Refine search
Actions for selected content:
26 results
14 - Medical Education
- from Part II - Learning from Interdisciplinary Perspectives
-
-
- Book:
- Sexual Harassment between Doctors
- Published online:
- 27 March 2026
- Print publication:
- 09 April 2026, pp 196-224
-
- Chapter
-
- You have access
- Open access
- HTML
- Export citation
4 - A History of Workplace Sexual Harms
- from Part I - Context
-
-
- Book:
- Sexual Harassment between Doctors
- Published online:
- 27 March 2026
- Print publication:
- 09 April 2026, pp 45-65
-
- Chapter
-
- You have access
- Open access
- HTML
- Export citation
2 - How to Be a Woman Doctor: Gender, Performance and Sexual Risk
- from Part I - Context
-
-
- Book:
- Sexual Harassment between Doctors
- Published online:
- 27 March 2026
- Print publication:
- 09 April 2026, pp 22-35
-
- Chapter
-
- You have access
- Open access
- HTML
- Export citation
3 - The Role of Men
- from Part I - Context
-
-
- Book:
- Sexual Harassment between Doctors
- Published online:
- 27 March 2026
- Print publication:
- 09 April 2026, pp 36-44
-
- Chapter
-
- You have access
- Open access
- HTML
- Export citation
15 - Therapy: Managing Occupational Sexual Harm in Medicine
- from Part II - Learning from Interdisciplinary Perspectives
-
-
- Book:
- Sexual Harassment between Doctors
- Published online:
- 27 March 2026
- Print publication:
- 09 April 2026, pp 225-234
-
- Chapter
-
- You have access
- Open access
- HTML
- Export citation
Characterizing the weed science faculty at universities in the United States of America
-
- Journal:
- Weed Science / Volume 74 / Issue 1 / 2026
- Published online by Cambridge University Press:
- 26 March 2026, e26
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Disparities amid Parity: An Intersectional Study of Publication Trends in Guatemalan Archaeology
-
- Journal:
- Advances in Archaeological Practice / Volume 14 / Issue 1 / February 2026
- Published online by Cambridge University Press:
- 03 February 2026, pp. 50-68
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Rainbow Research: Challenges and Recommendations for Sexual Orientation and Gender Identity and Expression (SOGIE) Survey Design
-
- Journal:
- Voluntas: International Journal of Voluntary and Nonprofit Organizations / Volume 34 / Issue 1 / February 2023
- Published online by Cambridge University Press:
- 01 January 2026, pp. 84-90
-
- Article
- Export citation
Different Destinations: Clarifying and Addressing Pipeline Problems for Women in Academic Archaeology
-
- Journal:
- Advances in Archaeological Practice / Volume 14 / Issue 1 / February 2026
- Published online by Cambridge University Press:
- 17 December 2025, pp. 15-32
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Food insecurity and employment income: considerations regarding gender inequalities
-
- Journal:
- Public Health Nutrition / Volume 28 / Issue 1 / 2025
- Published online by Cambridge University Press:
- 25 September 2025, e201
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

The Cambridge Companion to Women and Islam
-
- Published online:
- 12 April 2025
- Print publication:
- 17 April 2025
Girls in the Museum: Pursuing Gender Equity in Astronomy
-
- Journal:
- Proceedings of the International Astronomical Union / Volume 20 / Issue S358 / March 2024
- Published online by Cambridge University Press:
- 23 April 2026, pp. 135-138
- Print publication:
- March 2024
-
- Article
- Export citation
13 - What Money Cannot Buy
- from Part Three - The Prevention Problem
-
- Book:
- Enough
- Published online:
- 11 January 2024
- Print publication:
- 11 January 2024, pp 199-220
-
- Chapter
- Export citation
INTRODUCTION
-
- Journal:
- Journal of Law, Medicine & Ethics / Volume 50 / Issue 3 / Fall 2022
- Published online by Cambridge University Press:
- 18 November 2022, pp. 399-400
- Print publication:
- Fall 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Building Racial and Gender Equity into a National PrEP Access Program
-
- Journal:
- Journal of Law, Medicine & Ethics / Volume 50 / Issue S1 / Summer 2022
- Published online by Cambridge University Press:
- 29 July 2022, pp. 55-59
- Print publication:
- Summer 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Sex and Gender Equity in Prehospital Electrocardiogram Acquisition
-
- Journal:
- Prehospital and Disaster Medicine / Volume 37 / Issue 2 / April 2022
- Published online by Cambridge University Press:
- 09 March 2022, pp. 164-170
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Entrepreneurial Ecosystems
- A Gender Perspective
-
- Published online:
- 20 October 2021
- Print publication:
- 21 October 2021
Completed suicide and gender equality: Sex and age specific five-year data from Turkey
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, p. S834
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Suicide is a public health problem which has biopsychosocial aspects. These three compartments function differently for women and men in terms of biology and gender inequality.
ObjectivesThis study aims to investigate completed suicide rates in Turkey for women and men seperately considering age ranges for each, and their relationship with gender equality.
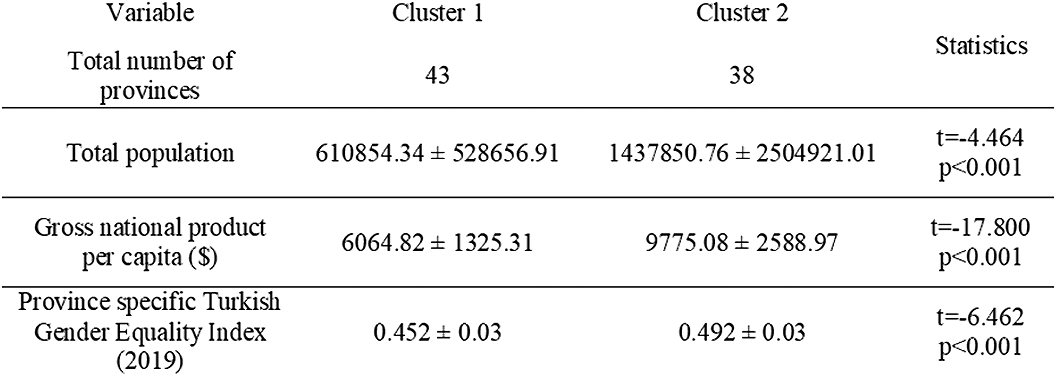
MethodsSex and age specific data between 2015-2019 was derived from Turkish Statistical Institute. Utilizing Bağdatlı Kalkan’s study (2018) and Turkey’s Gender Equality Ratings (2019), 81 cities were seperated into two clusters (Table 1). Mann Whitney U and Independent Samples T Test were applied.
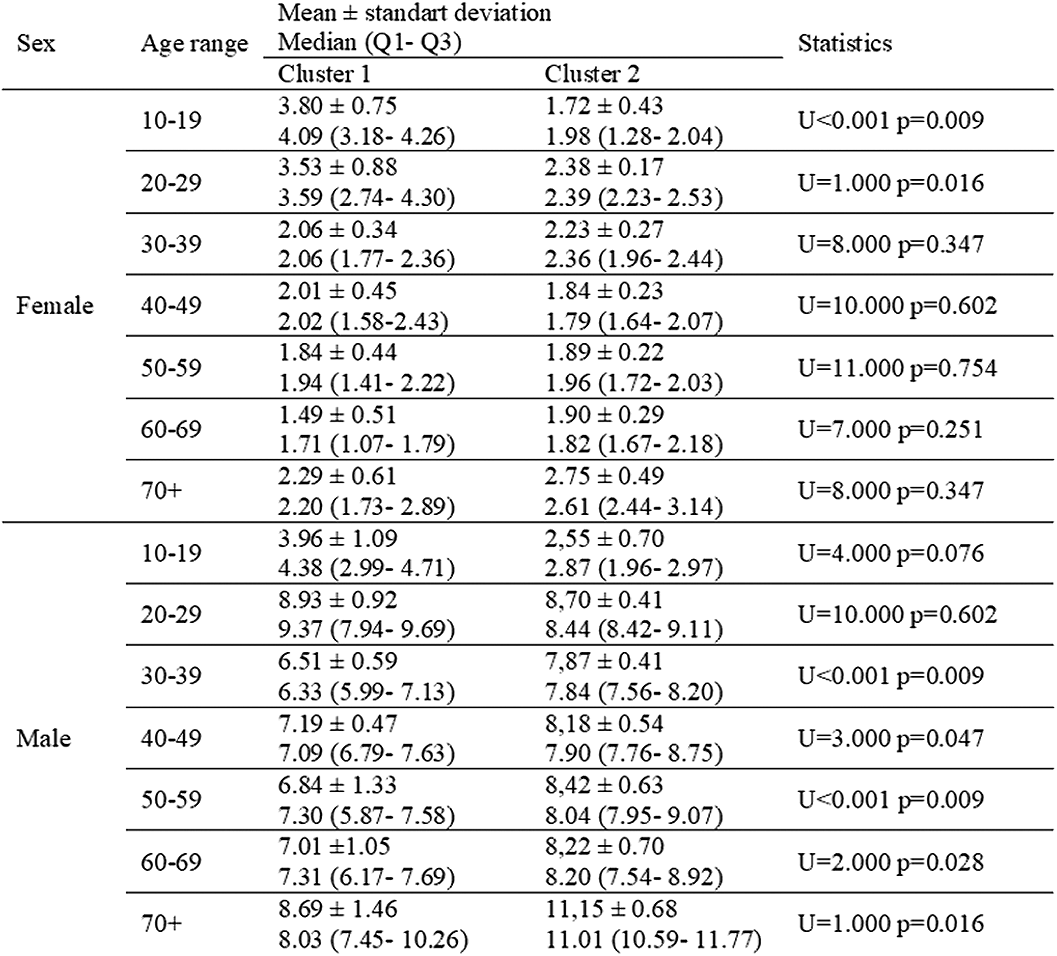
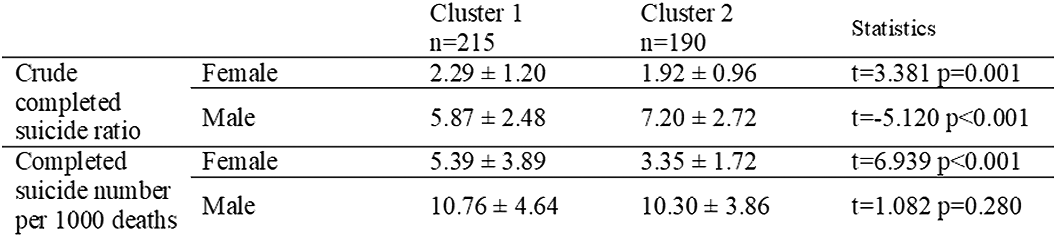
ResultsYoung women’s (<30 years old) crude completed suicide rates were higher, when crude completed suicide rates for men over the age of 30 were fewer in the cities which equality index is low (Table 2). Regardless of age ranges, in better gender equality cluster, female suicide rates were fewer, male suicide rates were higher. The number of deaths by suicide in 1000 deaths didn’t differ for men, while the rate decreases for women in better gender equality cluster (Table 3).
 Conclusions
ConclusionsGender inequality may negatively effect young women’s mental health in more patriarchal cities in Turkey from the point of completed suicide.
DisclosureNo significant relationships.



Disparity in Gender Representation of Speakers at National Emergency Medical Services Conferences: A Current Assessment and Proposed Path Forward
-
- Journal:
- Prehospital and Disaster Medicine / Volume 36 / Issue 4 / August 2021
- Published online by Cambridge University Press:
- 30 June 2021, pp. 445-449
-
- Article
- Export citation
Gender mainstreaming as a global policy paradigm: barriers to gender justice in health
-
- Journal:
- Journal of International and Comparative Social Policy / Volume 30 / Issue 1 / February 2014
- Published online by Cambridge University Press:
- 09 March 2020, pp. 28-40
-
- Article
- Export citation
