Refine search
Actions for selected content:
48204 results in Zoology

Fibre & fermented foods: differential effects on the microbiota-gut-brain axis
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 4 / December 2025
- Published online by Cambridge University Press:
- 25 October 2024, pp. 365-380
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Combined association between dietary antioxidant quality score and leisure-time physical activity on sleep pattern in cancer survivors: a cross-sectional study of National Health and Nutrition Examination Surveys database
-
- Journal:
- British Journal of Nutrition / Volume 133 / Issue 3 / 14 February 2025
- Published online by Cambridge University Press:
- 25 October 2024, pp. 334-345
- Print publication:
- 14 February 2025
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association between vegetable intake and major depressive disorder: results from National Health and Nutrition Examination Survey 2005–2018 and bidirectional two-sample Mendelian randomisation
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 24 October 2024, e220
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
How big is too big? A qualitative study of discretionary food portion size norms among Australian consumers
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 24 October 2024, e242
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Using spatial analysis to examine inequalities and temporal trends in food retail accessibility
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 24 October 2024, e222
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Response to: willingness v. ability to pay for a universal cost-shared school food programme in Canada
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 24 October 2024, e221
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
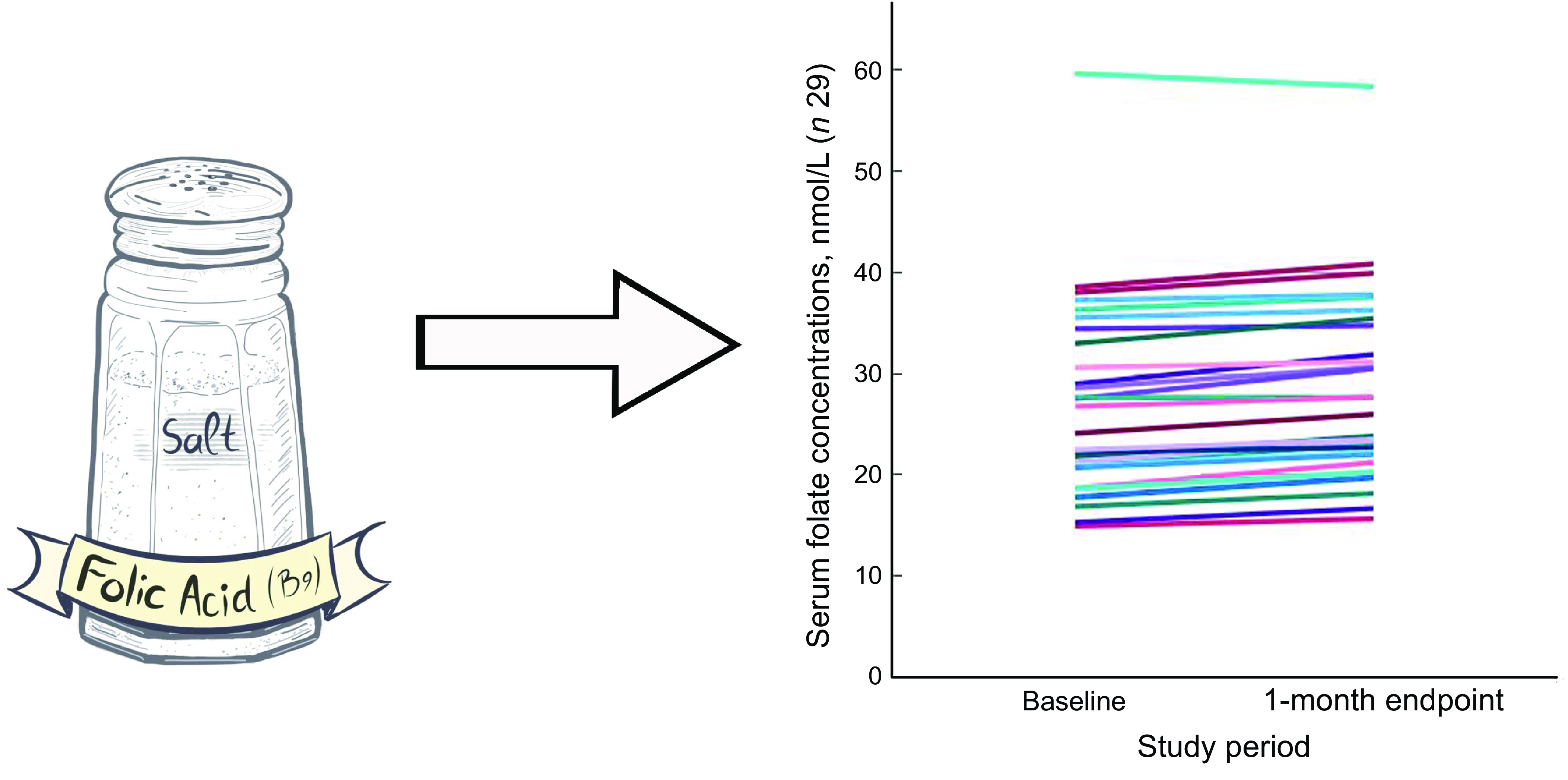
Improvement of serum folate status in the US women of reproductive age with fortified iodised salt with folic acid (FISFA study)
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 24 October 2024, e218
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Causal association of folic acid supplementary therapy and gastric ulcer: a Mendelian randomisation study
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 10 / 28 November 2024
- Published online by Cambridge University Press:
- 24 October 2024, pp. 1348-1355
- Print publication:
- 28 November 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Letter to the editor: willingness v. ability to pay for a universal cost-shared school food programme in Canada
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 24 October 2024, e219
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The promotion of ultra-processed foods in modern retail food outlets in rural and urban areas in Kenya
- Part of
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 24 October 2024, e240
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Yeast β-glucan supplementation lowers insulin resistance without altering microbiota composition compared with placebo in subjects with type II diabetes: a phase I exploratory study
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 9 / 14 November 2024
- Published online by Cambridge University Press:
- 23 October 2024, pp. 1161-1172
- Print publication:
- 14 November 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Carbohydrate intakes, food sources and tracking in Australian young children
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 8 / 28 October 2024
- Published online by Cambridge University Press:
- 23 October 2024, pp. 1073-1082
- Print publication:
- 28 October 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Salivary iodine concentrations can estimate iodine intake and diagnose abnormal thyroid function: a cross-sectional study in pregnant and lactating women in iodine-deficient areas
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 8 / 28 October 2024
- Published online by Cambridge University Press:
- 23 October 2024, pp. 1083-1092
- Print publication:
- 28 October 2024
-
- Article
-
- You have access
- HTML
- Export citation
PUFA and intrahepatic cholestasis of pregnancy: a two-sample Mendelian randomisation analysis
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 8 / 28 October 2024
- Published online by Cambridge University Press:
- 23 October 2024, pp. 1022-1029
- Print publication:
- 28 October 2024
-
- Article
-
- You have access
- HTML
- Export citation
Understanding consumer beliefs and choices related to food safety: a qualitative study in urban Ethiopia
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 23 October 2024, e239
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Folates, bacteria and ageing: insights from the model organism C. elegans in the study of nutrition and ageing
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 3 / September 2025
- Published online by Cambridge University Press:
- 23 October 2024, pp. 259-263
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring the interplay between emotional attitudes towards diabetes, eating behaviour and glycaemic control in patients with type 2 diabetes mellitus
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 23 October 2024, e237
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Conference on ‘nutrition and wellbeing in Oceania’
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 2 / May 2025
- Published online by Cambridge University Press:
- 22 October 2024, pp. 125-128
-
- Article
-
- You have access
- HTML
- Export citation
Food acquisition and consumption by NOVA food classification and lived poverty index among rural and urban households in South Africa and Ghana
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 22 October 2024, e260
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
M-SAKHI – Mobile health solutions to help community providers promote maternal and infant nutrition and health: a description of development of the Program Impact Pathway using Theory of Change
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 22 October 2024, e217
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
