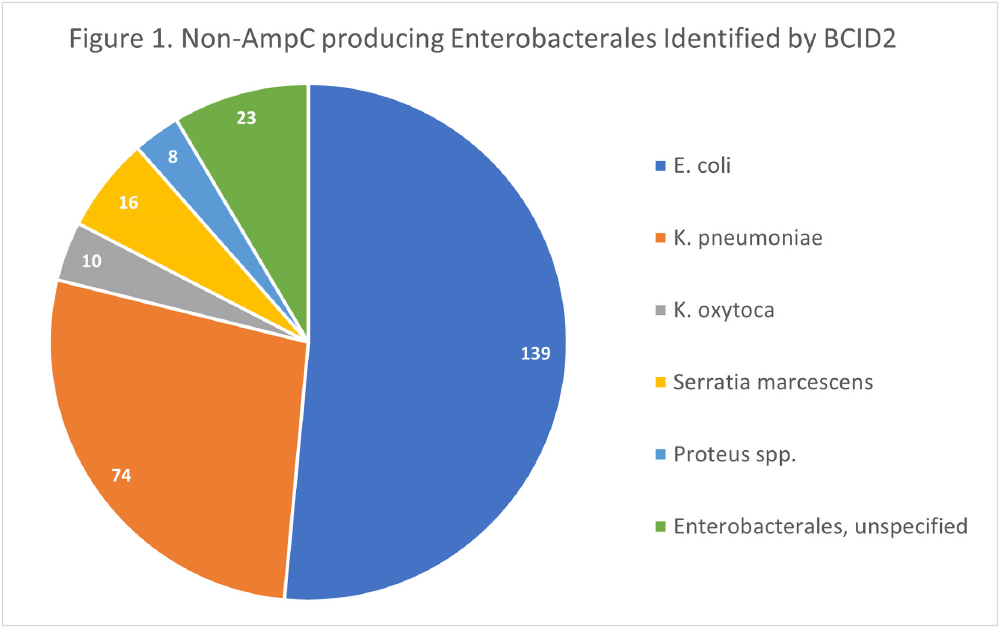
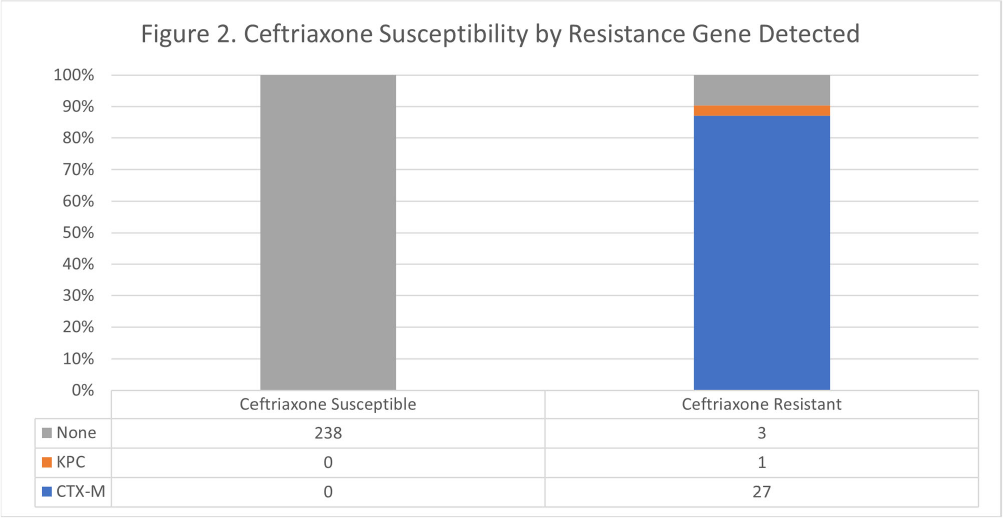
Background: The BioFire FilmArray Blood Culture Identification 2 (BCID2) Panel is used to identify organisms present in positive blood cultures within hours of detection at Virginia Commonwealth University Health System (VCUHS). BCID2 is also able to detect common resistance mechanisms including CTX-M, the most common extended-spectrum beta-lactamase (ESBL) in the United States, and several carbapenemases. The Antimicrobial Stewardship Program (ASP) at VCUHS established optimal treatment recommendations for each organism identified by BCID2 based on the detection of a resistance mechanism and local resistance patterns. The recommendation for the majority of Enterobacterales without a detected resistance mechanism is ceftriaxone. However, providers are often reluctant to de-escalate antibiotics without confirmed susceptibility testing, as there may be other mechanisms of antibiotic resistance in Gram-negative organisms. The objective of this evaluation was to measure the degree of congruence between BCID2 resistance mechanism detection and susceptibility testing by disk diffusion, and to validate the adequacy of the VCUHS ASP BCID2 treatment recommendations for Enterobacterales bacteremia. Methods: Patients with positive Enterobacterales BCID2 results from March 12 to June 19, 2023 were retrospectively identified. Organisms identified by BCID2 that were considered high-risk for clinically significant AmpC production due to an inducible AmpC gene (i.e., K. aerogenes, E. cloacae complex) were excluded. Results: A total of 270 results were included. The most commonly identified organism was E. coli (n = 139, 51.5%), followed by K. pneumoniae (n = 74, 27.4%). There were 27 (10%) isolates positive for CTX-M and 1 (0.4%) isolate positive for KPC. All CTX-M isolates were ceftriaxone resistant, and the KPC isolate was meropenem resistant. The remaining 242 isolates were negative for all resistance markers detected by BCID2. Of these, only 3 (1.2%) were resistant to ceftriaxone and notably, 8 (3.3%) were resistant to piperacillin/tazobactam. Overall, BCID2 CTX-M detection was 90% sensitive and 100% specific for predicting ceftriaxone resistance in Enterobacterales. Conclusion: CTX-M detection by BCID2 is highly sensitive and specific for predicting ceftriaxone resistance in Enterobacterales. CTX-M negative isolates were more often susceptible to ceftriaxone than to piperacillin/tazobactam, which is commonly used as empiric therapy for Gram-negative organisms at our institution. This highlights an excellent opportunity for safe and effective early de-escalation of antibiotics for treatment of Enterobacterales bacteremia.
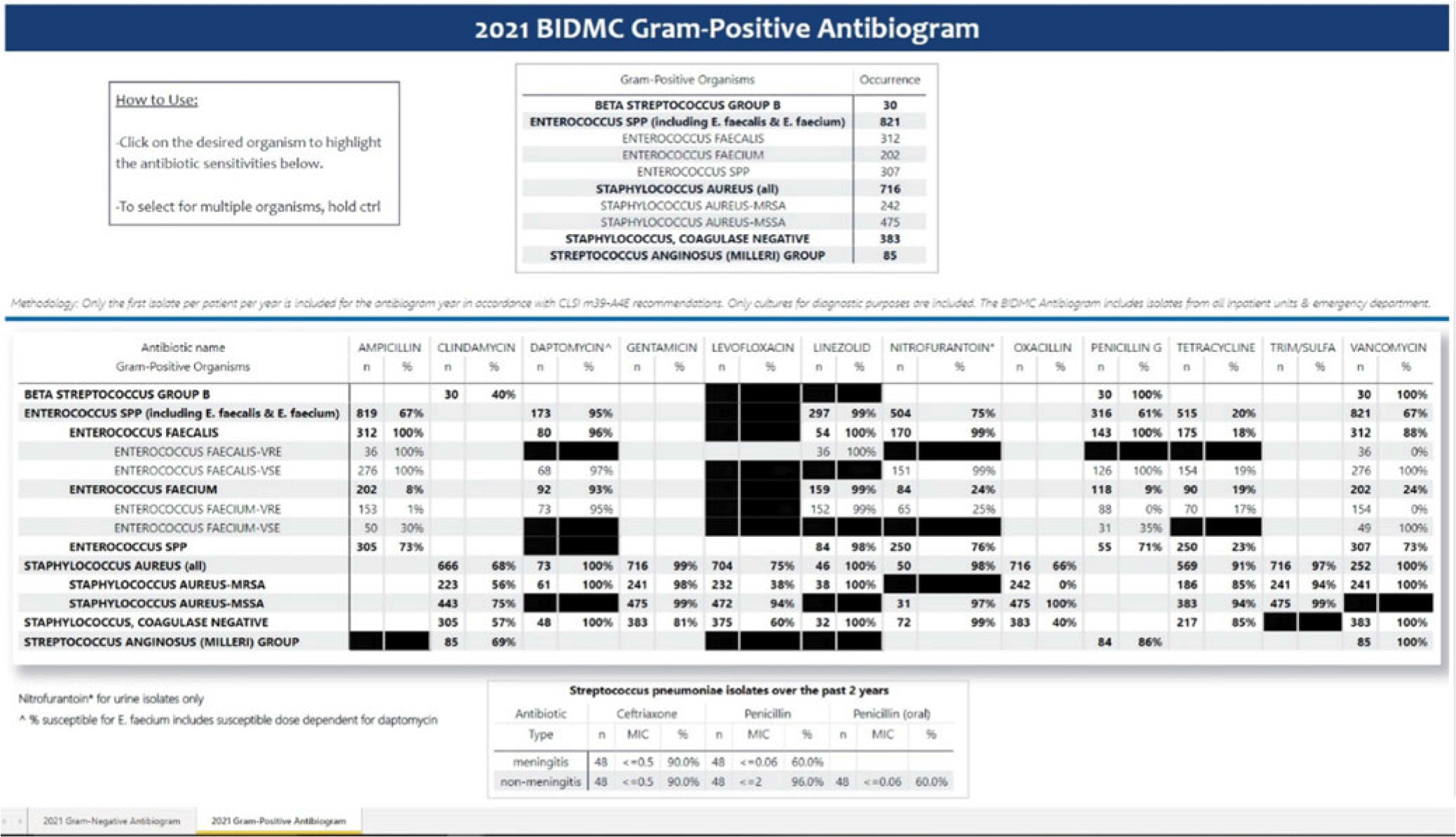
Background: Previously, our hospital manually built a static antibiogram from a surveillance system (VigiLanz) culture report. In 2019, a collaboration between the antimicrobial stewardship team (AST) and the infection control (IC) team set out to leverage data automation to create a dynamic antibiogram. The goal for the antibiogram was the ability to easily distribute and update for hospital staff, with the added ability to perform advanced tracking and surveillance of organism and drug susceptibilities for AST and IC. By having a readily available, accurate, and Clinical and Laboratory Standards Institute (CLSI)–compliant antibiogram, clinicians have the best available data on which to base their empiric antibiotic decisions. Methods: First, assessment of required access to hospital databases and selection of a visualization software (MS Power BI) was performed. Connecting SQL database feeds to Power BI enabled creation of a data model using DAX and M code to comply with the CLSI, generating the first isolate per patient per year. Once a visual antibiogram was created, it was validated against compiled antibiograms using data from the microbiology laboratory middleware (bioMerieux, Observa Integrated Data Management Software). This validation process uncovered some discrepancies between the 2 reference reports due to cascade reporting of susceptibilities. The Observa-derived data were used as the source of truth. The antibiogram prototype was presented to AST/IC members, microbiology laboratory leadership, and other stakeholders to assess functionality. Results: Following feedback and revisions by stakeholders, the new antibiogram was published on a hospital-wide digital platform (Fig. 1). Clinicians may view the antibiogram at any time on desktops from a firewall (or password)–protected intranet. The antibiogram view defaults to the current calendar year and users may interact with the antibiogram rows and columns without disrupting the integrity of the background databases or codes. Each year, simple refreshing of the Power BI antibiogram and changing of the calendar year allows us to easily and accurately update the antibiogram on the hospital-wide digital platform. Conclusions: This interdisciplinary collaboration resulted in a new dynamic, CLSI-compliant antibiogram with improved usability, increased visibility, and straightforward updating. In the future, a mobile version of the antibiogram may further enhance accessibility, bring more useful information to providers, and optimize AST/IC guidelines and education.
Disclosures: None

