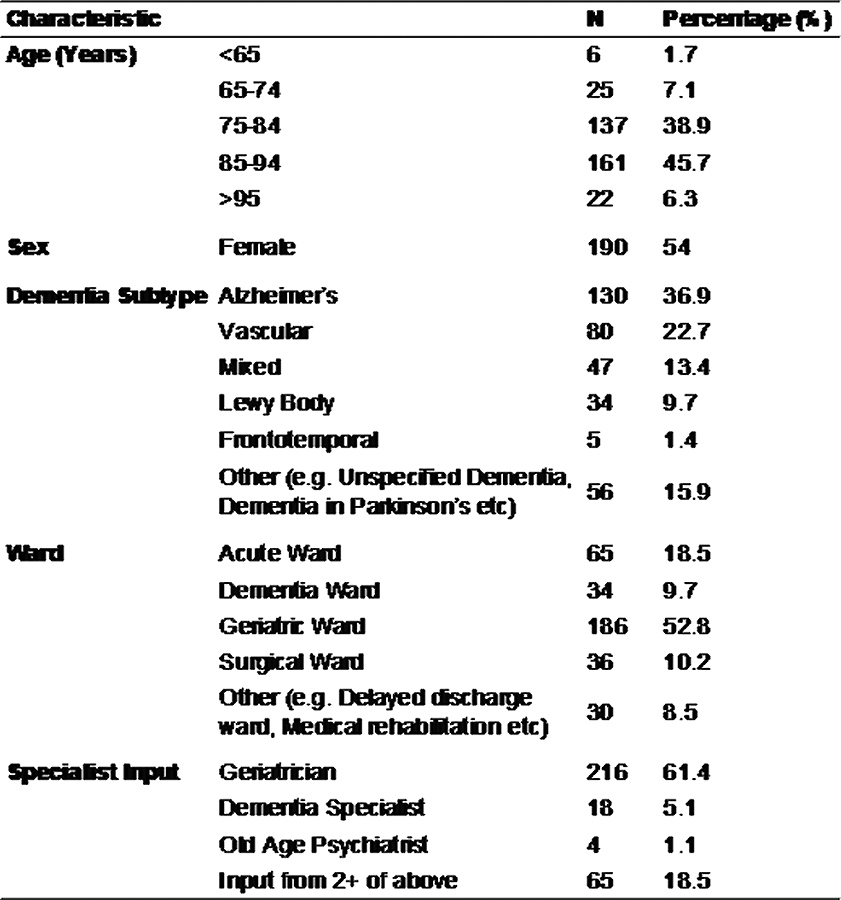
This multicentre cross-sectional study found that people with dementia are frequently prescribed anticholinergic drugs, even if also taking cholinesterase inhibitors, and are significantly more likely to be discharged with a higher anticholinergic drug burden than on admission to hospital.
This project was planned and executed by the authors on behalf of SPARC (Student Psychiatry Audit and Research Collaborative). We thank the National Student Association of Medical Research for allowing us use of the Enketo platform. Judith Harrison was su
Remote consultation technology has been rapidly adopted due to the COVID-19 pandemic. However, some healthcare settings have faced barriers in implementation. We present a study to investigate changes in rates of remote consultation during the pandemic using a large electronic health record (EHR) dataset.
The Clinical Record Interactive Search tool (CRIS) was used to examine de-identified EHR data of people receiving mental healthcare in South London, UK. Data from around 37,500 patients were analysed for each week from 7th January 2019 and 20th September 2020 using linear regression and locally estimated scatterplot smoothing (LOESS) to investigate changes in the number of clinical contacts (in-person, remote or non-attended) with mental healthcare professionals and prescribing of antipsychotics and mood stabilisers. The data are presented in an interactive dashboard: http://rpatel.co.uk/TelepsychiatryDashboard.
The frequency of in-person contacts was substantially reduced following the onset of the pandemic (β coefficient: -5829.6 contacts, 95% CI -6919.5 to -4739.6, p<0.001), while the frequency of remote contacts increased significantly (β coefficient: 3338.5 contacts, 95% CI 3074.4 to 3602.7, p<0.001). Rates of remote consultation were lower in older adults than in working age adults, children and adolescents. Despite the increase in remote contact, antipsychotic and mood stabiliser prescribing remained at similar levels.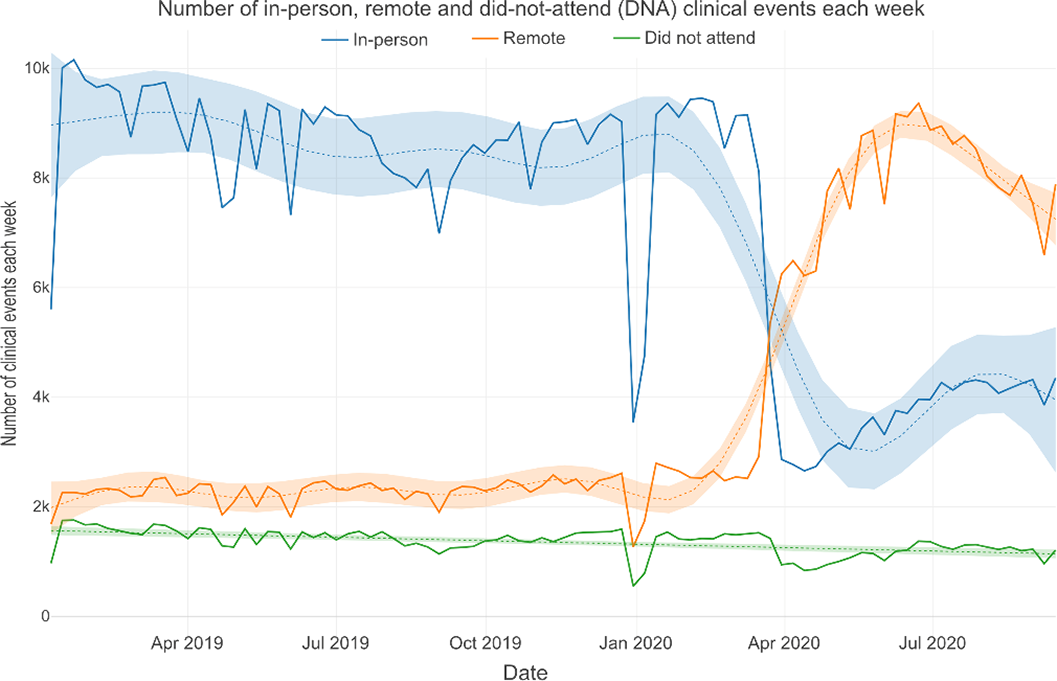
The COVID-19 pandemic has been associated with a marked increase in remote consultation, particularly among younger patients. However, there was no evidence that this has led to changes in prescribing. Further work is needed to support older patients in accessing remote mental healthcare.
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: RS has received funding from Janssen, GSK and Takeda outside the submitted work. RP has received funding from Janssen, Induction Healthcare and H

