Aircraft with bio-inspired flapping wings that are operated in low-density atmospheric environments encounter unique challenges associated with the low density. The low density results in the requirement of high operating velocities of aircraft to generate sufficient lift resulting in significant compressibility effects. Here, we perform numerical simulations to investigate the compressibility effects on the lift generation of a bio-inspired wing during hovering flight using an immersed boundary method. The aim of this study is to develop a scaling law to understand how the lift is influenced by the Reynolds and Mach numbers, and the associated flow physics. Our simulations have identified a critical Mach number of approximately  $0.6$ defined by the average wing-tip velocity. When the Mach number is lower than 0.6, compressibility does not have significant effects on the lift or flow fields, while when the Mach number is greater than
$0.6$ defined by the average wing-tip velocity. When the Mach number is lower than 0.6, compressibility does not have significant effects on the lift or flow fields, while when the Mach number is greater than  $0.6$, the lift coefficient decreases linearly with increasing Mach number, due to the drastic change in the pressure on the wing surface caused by unsteady shock waves. Moreover, the decay rate is dependent on the Reynolds number and the angle of attack. Based on these observations, we propose a scaling law for the lift of a hovering flapping wing by considering compressible and viscous effects, with the scaled lift showing excellent collapse.
$0.6$, the lift coefficient decreases linearly with increasing Mach number, due to the drastic change in the pressure on the wing surface caused by unsteady shock waves. Moreover, the decay rate is dependent on the Reynolds number and the angle of attack. Based on these observations, we propose a scaling law for the lift of a hovering flapping wing by considering compressible and viscous effects, with the scaled lift showing excellent collapse.
The effects of the evolution of vortices on the aeroacoustics generated by a hovering wing are numerically investigated by using a hybrid method of an immersed boundary–finite difference method for the three-dimensional incompressible flows and a simplified model based on the Ffowcs Williams-Hawkings acoustic analogy. A low-aspect-ratio ( $AR=1.5$) rectangular wing at low Reynolds (
$AR=1.5$) rectangular wing at low Reynolds ( $Re=1000$) and Mach (
$Re=1000$) and Mach ( $M=0.04$) numbers is investigated. Based on the simplified model, the far-field acoustics is shown to be dominated by the time derivative of the pressure on the wing surface. Results show that vortical structure evolution in the flow fields, which is described by the divergence of the convection term of the incompressible Navier–Stokes equations in a body-fixed reference frame, determines the time derivative of the surface pressure and effectively the far-field acoustics. It dominates over the centrifugal acceleration and Coriolis acceleration terms in determining the time derivative of the surface pressure. The position of the vortex is also found to affect the time derivative of the surface pressure. A scaling analysis reveals that the vortex acoustic source is scaled with the cube of the flapping frequency.
$M=0.04$) numbers is investigated. Based on the simplified model, the far-field acoustics is shown to be dominated by the time derivative of the pressure on the wing surface. Results show that vortical structure evolution in the flow fields, which is described by the divergence of the convection term of the incompressible Navier–Stokes equations in a body-fixed reference frame, determines the time derivative of the surface pressure and effectively the far-field acoustics. It dominates over the centrifugal acceleration and Coriolis acceleration terms in determining the time derivative of the surface pressure. The position of the vortex is also found to affect the time derivative of the surface pressure. A scaling analysis reveals that the vortex acoustic source is scaled with the cube of the flapping frequency.
Flow control of a low-aspect-ratio flat-plate heaving wing at an average angle of attack of  $10^{\circ }$ by a steady-blowing jet is numerically studied by using a feedback immersed boundary–lattice Boltzmann method. Blowing jets at the leading edge, mid-chord and trailing edge are considered. The wing enjoys the highest lift production with the trailing-edge downstream blowing jet, which improves the average lift by 50.0 % at
$10^{\circ }$ by a steady-blowing jet is numerically studied by using a feedback immersed boundary–lattice Boltzmann method. Blowing jets at the leading edge, mid-chord and trailing edge are considered. The wing enjoys the highest lift production with the trailing-edge downstream blowing jet, which improves the average lift by 50.0 % at  $Re = 1000$ and 22.9 % at
$Re = 1000$ and 22.9 % at  $Re = 5000$ through the enhancement of the tip vortex circulation caused by the increase in the mass flux of the shear layer at the wing tips. This increase in mass flux decreases as
$Re = 5000$ through the enhancement of the tip vortex circulation caused by the increase in the mass flux of the shear layer at the wing tips. This increase in mass flux decreases as  $Re$ increases from 1000 to 5000 due to its self-limiting mechanism. A mid-chord vertical blowing jet induces a middle vortex which enhances the lift production but the enhancement is smaller than that of trailing-edge downstream blowing jet. Other jet arrangements do not significantly increase the lift coefficient, but the mid-chord upstream blowing jet experiences a significant reduction in the drag coefficient, leading to an increase of 50.6 % in the average lift-to-drag ratio. The effectiveness of the flow control is not significantly affected by the aspect ratio.
$Re$ increases from 1000 to 5000 due to its self-limiting mechanism. A mid-chord vertical blowing jet induces a middle vortex which enhances the lift production but the enhancement is smaller than that of trailing-edge downstream blowing jet. Other jet arrangements do not significantly increase the lift coefficient, but the mid-chord upstream blowing jet experiences a significant reduction in the drag coefficient, leading to an increase of 50.6 % in the average lift-to-drag ratio. The effectiveness of the flow control is not significantly affected by the aspect ratio.
 $\boldsymbol{{n}}$ variance-premium reinsurers: from tree to chain
$\boldsymbol{{n}}$ variance-premium reinsurers: from tree to chain
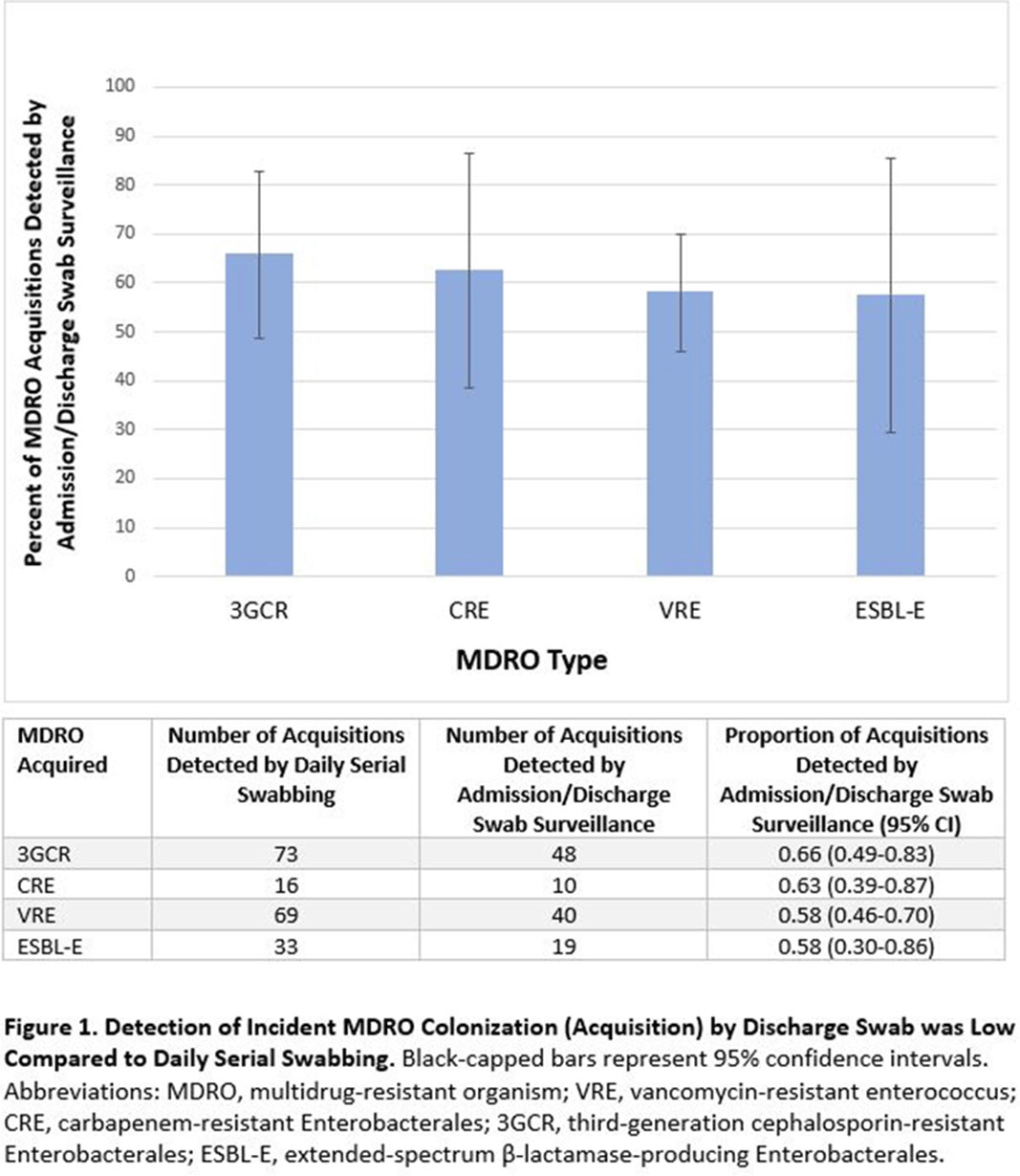
Background: Identification of hospitalized patients with enteric multidrug-resistant organism (MDRO) carriage, combined with implementation of targeted infection control interventions, may help reduce MDRO transmission. However, the optimal surveillance approach has not been defined. We sought to determine whether daily serial rectal surveillance for MDROs detects more incident cases (acquisition) of MDRO colonization in medical intensive care unit (MICU) patients than admission and discharge surveillance alone. Methods: Prospective longitudinal observational single-center study from January 11, 2017, to January 11, 2018. Inclusion criteria were ≥3 consecutive MICU days and ≥2 rectal or stool swabs per MICU admission. Daily rectal or stool swabs were collected from patients and cultured for MDROs, including vancomycin-resistant Enterococcus (VRE), carbapenem-resistant Enterobacterales (CRE), third-generation cephalosporin-resistant Enterobacterales (3GCR), and extended-spectrum β-lactamase–producing Enterobacterales (ESBL-E) (as a subset of 3GCR). MDRO detection at any time during the MICU stay was used to calculate prevalent colonization. Incident colonization (acquisition) was defined as new detection of an MDRO after at least 1 prior negative swab. We then determined the proportion of prevalent and incident cases detected by daily testing that were also detected when only first swabs (admission) and last swabs (discharge) were tested. Data were analyzed using SAS version 9.4 software. Results: In total, 939 MICU stays of 842 patients were analyzed. Patient characteristics were median age 64 years (interquartile range [IQR], 51–74), median MICU length of stay 5 days (IQR, 3–8), median number of samples per admission 3 (IQR, 2–5), and median Charlson index 4 (IQR, 2–7). Prevalent colonization with any MDRO was detected by daily swabbing in 401 stays (42.7%). Compared to daily serial swabbing, an admission- and discharge-only approach detected ≥86% of MDRO cases (ie, overall prevalent MDRO colonization). Detection of incident MDRO colonization by an admission- or discharge-only approach would have detected fewer cases than daily swabbing (Figure 1); ≥34% of total MDRO acquisitions would have been missed. Conclusions: Testing patients upon admission and discharge to an MICU may fail to detect MDRO acquisition in more than one-third of patients, thereby reducing the effectiveness of MDRO control programs that are targeted against known MDRO carriers. The poor performance of a single discharge swab may be due to intermittent or low-level MDRO shedding, inadequate sampling, or transient MDRO colonization. Additional research is needed to determine the optimal surveillance approach of enteric MDRO carriage.
Funding: No
Disclosures: None
Figure 1.