
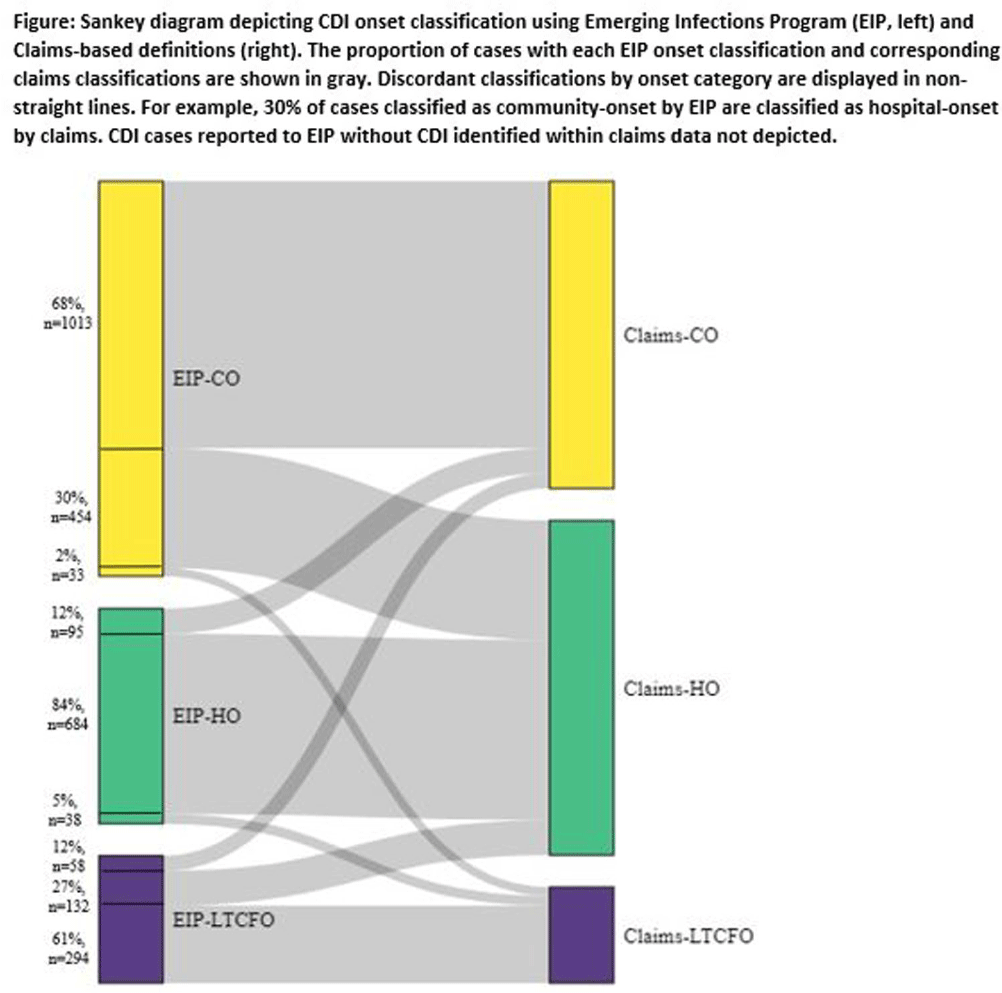
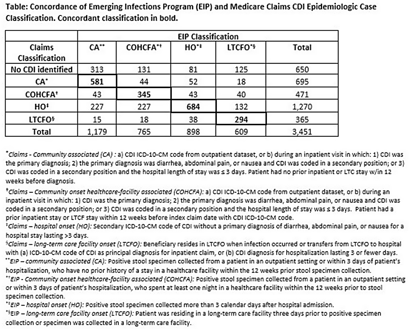
Background: Medicare claims are frequently used to study Clostridioides difficile infection (CDI) epidemiology. Categorizing CDI based on location of onset and potential exposure is critical in understanding transmission patterns and prevention strategies. While claims data are well-suited for identifying prior healthcare utilization exposures, they lack specimen collection and diagnosis dates to assign likely location of onset. Algorithms to classify CDI onset and healthcare association using claims data have been published, but the degree of misclassification is unknown. Methods: We linked patients with laboratory-confirmed CDI reported to four Emerging Infections Program (EIP) sites from 2016-2020 to Medicare beneficiaries using residence, birth date, sex, and hospitalization and/or healthcare exposure dates. Uniquely linked patients with fee-for-service Medicare A/B coverage and complete EIP case report forms were included. Patients with a claims CDI diagnosis code within ±28 days of a positive CDI test reported to EIP were categorized as hospital-onset (HO), long-term care facility onset (LTCFO), or community-onset (CO, either healthcare facility-associated [COHCFA] or community-associated [CA]) using a previously published algorithm based on claim type, ICD-10-CM code position, and duration of hospitalization (if applicable). EIP classifies CDI into these categories using positive specimen collection date and other information from chart review (e.g. admit/discharge dates). We assessed concordance of EIP and claims case classifications using Cohen’s kappa. Results: Of 10,002 eligible EIP-identified CDI cases, 7,064 were linked to a unique beneficiary; 3,451 met Medicare A/B fee-for-service coverage inclusion criteria. Of these, 650 (19%) did not have a claims diagnosis code ±28 days of the EIP specimen collection date (Table); 48% (313/650) of those without a claims diagnosis code were categorized by EIP as CA CDI. Among those with a CDI diagnosis code, concurrence of claims-based and EIP CDI classification was 68% (κ=0.56). Concurrence was highest for HO and lowest for COHCFA CDI. A substantial number of EIP-classified CO CDIs (30%, Figure) were misclassified as HO using the claims-based algorithm; half of these had a primary ICD-10 diagnosis code of sepsis (226/454; 50%). Conclusions: Evidence of CDI in claims data was found for 81% of EIP-reported CDI cases. Medicare classification algorithms concurred with the EIP classification in 68% of cases. Discordance was most common for community-onset CDI patients, many of whom were hospitalized with a primary diagnosis of sepsis. Misclassification of CO-CDI as HO may bias findings of claims-based CDI studies.
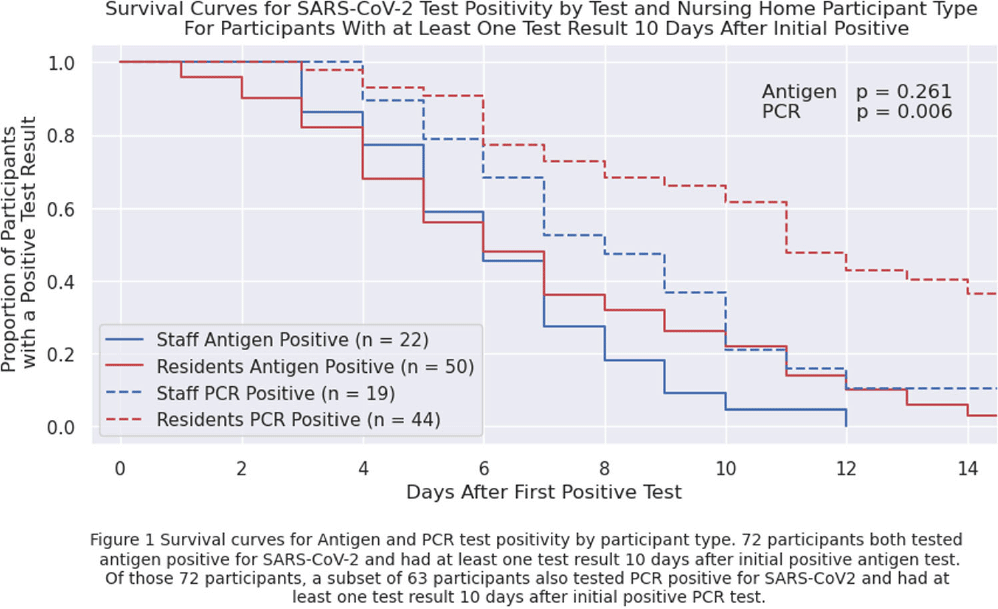
Background: Nursing home (NH) residents are at high risk of COVID-19 from exposure to infected staff and other residents. Understanding SARS-CoV-2 viral RNA kinetics in residents and staff can guide testing, isolation, and return to work recommendations. We sought to determine the duration of antigen test and polymerase chain reaction (PCR) positivity in a cohort of NH residents and staff. Methods: We prospectively collected data on SARS-CoV-2 viral kinetics from April 2023 through November 2023. Staff and residents could enroll prospectively or upon a positive test (identified through routine clinical testing, screening, or outbreak response testing). Participating facilities performed routine clinical testing; asymptomatic testing of contacts was performed within 48 hours if an outbreak or known exposure occurred and upon (re-) admission. Enrolled participants who tested positive for SARS-CoV-2 were re-tested daily for 14 days with both nasal antigen and nasal PCR tests. All PCR tests were run by a central lab with the same assay. We conducted a Kaplan-Meier survival analysis on time to first negative test restricted to participants who initially tested positive (day zero) and had at least one test ≥10 days after initially testing positive with the same test type; a participant could contribute to both antigen and PCR survival curves. We compared survival curves for staff and residents using the log-rank test. Results: Twenty-four nursing homes in eight states participated; 587 participants (275 residents, 312 staff) enrolled in the evaluation, participants were only tested through routine clinical or outbreak response testing. Seventy-two participants tested positive for antigen; of these, 63 tested PCR-positive. Residents were antigen- and PCR-positive longer than staff (Figure 1), but this finding is only statistically significant (p=0.006) for duration of PCR positivity. Five days after the first positive test, 56% of 50 residents and 59% of 22 staff remained antigen-positive; 91% of 44 residents and 79% of 19 staff were PCR-positive. Ten days after the first positive test, 22% of 50 residents and 5% of 22 staff remained antigen-positive; 61% of 44 residents and 21% of 19 staff remained PCR-positive. Conclusions: Most NH residents and staff with SARS-CoV-2 remained antigen- or PCR-positive 5 days after the initial positive test; however, differences between staff and resident test positivity were noted at 10 days. These data can inform recommendations for testing, duration of NH resident isolation, and return to work guidance for staff. Additional viral culture data may strengthen these conclusions.
Disclosure: Stefan Gravenstein: Received consulting and speaker fees from most vaccine manufacturers (Sanofi, Seqirus, Moderna, Merck, Janssen, Pfizer, Novavax, GSK, and have or expect to receive grant funding from several (Sanofi, Seqirus, Moderna, Pfizer, GSK). Lona Mody: NIH, VA, CDC, Kahn Foundation; Honoraria: UpToDate; Contracted Research: Nano-Vibronix
We recently reported on the radio-frequency attenuation length of cold polar ice at Summit Station, Greenland, based on bi-static radar measurements of radio-frequency bedrock echo strengths taken during the summer of 2021. Those data also allow studies of (a) the relative contributions of coherent (such as discrete internal conducting layers with sub-centimeter transverse scale) vs incoherent (e.g. bulk volumetric) scattering, (b) the magnitude of internal layer reflection coefficients, (c) limits on signal propagation velocity asymmetries (‘birefringence’) and (d) limits on signal dispersion in-ice over a bandwidth of ~100 MHz. We find that (1) attenuation lengths approach 1 km in our band, (2) after averaging 10 000 echo triggers, reflected signals observable over the thermal floor (to depths of ~1500 m) are consistent with being entirely coherent, (3) internal layer reflectivities are ≈–60$\to$ –70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.
–70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.

