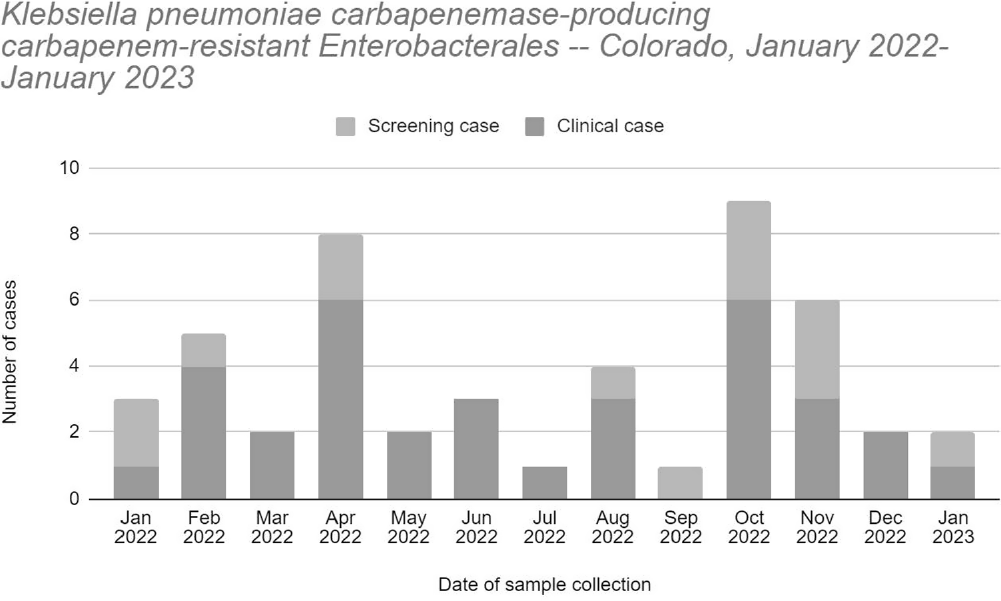
Background: The Colorado Department of Public Health and Environment (CDPHE) detected an increase in Klebsiella pneumoniae carbapenemase-producing carbapenem-resistant Enterobacterales (KPC-CRE) infections in October 2022. We investigated patient epidemiological links and isolate relatedness to characterize interfacility transmission of KPC-CRE in the Denver metro area and inform regional prevention strategies. Methods: We defined a case as polymerase chain reaction detection of KPC from clinical or screening specimens collected during January 2022 – January 2023. Cases were identified through statewide CRE surveillance and carbapenemase testing at the CDPHE laboratory and counted once within a 30-day period. Medical records were reviewed to identify healthcare facility admissions and patient facility overlap in the 12 months prior to sample collection. Whole genome sequencing (WGS) was performed for 34 patients with available KPC-CRE isolates using short- and long-read sequencing techniques. We performed multi-locus sequence typing, generated genome phylogenetic trees, and compared plasmid contig sequences to identify relatedness between KPC-CRE isolates. Clusters were defined as ≥2 genetically related isolates of the same organism or carbapenemase plasmid, from different patients. Results: We identified 48 cases (34 clinical and 14 screening) among 39 patients (figure). Patients had a mean age of 52 years (range 16-86) and median of three healthcare facility admissions (range 1-14). Twenty-eight patients (72%) were male. We identified 16 (41%) patients with epidemiological links to one acute care hospital (ACH), 11 (28.2%) patients to one long-term acute care hospital (LTACH), and four (10.2%) patients to each of two ventilator-capable skilled nursing facilities (vSNF). Five distinct clusters of KPC-CRE were identified by WGS among 23 patients (E. hormaechei, two distinct E. cloacae clusters, K. pneumoniae, and K. oxytoca) with linkages to ten healthcare facilities, including two vSNFs, two LTACHs, and six ACHs. Three distinct KPC genes were identified among the clusters: KPC-2, KPC-3, and KPC-4. Genomes assembled from long reads identified identical or similar KPC-gene-containing plasmids across different species or sequence types, suggesting horizontal gene transfer of KPC. Conclusions: Multiple KPC-CRE strains co-circulated and were associated with patient movement between acute and post-acute care settings. WGS allowed us to identify multi-facility clusters. Time and location of carbapenemase acquisition were challenging to determine for genetically related isolates when epidemiologic links could not be determined from medical records. This could be due to undetected cases. We notified healthcare facilities of their shared transmission risk and advocated for improved attention to infection control, carbapenemase screening, and communication upon patient transfer.
Background: During 2021–2023, an increase in Klebsiella pneumoniae carbapenemase producing Enterobacterales species (KPC-CRE) cases occurred among patients admitted to several overlapping healthcare facilities, prompting an investigation by the Colorado Department of Public Health and Environment (CDPHE). We applied social network analysis (SNA) to identify KPC-CRE networks and other multidrug-resistant organism (MDRO) transmission, created a tool for public health prevention planning and for facilities to examine their own patient transfer connectivity, and explored additional public health and emergency preparedness applications. Methods: A statewide patient transfer network was created using 2021–2022 Medicare beneficiary data. Sub-networks were isolated from the larger network to examine a cluster of facilities involved in a KPC-CRE outbreak, defined as ≥2 KPC-CRE cases related by whole genome sequencing (WGS). WGS was conducted at the CDPHE State Lab. Highly connected facilities were determined by patient transfers between at least two KPC-CRE testing facilities. Individual patient journeys were constructed using admissions and culture date. SNA was conducted in RStudio; visualizations, network metric calculations, and clustering analysis were conducted using Gephi and ArcGIS software. Results: SNA yielded 4,864 direct patient transfers between 326 healthcare facilities (220 skilled nursing facilities, 50 acute care hospitals, 32 critical access hospitals, six long term acute care hospitals, and 18 facilities not previously classified; Figure 1). WGS identified five separate KPC-CRE outbreaks among 14 patients during February 2022–January 2023; 14 patient specimens were collected at four testing facilities. We identified five highly connected facilities in addition to the four testing facilities. Patient journeys allowed us to identify possible locations of KPC-CRE transmission in four of the five outbreaks (Figure 2). CDPHE provided guidance to all involved facilities on admission screening, routine point prevalence surveys, and interfacility communication as part of an MDRO prevention plan. CDPHE then developed the transfer network into an interactive ArcGIS dashboard enabling facilities to examine their own patient transfer patterns. Conclusions: SNA enabled CDPHE to identify at-risk facilities for KPC-CRE transmission and create an interactive tool for facility and public health use. Future applications of patient transfer networks can include geographical grouping of facilities based on transfers to zone healthcare coalitions and conduct preparedness activities, and creating medical operations preparedness plans for emergencies or disasters.



