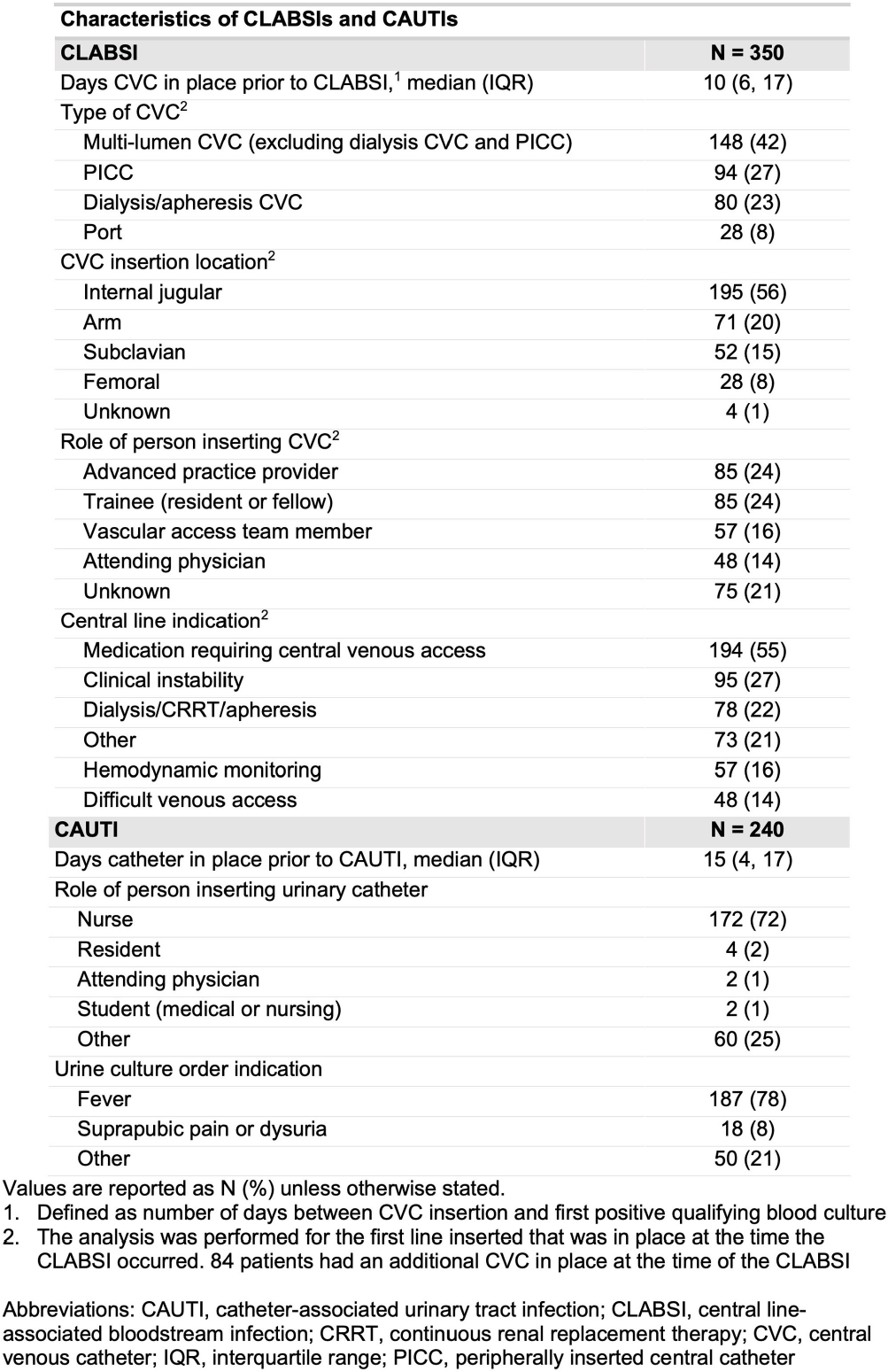
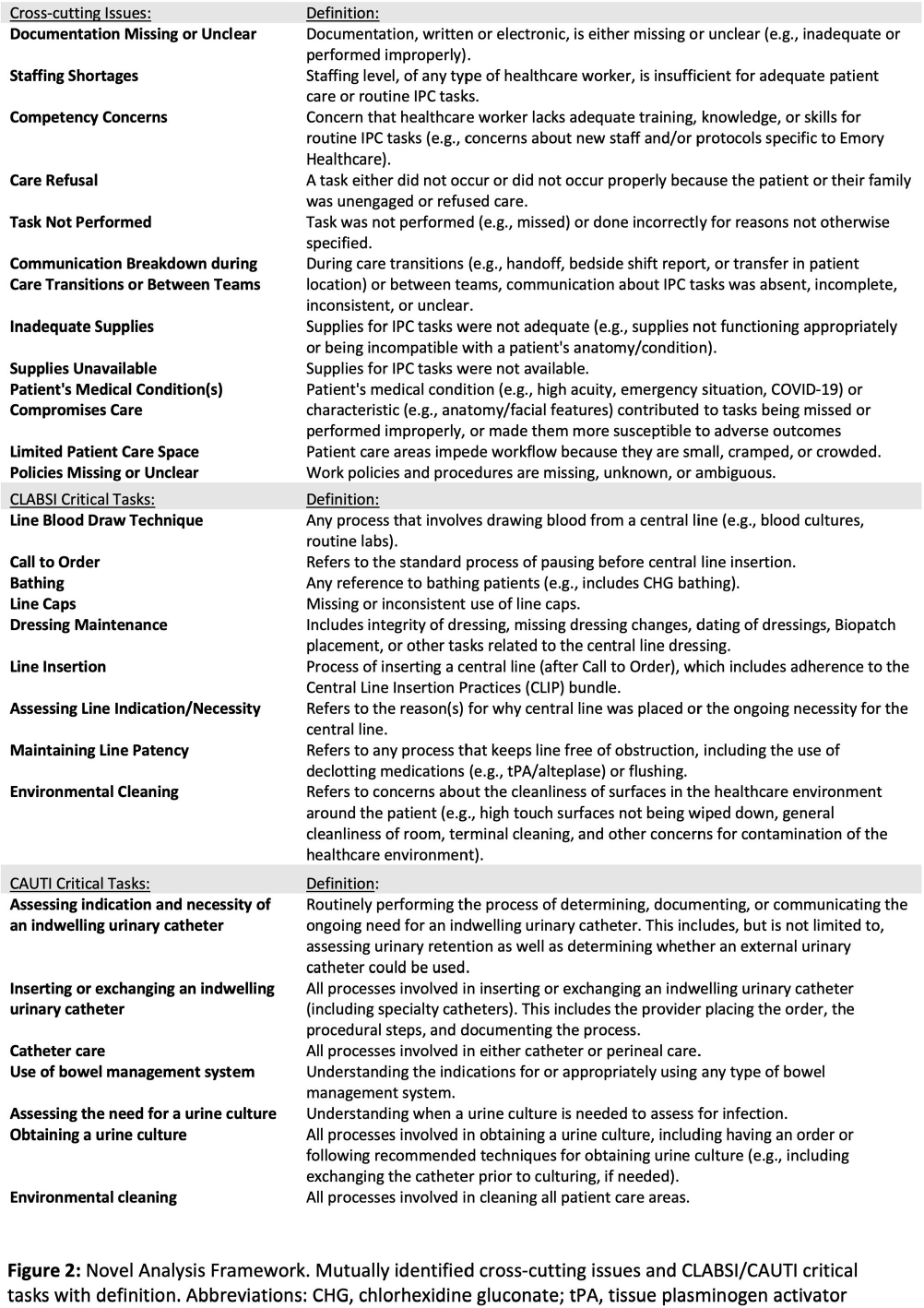
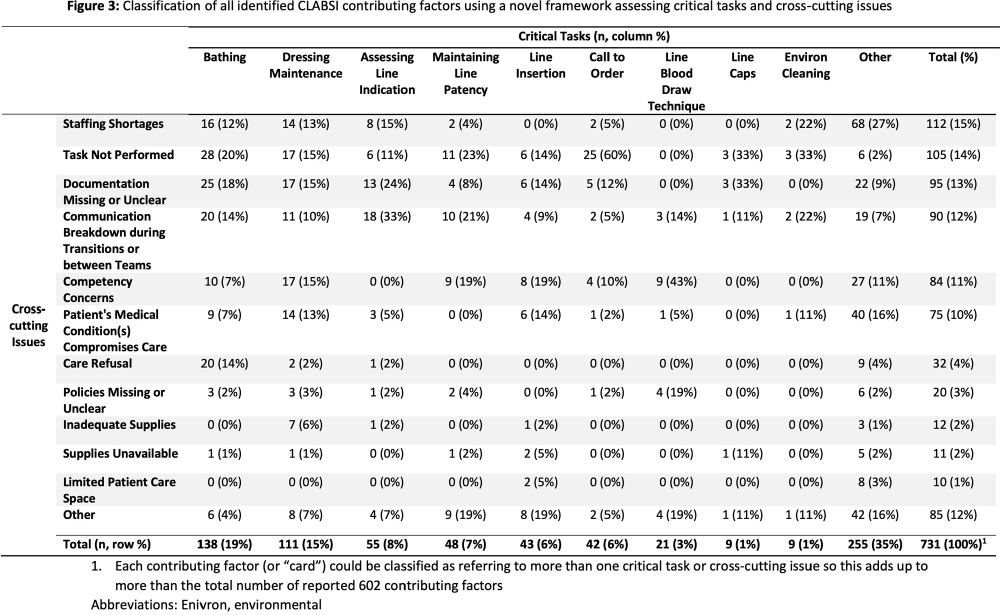
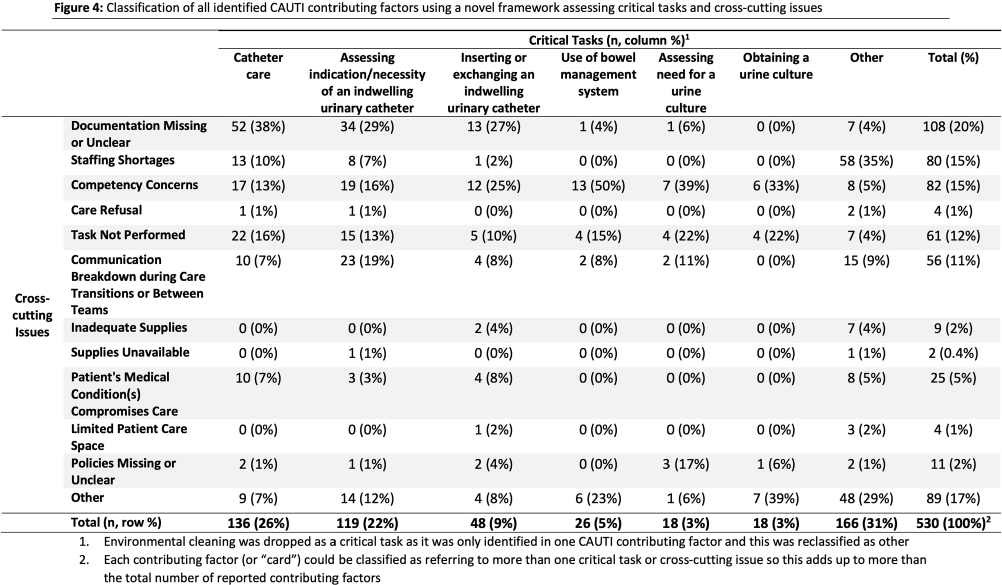
Background: Central line-associated bloodstream infections (CLABSI) and catheter-associated urinary tract infections (CAUTI) are key healthcare-associated infection (HAI) quality metrics. In this qualitative analysis, we aimed to identify common issues contributing to CLABSIs and CAUTIs occurring during the COVID-19 pandemic. Methods: In an academic healthcare network in Atlanta, GA, four hospitals perform real-time, apparent cause analyses (ACAs) for all CLABSIs and CAUTIs. Contributing factors are entered as free text into an electronic database. We analyzed data from 8/2020–8/2022. We first performed a qualitative open card sort of all reported contributing factors to CLABSI and created a novel framework based on mutually defined critical tasks (e.g., line insertion) and cross-cutting issues (e.g., communication breakdown). Contributing factors could describe ≥1 critical task and/or ≥1 cross-cutting issue. After establishing interrater reliability, a multidisciplinary group applied this framework to classify each contributing factor. For CAUTI, we used the same set of cross-cutting issues but identified new critical tasks via open card sorting. We then used the framework to classify each CAUTI contributing factor. We used descriptive statistics to identify frequent critical tasks and cross-cutting issues. Results: We reviewed 350 CLABSI ACAs with 602 contributing factors and 240 CAUTI ACAs with 405 contributing factors (Figure 1). Our classification framework comprised 11 cross-cutting issues and 9 critical tasks for CLABSI and 7 critical tasks for CAUTI (Figure 2). CLABSI: The critical tasks most often reported were bathing (19%), central line dressing maintenance (15%), and assessing central line indication (8%; Figure 3). Within these tasks, the most frequent issues described for bathing were the task not being performed (20%) and unclear documentation (18%); for dressing maintenance, the task was not performed (15%), not documented (15%), or poorly performed due to lack of competency (15%); and for assessing line indication, there was frequent communication breakdown (33%). CAUTI: The critical tasks most often reported were urinary catheter care (26%) and assessing the indication for urinary catheter (22%; Figure 4). Within these tasks, urinary catheter care was frequently not documented (38%) or not performed (16%); assessing urinary catheter necessity was often not documented (29%) or involved breakdown of communication (19%). Conclusion: We created a novel framework to evaluate common causes of HAIs in an academic healthcare network. This framework can be used to identify and track gaps over time and to develop quality improvement initiatives targeting key tasks and associated factors, such as communication difficulties when assessing device indications.
Disclosure: Colleen Kraft: Consultant - REbiotix/Ferring; Scientific Advisory Board - Seres, LLC
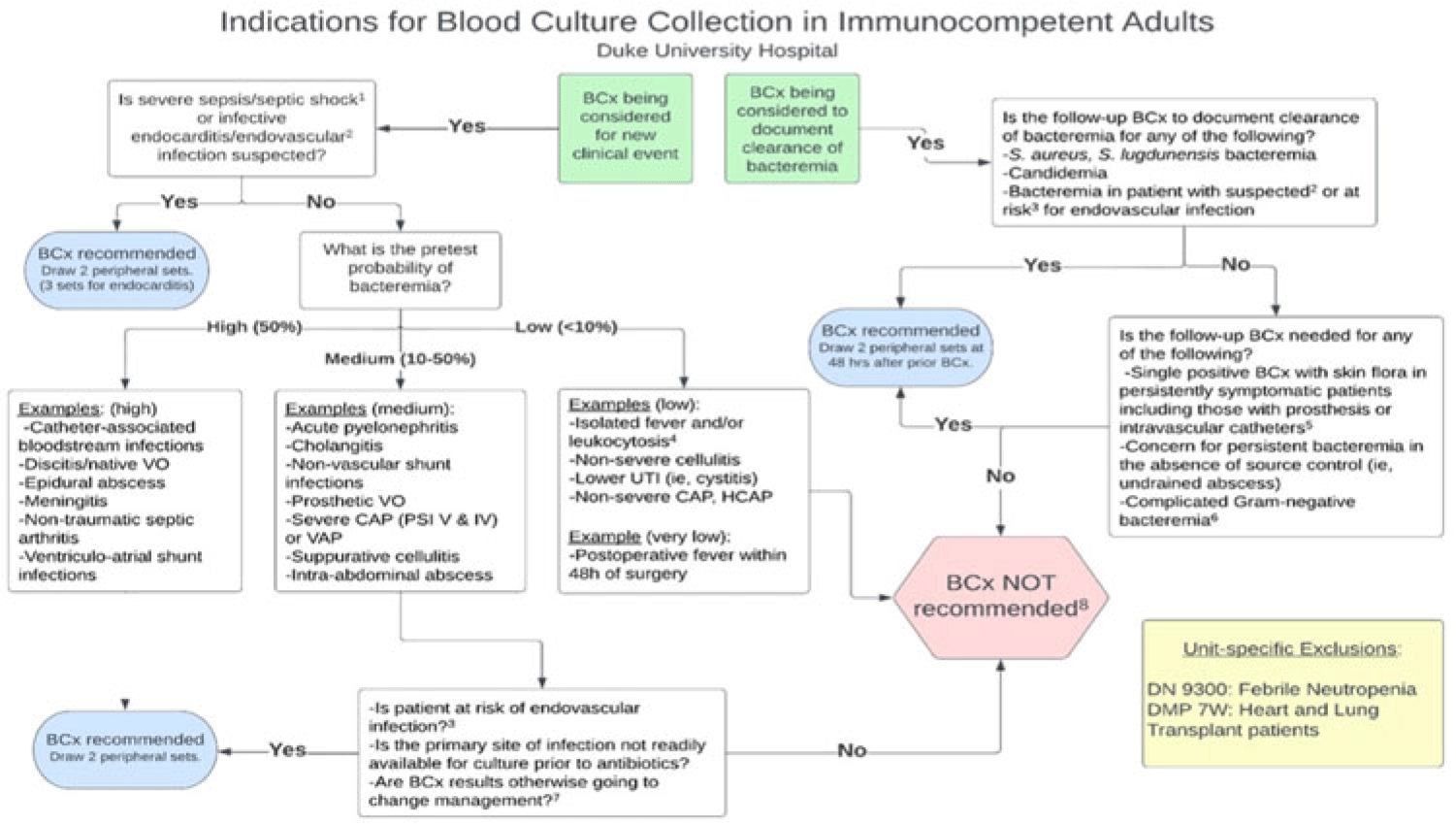
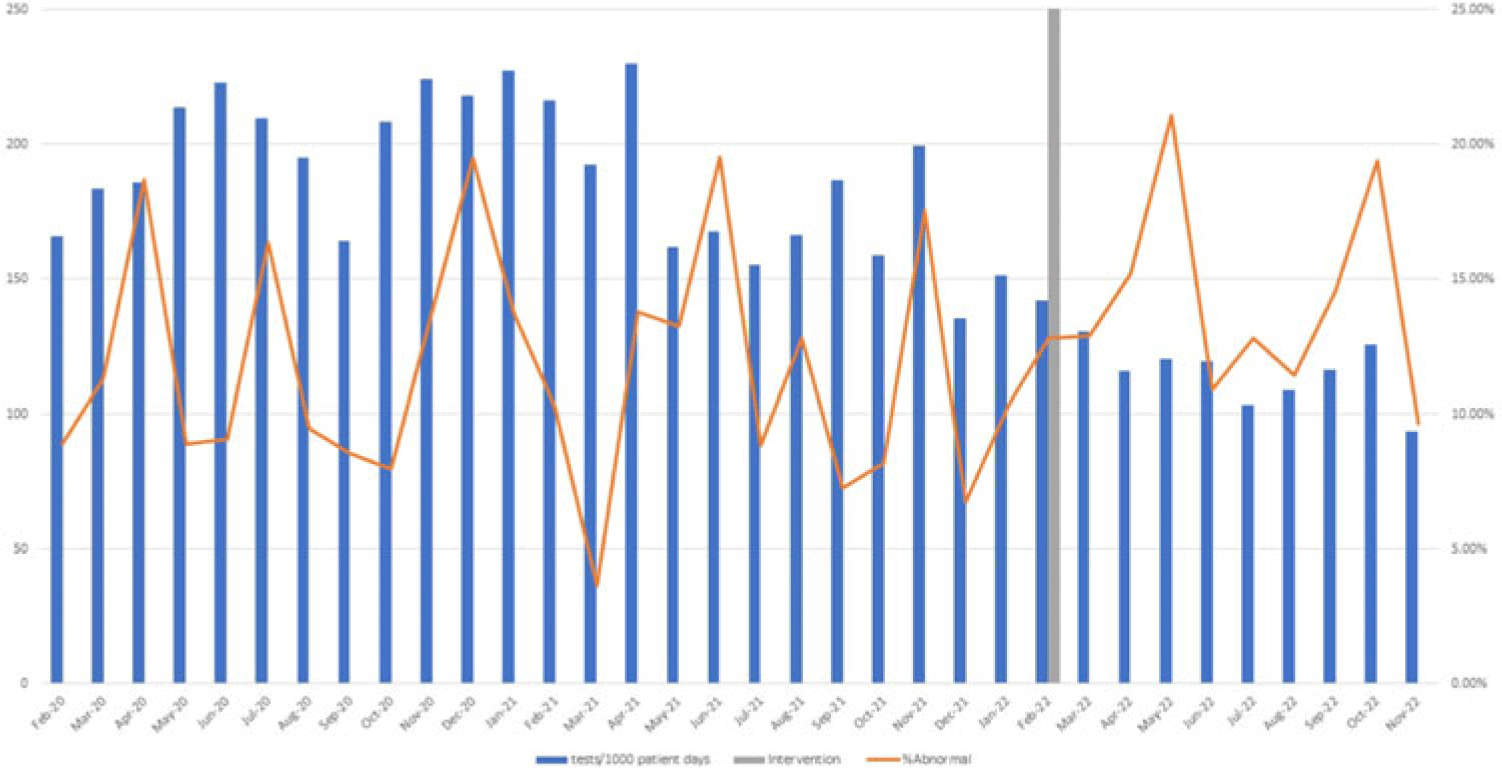
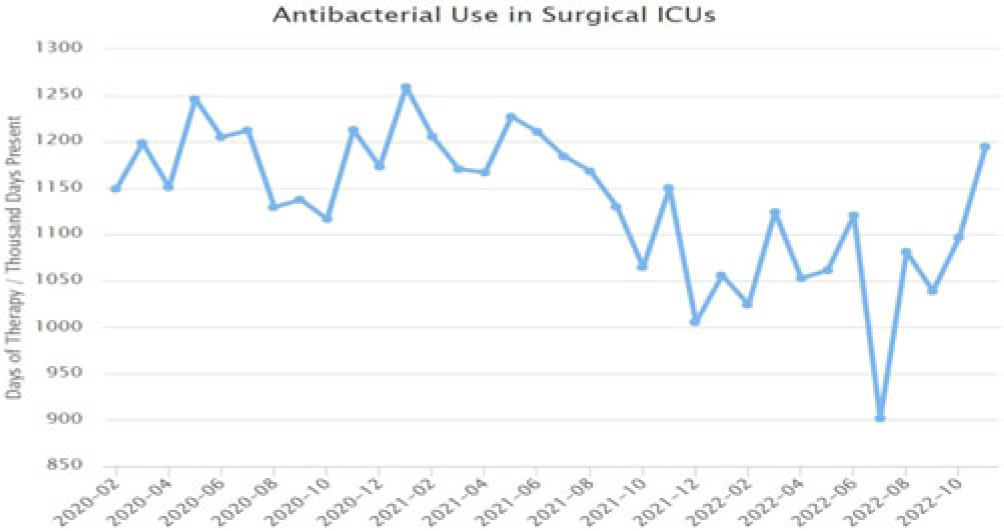
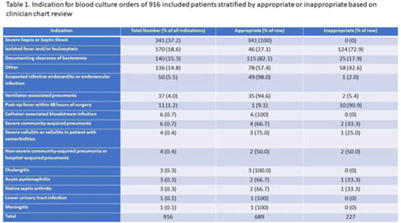
Background: Blood cultures are commonly ordered for patients with low risk of bacteremia. Liberal blood-culture ordering increases the risk of false-positive results, which can lead to increased length of stay, excess antibiotics, and unnecessary diagnostic procedures. We implemented a blood-culture indication algorithm with data feedback and assessed the impact on ordering volume and percent positivity. Methods: We performed a prospective cohort study from February 2022 to November 2022 using historical controls from February 2020 to January 2022. We introduced the blood-culture algorithm (Fig. 1) in 2 adult surgical intensive care units (ICUs). Clinicians reviewed charts of eligible patients with blood cultures weekly to determine whether the blood-culture algorithm was followed. They provided feedback to the unit medical directors weekly. We defined a blood-culture event as ≥1 blood culture within 24 hours. We excluded patients aged <18 years, absolute neutrophil count <500, and heart and lung transplant recipients at the time of blood-culture review. Results: In total, 7,315 blood-culture events in the preintervention group and 2,506 blood-culture events in the postintervention group met eligibility criteria. The average monthly blood-culture rate decreased from 190 blood cultures per 1,000 patient days to 142 blood cultures per 1,000 patient days (P < .01) after the algorithm was implemented. (Fig. 2) The average monthly blood-culture positivity increased from 11.7% to 14.2% (P = .13). Average monthly days of antibiotic therapy (DOT) was lower in the postintervention period than in the preintervention period (2,200 vs 1,940; P < .01). (Fig. 3) The ICU length of stay did not change before the intervention compared to after the intervention: 10 days (IQR, 5–18) versus 10 days (IQR, 5–17; P = .63). The in-hospital mortality rate was lower during the postintervention period, but the difference was not statistically significant: 9.24% versus 8.34% (P = .17). The all-cause 30-day mortality was significantly lower during the intervention period: 11.9% versus 9.7% (P < .01). The unplanned 30-day readmission percentage was significantly lower during the intervention period (10.6% vs 7.6%; P < .01). Over the 9-month intervention, we reviewed 916 blood-culture events in 452 unique patients. Overall, 74.6% of blood cultures followed the algorithm. The most common reasons overall for ordering blood cultures were severe sepsis or septic shock (37%), isolated fever and/or leukocytosis (19%), and documenting clearance of bacteremia (15%) (Table 1). The most common indications for inappropriate blood cultures were isolated fever and/or leukocytosis (53%). Conclusions: We introduced a blood-culture algorithm with data feedback in 2 surgical ICUs and observed decreases in blood-culture volume without a negative impact on ICU LOS or mortality rate.
Disclosure: None

