GX is a code designed to solve the nonlinear gyrokinetic system for low-frequency turbulence in magnetized plasmas, particularly tokamaks and stellarators. In GX, our primary motivation and target is a fast gyrokinetic solver that can be used for fusion reactor design and optimization along with wide-ranging physics exploration. This has led to several code and algorithm design decisions, specifically chosen to prioritize time to solution. First, we have used a discretization algorithm that is pseudospectral in the entire phase space, including a Laguerre–Hermite pseudospectral formulation of velocity space, which allows for smooth interpolation between coarse gyrofluid-like resolutions and finer conventional gyrokinetic resolutions and efficient evaluation of a model collision operator. Additionally, we have built GX to natively target graphics processors (GPUs), which are among the fastest computational platforms available today. Finally, we have taken advantage of the reactor-relevant limit of small $\rho _*$ by using the radially local flux-tube approach. In this paper we present details about the gyrokinetic system and the numerical algorithms used in GX to solve the system. We then present several numerical benchmarks against established gyrokinetic codes in both tokamak and stellarator magnetic geometries to verify that GX correctly simulates gyrokinetic turbulence in the small $\rho _*$
by using the radially local flux-tube approach. In this paper we present details about the gyrokinetic system and the numerical algorithms used in GX to solve the system. We then present several numerical benchmarks against established gyrokinetic codes in both tokamak and stellarator magnetic geometries to verify that GX correctly simulates gyrokinetic turbulence in the small $\rho _*$ limit. Moreover, we show that the convergence properties of the Laguerre–Hermite spectral velocity formulation are quite favourable for nonlinear problems of interest. Coupled with GPU acceleration, which we also investigate with scaling studies, this enables GX to be able to produce useful turbulence simulations in minutes on one (or a few) GPUs and higher fidelity results in a few hours using several GPUs. GX is open-source software that is ready for fusion reactor design studies.
limit. Moreover, we show that the convergence properties of the Laguerre–Hermite spectral velocity formulation are quite favourable for nonlinear problems of interest. Coupled with GPU acceleration, which we also investigate with scaling studies, this enables GX to be able to produce useful turbulence simulations in minutes on one (or a few) GPUs and higher fidelity results in a few hours using several GPUs. GX is open-source software that is ready for fusion reactor design studies.
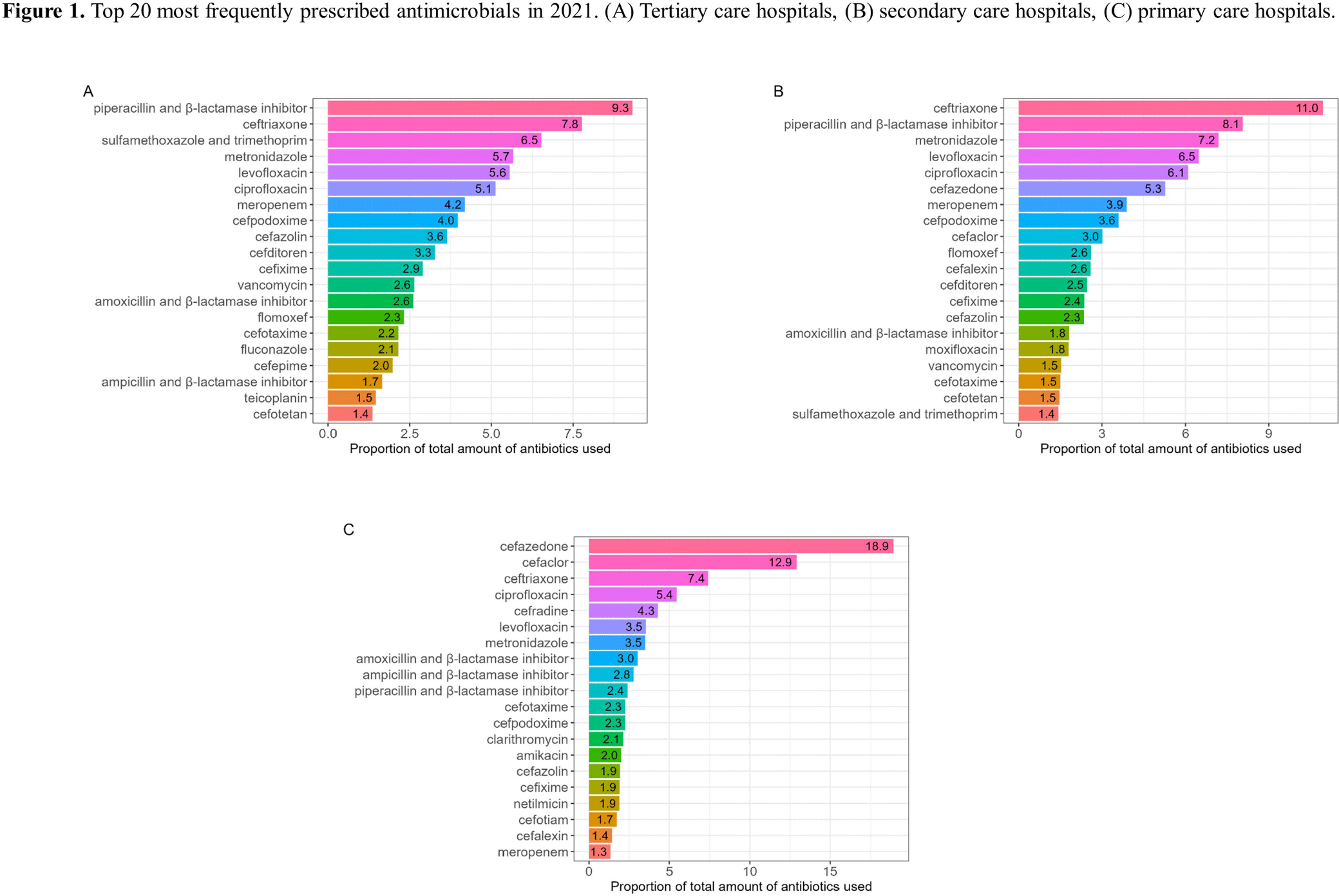
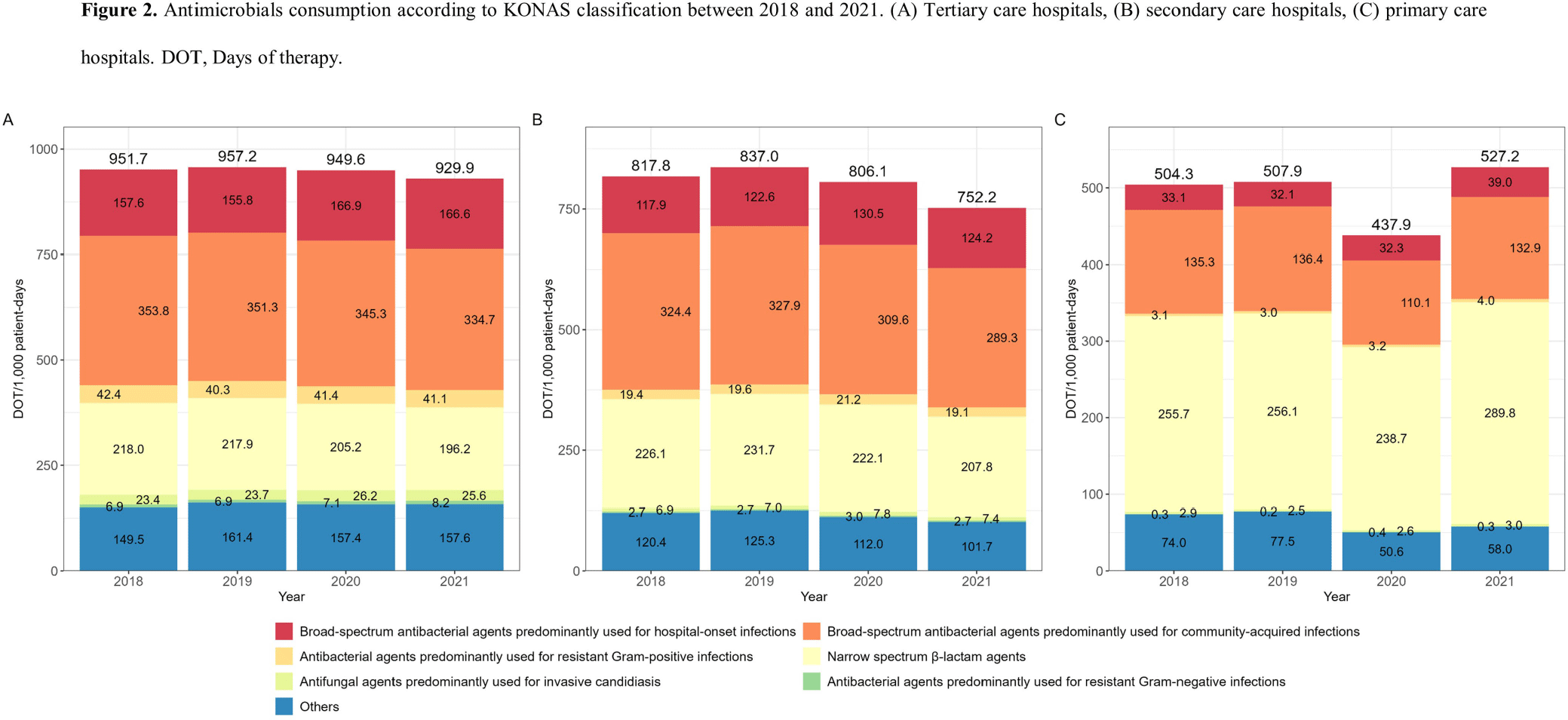
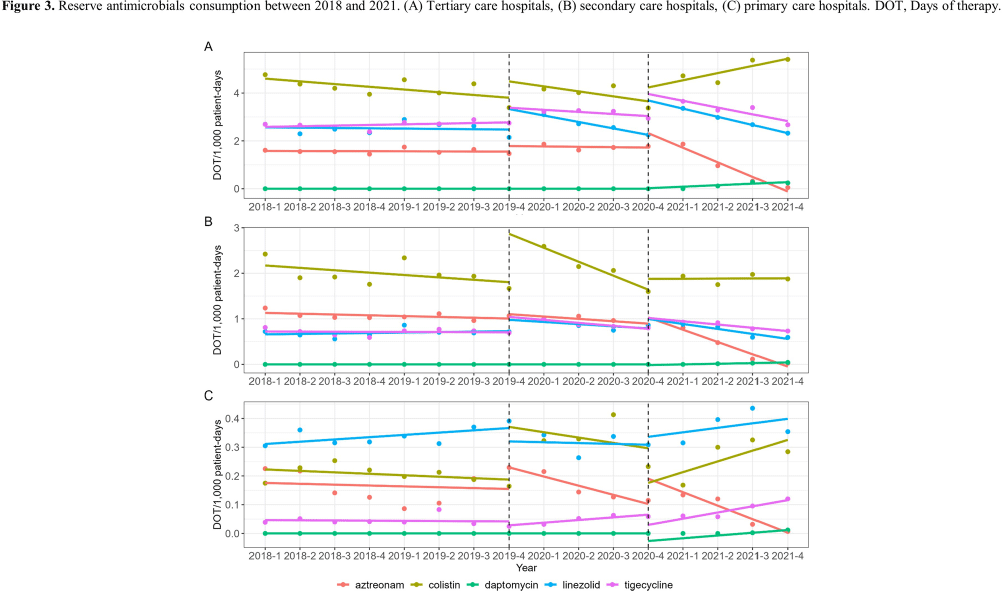
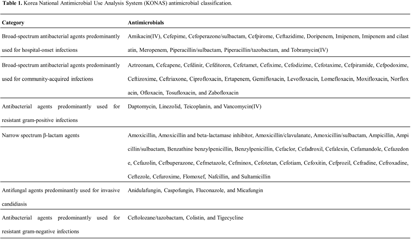
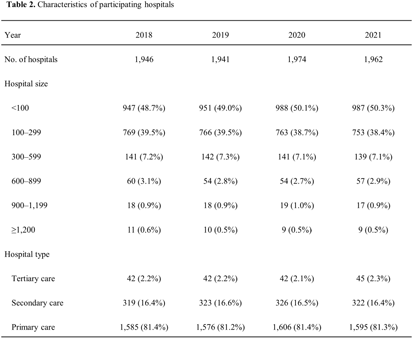
Background: Data on antimicrobial use at the national level is crucial to establish domestic antimicrobial stewardship policies and enable medical institutions to benchmark against each other. This study aimed to analyze antimicrobial use in Korean hospitals. Methods: We investigated the antimicrobials prescribed in Korean hospitals between 2018 and 2021, using data from the Health Insurance Review and Assessment. Primary care hospitals (PCHs), secondary care hospitals (SCHs), and tertiary care hospitals (TCHs) were included in this analysis. Antimicrobials were categorized according to the Korea National Antimicrobial Use Analysis System (KONAS) classification, which is suitable for measuring antimicrobial use in Korean hospitals. Results: Out of more than 1,900 hospitals, PCHs and TCHs represented the largest and lowest percentage of hospitals, respectively. The most frequently prescribed antimicrobial in 2021 was piperacillin/β-lactamase inhibitor (9.3%) in TCHs, ceftriaxone (11.0%) in SCHs, and cefazedone (18.9%) in PCHs. Between 2018 and 2021, the most used antimicrobial class according to the KONAS classification was ‘broad-spectrum antibacterial agents predominantly used for community-acquired infections’ in TCHs and SCHs, and 'narrow spectrum beta-lactam agents' in PCH. Total consumption of antimicrobials has decreased from 951.7 to 929.9 days of therapy (DOT)/1,000 patient-days in TCHs and from 817.8 to 752.2 DOT/1,000 patient-days in SCHs during study period, but not in PCHs (from 504.3 to 527.2 DOT/1,000 patient-days). Moreover, in 2021, while use of reserve antimicrobials has decreased from 13.6 to 10.7 DOT/1,000 patient-days in TCHs and from 4.6 to 3.3 DOT/1,000 patient-days in SCHs, it has increased from 0.7 to 0.8 DOT/1,000 patient-days in PCHs. Conclusion: This study confirms that antimicrobial use differs by hospital type in Korea. Recent increases of use of antimicrobials, including reserve antimicrobials, in PCHs reflect the challenges that must be addressed.