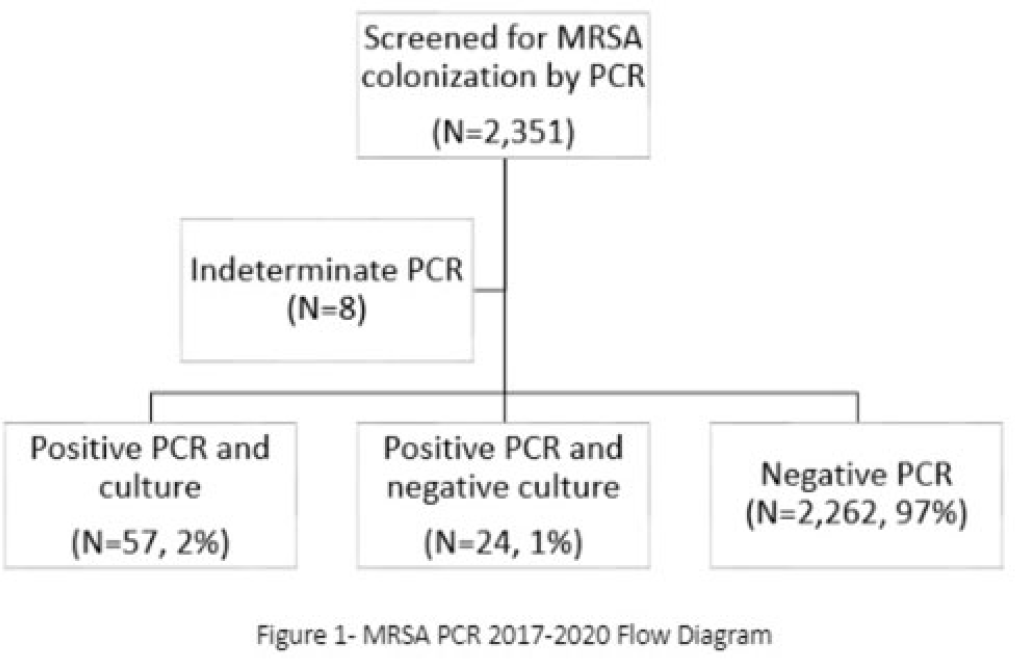
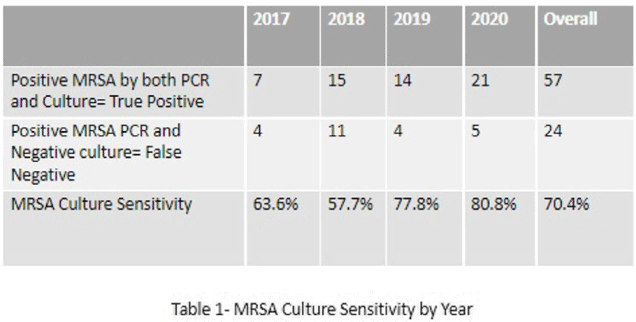
Background: Neonates colonized with methicillin-resistant Staphylococcus aureus (MRSA) are at high risk of developing life-threatening MRSA infection. Due to lack of evidence, national guidelines do not currently recommend a specific methodology for detecting MRSA colonization. We hypothesize that surveillance for MRSA colonization via polymerase chain reaction (PCR) is superior to culture for the detection of colonization. Methods: In this retrospective study, we compared results of MRSA surveillance by 2 methodologies, culture and PCR, after implementation of an MRSA surveillance and decolonization protocol in the Texas Children’s Hospital Pavilion for Women, a 42-bed neonatal intensive care unit. MRSA colonization of 3 body sites via the 2 methodologies was assessed from June 2017 through December 2020. All neonates were screened for MRSA upon admission to the NICU and weekly thereafter until MRSA-positive or discharged. Swab specimens were initially tested by PCR (Xpert MRSA NxG, Cepheid) and when MRSA-positive reflexed to culture to recover the organism for further characterization. This study was approved through the Baylor College of Medicine Institutional Review Board. Results: During the study period, 2,351 neonates were assessed for MRSA colonization by PCR; 81 (3.4%) infants were PCR positive (Fig. 1). Of those 81, 57 (70.4%) had concordant MRSA PCR and culture results, and 24 (29.6%) were MRSA PCR positive but no isolate was recovered in culture. Also, 8 specimens were indeterminate by PCR. However, 1 infant who was negative by culture but was PCR positive developed an MRSA orbital infection. Compared to PCR, the overall sensitivity of MRSA culture was 70.4% (range, 57.7%–80.8%, depending on the year) (Table 1). Conclusions: PCR is more sensitive than culture for detecting MRSA colonization in neonates. Utilizing a PCR method enhances the ability to identify MRSA colonized infants more readily and allows for prompt initiation of infection control interventions including isolation precautions and decolonization strategies. Reflex to culture remains important for strain characterization during outbreak investigations and for additional susceptibility testing. Resource utilization and cost–benefit analyses should be done in future studies to influence changes in national guidelines for the control of Staphylococcus aureus colonization and infection in neonatal intensive care units.
Disclosures: None
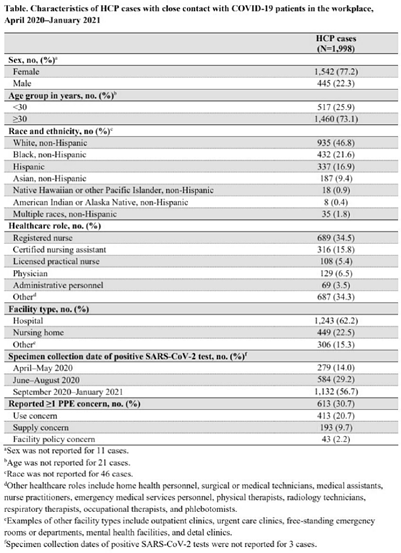
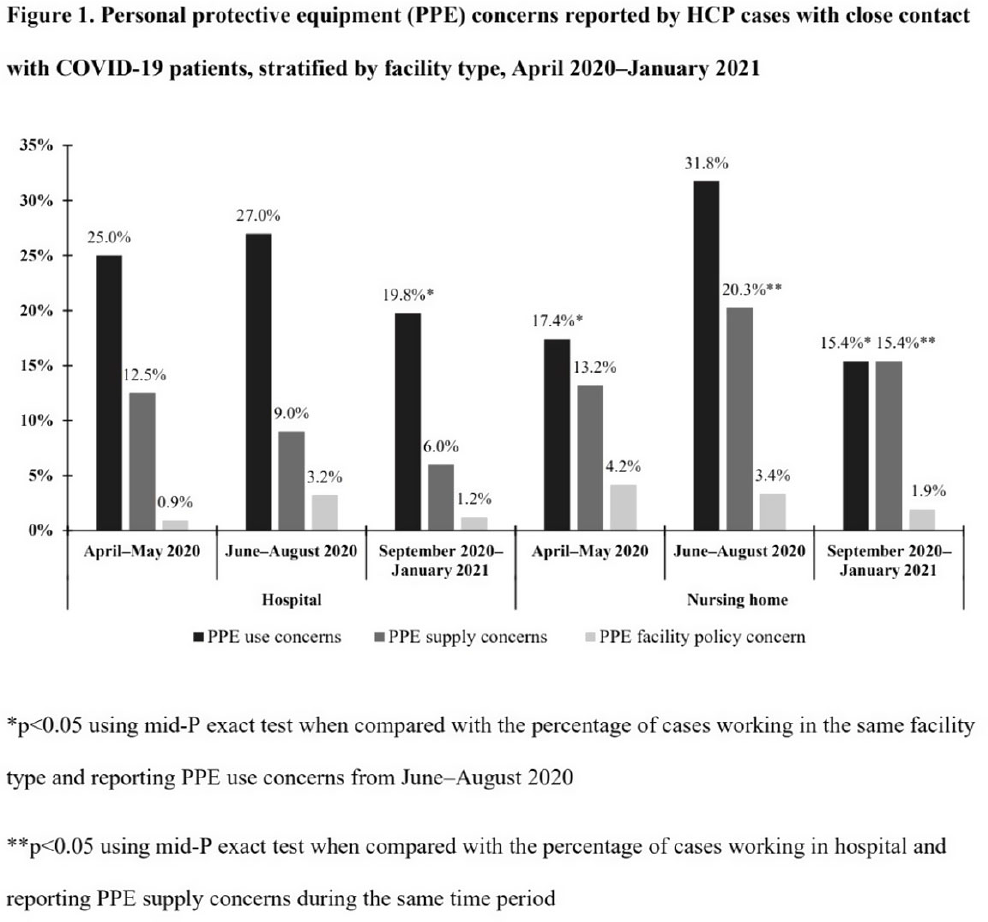
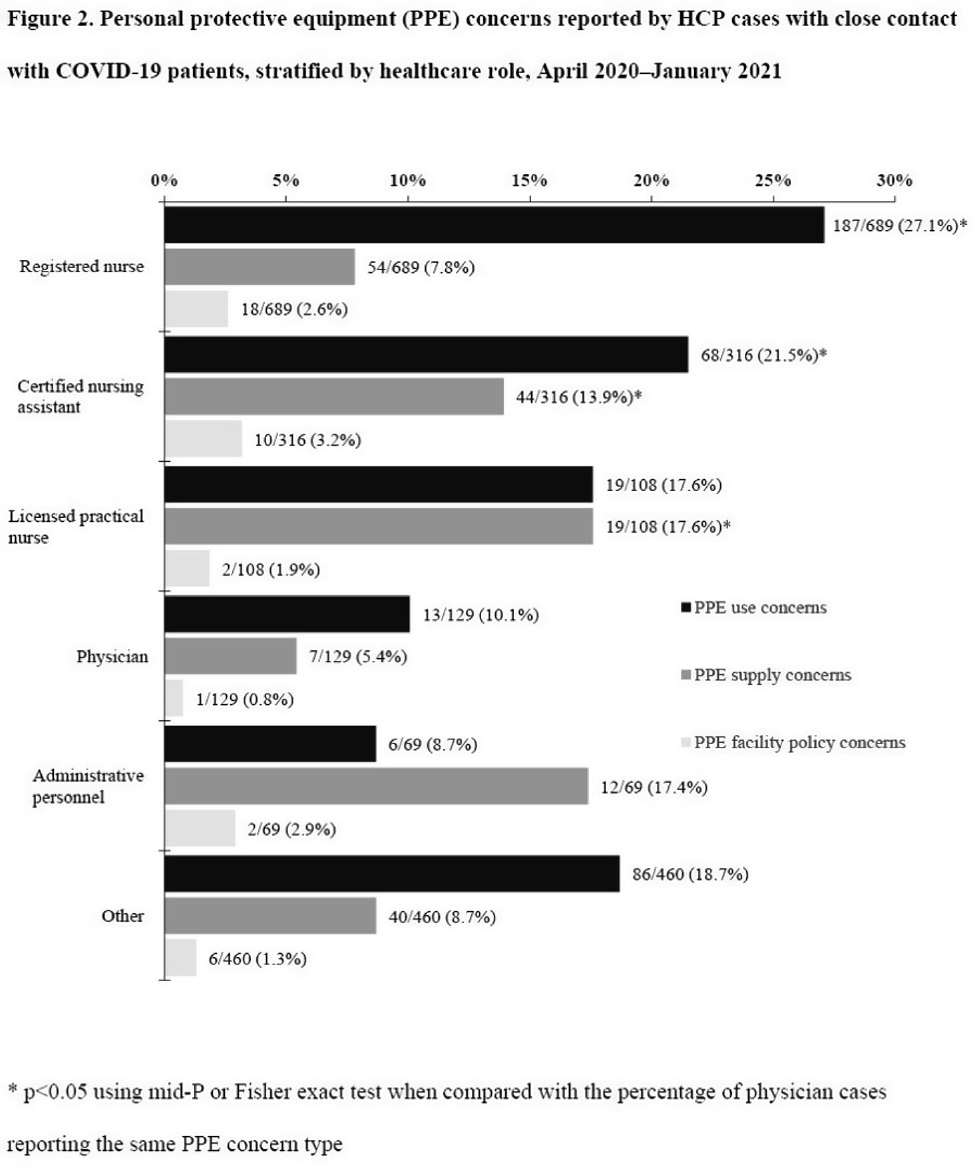
Background: Healthcare facilities have experienced many challenges during the COVID-19 pandemic, including limited personal protective equipment (PPE) supplies. Healthcare personnel (HCP) rely on PPE, vaccines, and other infection control measures to prevent SARS-CoV-2 infections. We describe PPE concerns reported by HCP who had close contact with COVID-19 patients in the workplace and tested positive for SARS-CoV-2. Method: The CDC collaborated with Emerging Infections Program (EIP) sites in 10 states to conduct surveillance for SARS-CoV-2 infections in HCP. EIP staff interviewed HCP with positive SARS-CoV-2 viral tests (ie, cases) to collect data on demographics, healthcare roles, exposures, PPE use, and concerns about their PPE use during COVID-19 patient care in the 14 days before the HCP’s SARS-CoV-2 positive test. PPE concerns were qualitatively coded as being related to supply (eg, low quality, shortages); use (eg, extended use, reuse, lack of fit test); or facility policy (eg, lack of guidance). We calculated and compared the percentages of cases reporting each concern type during the initial phase of the pandemic (April–May 2020), during the first US peak of daily COVID-19 cases (June–August 2020), and during the second US peak (September 2020–January 2021). We compared percentages using mid-P or Fisher exact tests (α = 0.05). Results: Among 1,998 HCP cases occurring during April 2020–January 2021 who had close contact with COVID-19 patients, 613 (30.7%) reported ≥1 PPE concern (Table 1). The percentage of cases reporting supply or use concerns was higher during the first peak period than the second peak period (supply concerns: 12.5% vs 7.5%; use concerns: 25.5% vs 18.2%; p Conclusions: Although lower percentages of HCP cases overall reported PPE concerns after the first US peak, our results highlight the importance of developing capacity to produce and distribute PPE during times of increased demand. The difference we observed among selected groups of cases may indicate that PPE access and use were more challenging for some, such as nonphysicians and nursing home HCP. These findings underscore the need to ensure that PPE is accessible and used correctly by HCP for whom use is recommended.
Funding: None
Disclosures: None