Diabetes mellitus is reaching epidemic proportions globally and is associated with a number of long-term central nervous system complications in older diabetic adults which are potentially modifiable. Improving diabetic brain health literacy among the public, diabetic individuals and healthcare staff has the potential to reduce the incidence of such complications as depression, cognitive impairment and dementia, leading to healthier ageing.
To establish diabetic brain health literacy levels among the general public, healthcare professionals and diabetic outpatient attendees using a knowledge questionnaire.
A self-administered questionnaire was made available to the public for completion via an Irish website. An adapted questionnaire was disseminated among medicine for the elderly nursing staff and diabetes outpatient attendees in a large urban teaching hospital in Dublin, Ireland. Questions assessed knowledge of potential brain health diabetic complications and garnered pertinent demographic information.
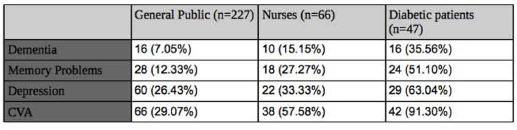
Graph 1- Knowledge of potential brain health complications of diabetes.
Graph 2 – Knowledge of potential non-central nervous system complications of diabetes
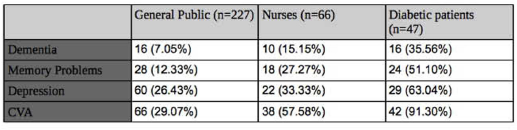
This study demonstrates poor knowledge among the public of the increased risk of brain health complications in older diabetic adults. Nursing staff members had greater knowledge and diabetic patients had the greatest, but less than satisfactory knowledge. This contrasts with greater awareness of non-brain diabetic complications such as eye disease and neuropathy among all three groups. Results suggest a need for expansion of health literacy campaigns to promote awareness, and to highlight potentially modifiable risk factors to aid in disease prevention, control and prevention of brain health complications.

