
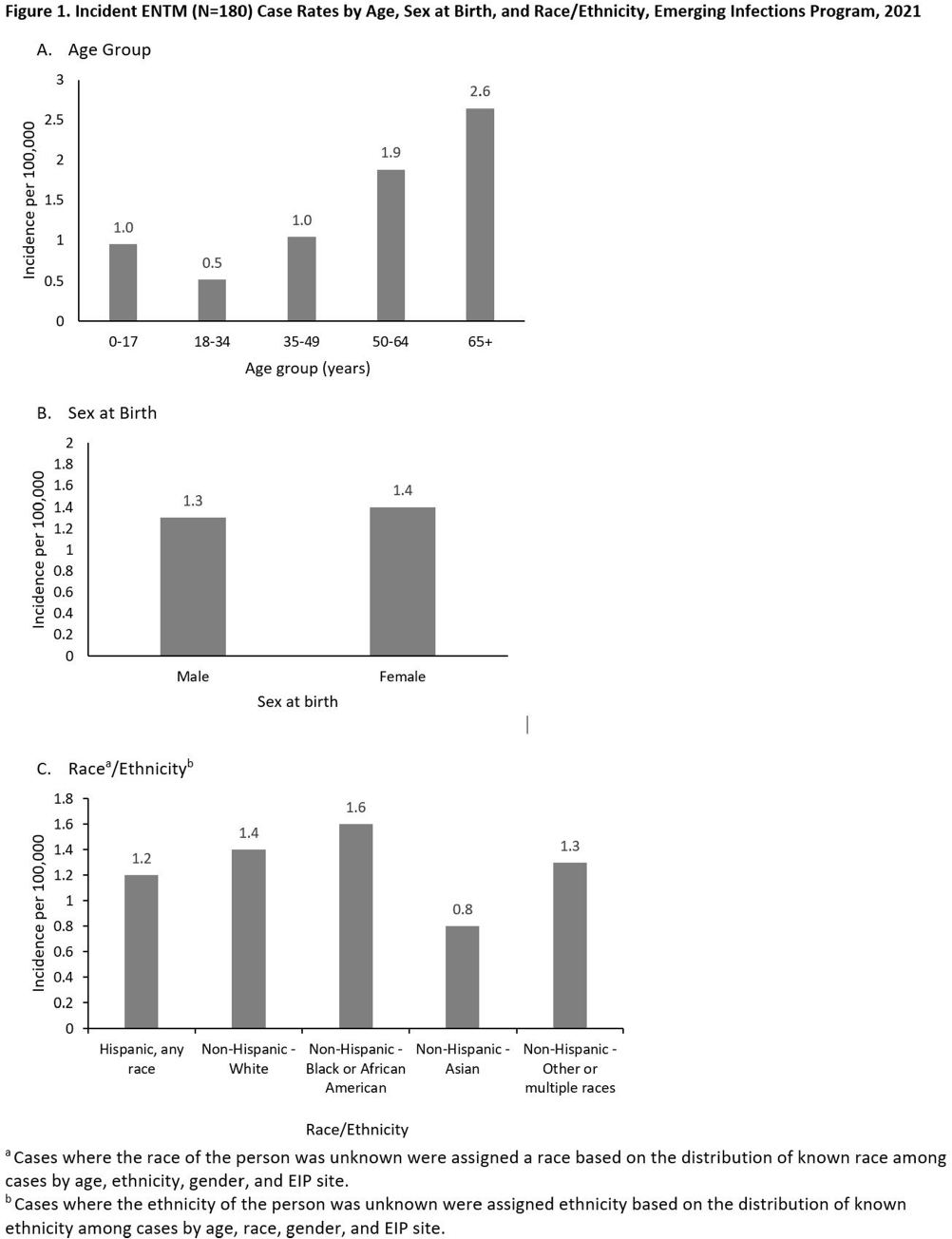
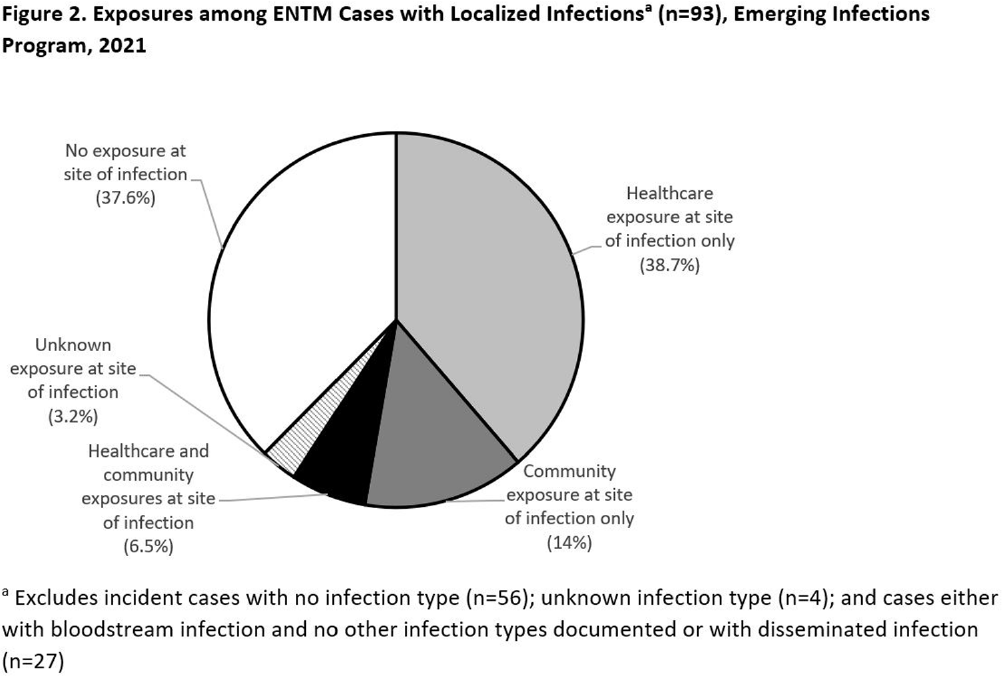
Background: Extrapulmonary nontuberculous mycobacteria (ENTM) infections are difficult to treat and often require prolonged therapy or surgery. Few population-based studies describe ENTM epidemiology, though well-known healthcare-associated outbreaks have occurred. Using the first year of multi-site ENTM surveillance, we characterized rates and how frequently ENTM infections may be related to healthcare. Methods: CDC’s Emerging Infections Program conducted active, laboratory- and population-based surveillance for ENTM cases in 4 sites (Colorado [5 counties], Minnesota [statewide], New York [1 county], and Oregon [statewide]) in 2021. An incident ENTM case was NTM isolation from a non-pulmonary specimen, excluding stool or rectal swabs, in a resident of the surveillance area without either medical record documentation of prior ENTM infection or isolation of ENTM in the prior 12 months. Demographic, clinical, information on selected healthcare and community exposures, and laboratory data were collected via medical record review. We calculated incidence per 100,000 population using U.S. Census population estimates and performed descriptive analyses. Results: A total of 180 incident ENTM cases were reported in 2021. The crude annual incidence rate was 1.3 per 100,000 persons. Incidence increased with age (from 0.95 per 100,000 among 0–17 year-olds to 2.65 per 100,000 among persons ≥65), ranged from 0.8 among non-Hispanic Asian persons to 1.6 per 100,000 in non-Hispanic Black persons, and was similar among males (1.3 per 100,000) and females (1.4 per 100,000; Figure 1). Mycobacterium avium complex (64 [35.6%]) was the most frequently isolated species group, followed by Mycobacterium chelonae complex (31 [17.2%]). Skin and soft tissue infections were the most frequent infection type (37 [20.6%]); 27 cases (15.0%) were associated with disseminated and/or only bloodstream infection, and 56 cases (31.1%) had no infection type documented. Among 93 cases with localized ENTM infections (i.e., infections that were not disseminated and/or only bloodstream infections), 38.7% had only healthcare-related exposures, 14% had only community-related exposures and 6.5% had both exposure types at the site of infection (Figure 2). Healthcare-related exposures at the infection site included surgery (23.7%), injection/infusion (21.5%), and medical devices (18.3%). The most frequent community-related exposure at the infection site was trauma (17.2%). Only one case was part of a known outbreak, which was healthcare-associated. Conclusions: ENTM infections are relatively rare, but nearly half of patients with localized ENTM infections had prior healthcare-related exposures. This indicates that the burden of ENTM infections related to healthcare may be much larger than what has been suggested from reported outbreaks.
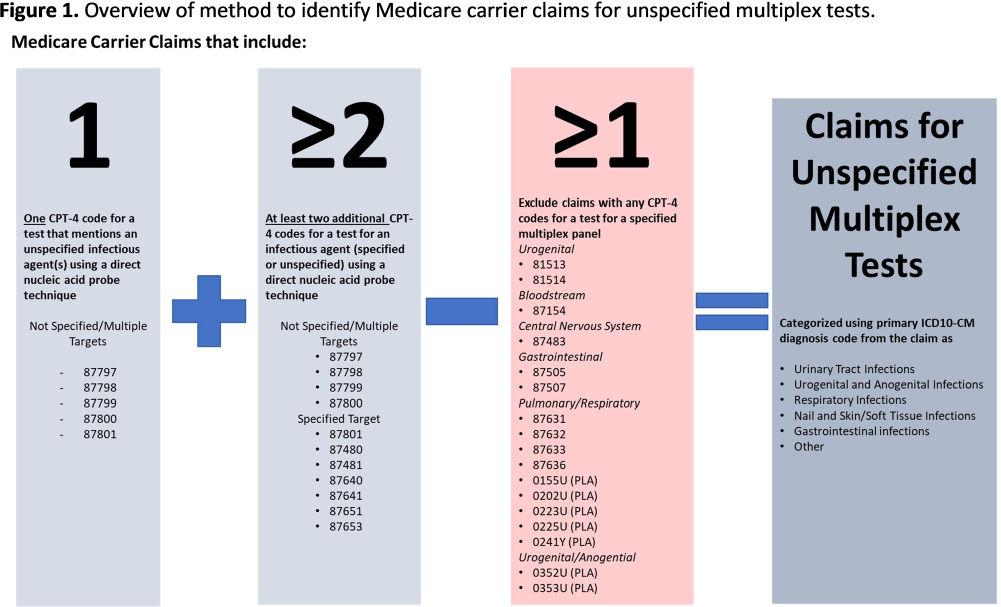
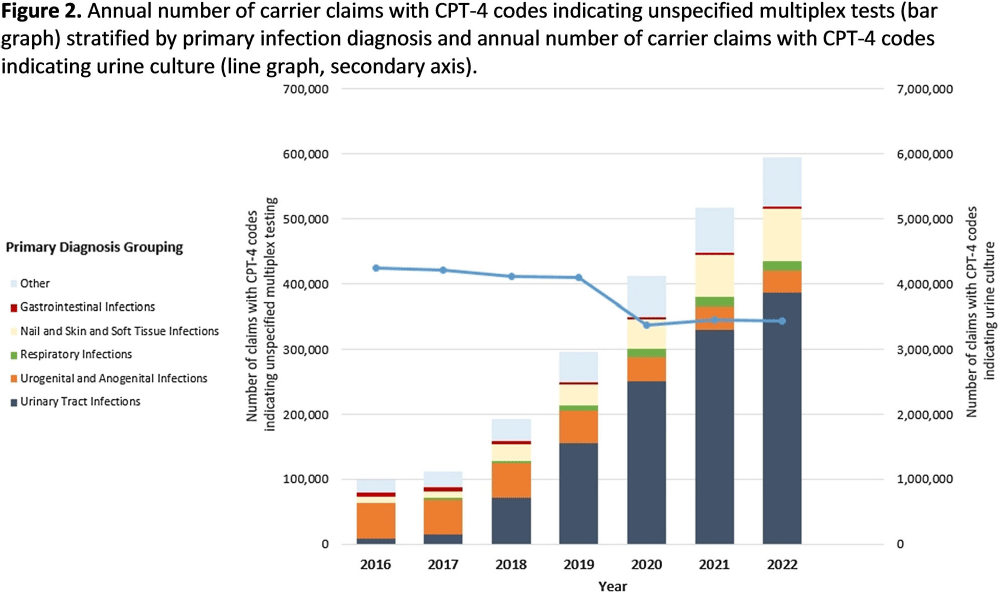
Background: Multiplex molecular tests for infectious diseases can provide highly sensitive results rapidly; however, these tests may more readily detect asymptomatic colonization. There are reports of non-FDA approved laboratory-developed multiplex tests for the diagnosis of urinary tract infections (UTI). Differentiating UTI from asymptomatic bacteriuria is challenging, especially in older adults. The increased sensitivity of multiplex tests may exacerbate this challenge. We sought to describe the use of multiplex testing for UTIs in Medicare claims. Methods: Multiplex testing was identified using carrier claims submitted by non-institutional providers using the Chronic Conditions Warehouse for 2016 – 2022. Because there are no CPT-4 codes specifying UTI multiplex testing, we included claims as described in Figure 1 and categorized claims based on the primary ICD-10-CM diagnosis. The payment amounts for line items related to testing for infectious agents were summed. Laboratories were counted using CLIA numbers listed on corresponding claims. Beneficiaries residing in a nursing home at the time of their claim were identified using stay information derived from the Minimum Dataset 3.0. For comparison, similar characteristics among carrier claims with a CPT-4 code indicating urine culture were also described. Results: Claims for unspecified multiplex molecular tests overall have increased, driven by increases in claims with a primary UTI diagnosis (from 8,521 in 2016 to 386,943 in 2022), while urine cultures have not (Figure 1). In 2022, 65% of all unspecified multiplex tests were linked to a diagnosis of UTI; UTI multiplex claims were associated with 647 laboratories. For UTI claims, the median cost per claim for line items related to multiplex testing was $589 compared to $13 for urine culture-related line items. Overall, 8% of UTI multiplex claims were for beneficiaries residing in a nursing home. Conclusions: Claims for non-FDA approved unspecified multiplex tests associated with a primary diagnosis of UTI have increased >45-times between 2016-2021 and have >45-times higher median costs than urine cultures. The use of this testing in the Medicare population, including nursing home residents, is of potential concern given that inappropriate treatment of asymptomatic bacteriuria has been described to be common in older adults. Research is needed to outline use cases where UTI multiplex testing may be beneficial. Appropriate use of diagnostic testing is important to minimize diagnostic errors and avoid unnecessary antibiotic use.
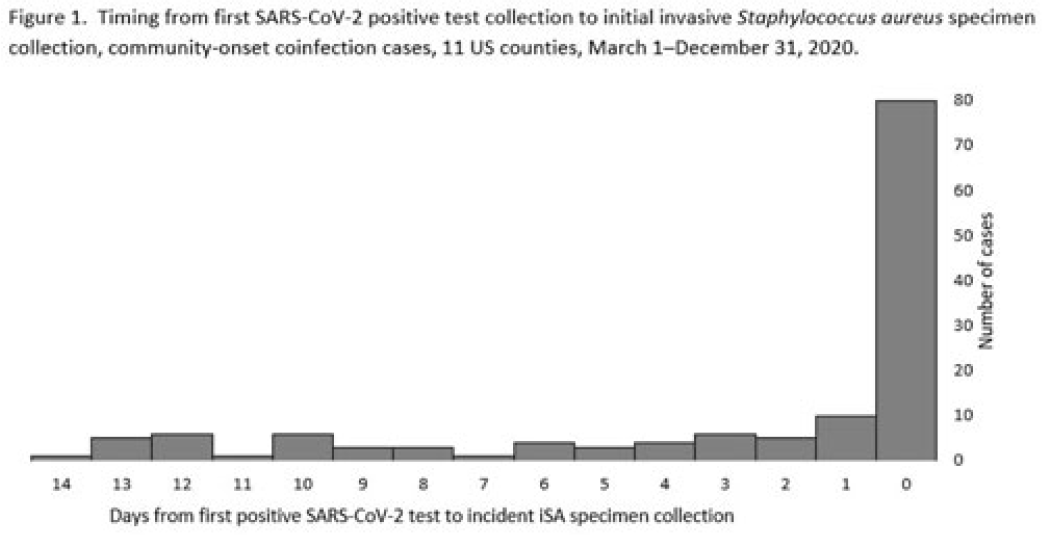
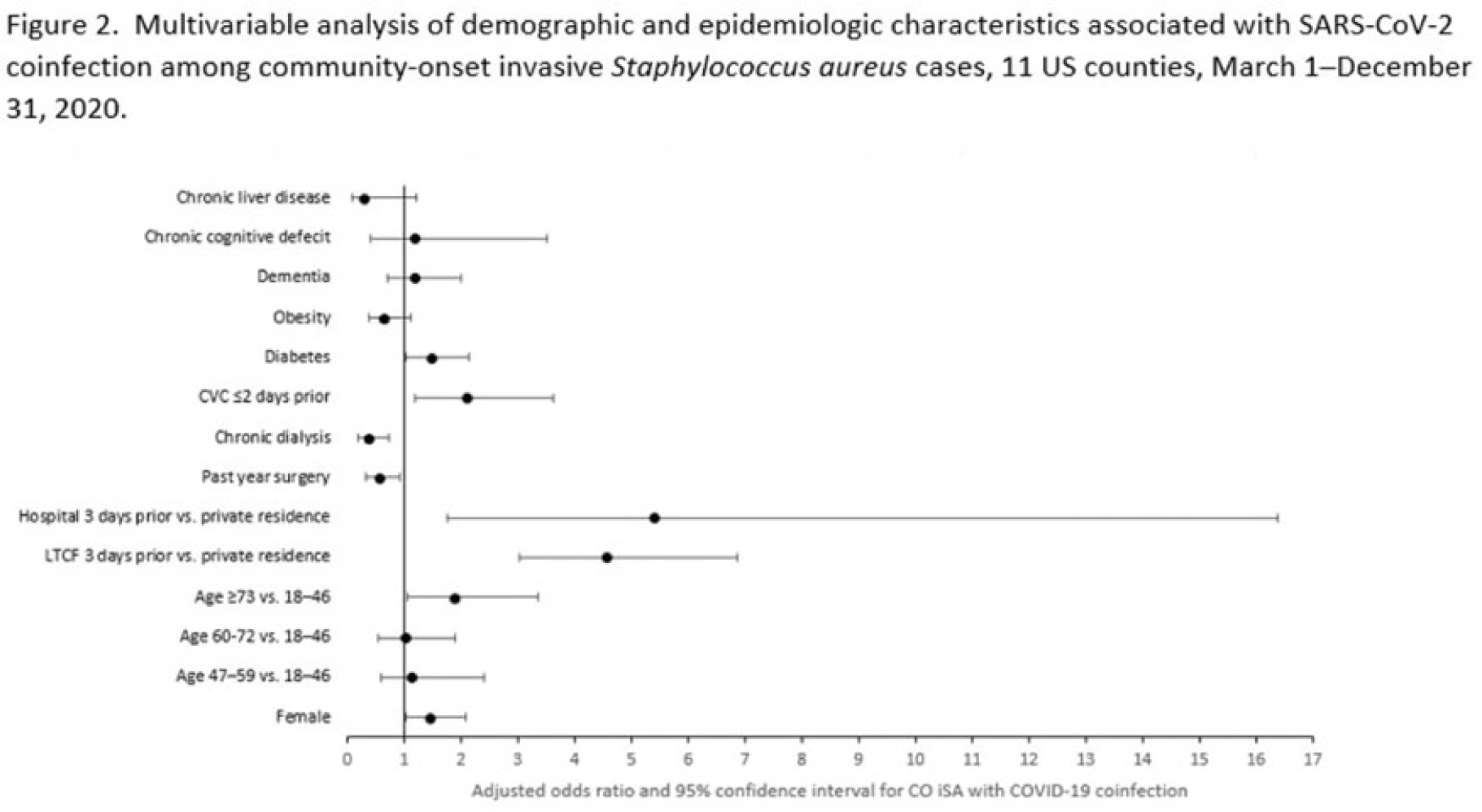
Background: Previous analyses describing the relationship between SARS-CoV-2 infection and Staphylococcus aureus have focused on hospital-onset S. aureus infections occurring during COVID-19 hospitalizations. Because most invasive S. aureus (iSA) infections are community-onset (CO), we characterized CO iSA cases with a recent positive SARS-CoV-2 test (coinfection). Methods: We analyzed CDC Emerging Infections Program active, population- and laboratory-based iSA surveillance data among adults during March 1–December 31, 2020, from 11 counties in 7 states. The iSA cases (S. aureus isolation from a normally sterile site in a surveillance area resident) were considered CO if culture was obtained <3 days after hospital admission. Coinfection was defined as first positive SARS-CoV-2 test ≤14 days before the initial iSA culture. We explored factors independently associated with SARS-CoV-2 coinfection versus no prior positive SARS-CoV-2 test among CO iSA cases through a multivariable logistic regression model (using demographic, healthcare exposure, and underlying condition variables with P<0.25 in univariate analysis) and examined differences in outcomes through descriptive analysis. Results: Overall, 3,908 CO iSA cases were reported, including 138 SARS-CoV-2 coinfections (3.5%); 58.0% of coinfections had iSA culture and the first positive SARS-CoV-2 test on the same day (Fig. 1). In univariate analysis, neither methicillin resistance (44.2% with coinfection vs 36.5% without; P = .06) nor race and ethnicity differed significantly between iSA cases with and without SARS-CoV-2 coinfection (P = .93 for any association between race and ethnicity and coinfection), although iSA cases with coinfection were older (median age, 72 vs 60 years , P<0.01) and more often female (46.7% vs 36.3%, P=0.01). In multivariable analysis, significant associations with SARS-CoV-2 coinfection included older age, female sex, previous location in a long-term care facility (LTCF) or hospital, presence of a central venous catheter (CVC), and diabetes (Figure 2). Two-thirds of co-infection cases had ≥1 of the following characteristics: age > 73 years, LTCF residence 3 days before iSA culture, and/or CVC present any time during the 2 days before iSA culture. More often, iSA cases with SARS-CoV-2 coinfection were admitted to the intensive care unit ≤2 days after iSA culture (37.7% vs 23.3%, P<0.01) and died (33.3% vs 11.3%, P<0.01). Conclusions: CO iSA patients with SARS-CoV-2 coinfection represent a small proportion of CO iSA cases and mostly involve a limited number of factors related to likelihood of acquiring SARS-CoV-2 and iSA. Although CO iSA patients with SARS-CoV-2 coinfection had more severe outcomes, additional research is needed to understand how much of this difference is related to differences in patient characteristics.
Disclosures: None

