Refine search
Actions for selected content:
48206 results in Zoology
Sexual dimorphism in the context of nutrition and health
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue 2 / May 2024
- Published online by Cambridge University Press:
- 04 September 2023, pp. 109-119
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Health effects of 100% fruit and vegetable juices: evidence from human subject intervention studies
-
- Journal:
- Nutrition Research Reviews / Volume 37 / Issue 1 / June 2024
- Published online by Cambridge University Press:
- 01 September 2023, pp. 194-238
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Sustainability analysis of the Mediterranean diet: results from the French NutriNet-Santé study—CORRIGENDUM
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 1 / 14 January 2024
- Published online by Cambridge University Press:
- 01 September 2023, pp. 174-175
- Print publication:
- 14 January 2024
-
- Article
-
- You have access
- HTML
- Export citation
The association of diet-dependent acid load with colorectal cancer risk: a case–control study in Korea
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 2 / 28 January 2024
- Published online by Cambridge University Press:
- 31 August 2023, pp. 333-342
- Print publication:
- 28 January 2024
-
- Article
-
- You have access
- HTML
- Export citation
Determinates of anemia among Human Immune Deficiency Virus positive children on Anti-retro Viral Therapy in selected health facilities, Northwest Ethiopia: A Case-Control Study
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 30 August 2023, e95
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Ethnic differences in eating patterns and their associations with obesity among adults in West China
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 2 / 28 January 2024
- Published online by Cambridge University Press:
- 29 August 2023, pp. 321-332
- Print publication:
- 28 January 2024
-
- Article
-
- You have access
- HTML
- Export citation
Resting energy metabolism and sweet taste preference during the menstrual cycle in healthy women
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 3 / 14 February 2024
- Published online by Cambridge University Press:
- 29 August 2023, pp. 384-390
- Print publication:
- 14 February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
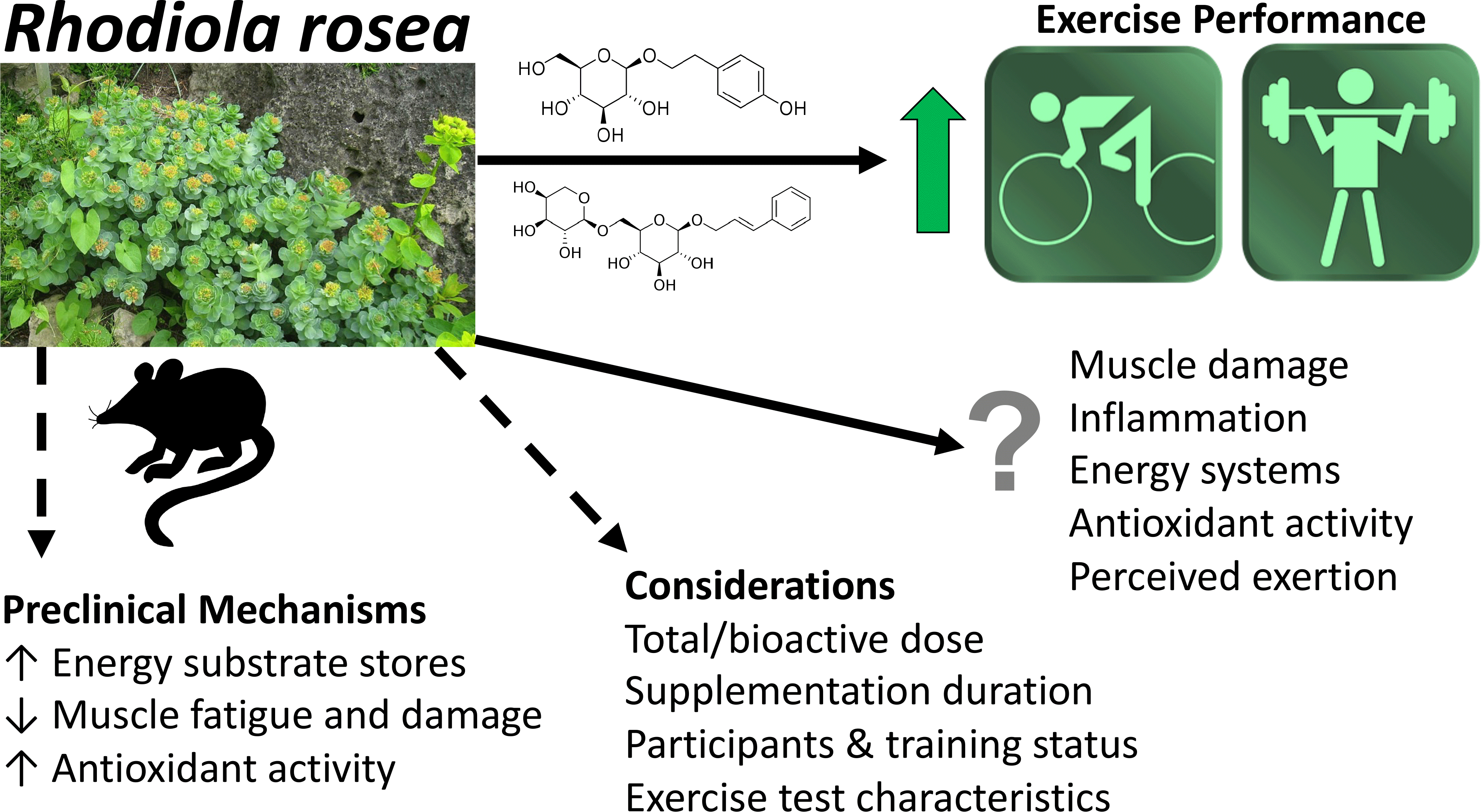
Rhodiola rosea as an adaptogen to enhance exercise performance: a review of the literature
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 3 / 14 February 2024
- Published online by Cambridge University Press:
- 29 August 2023, pp. 461-473
- Print publication:
- 14 February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Choline-mediated hepatic lipid homoeostasis in yellow catfish: unravelling choline’s lipotropic and methyl donor functions and significance of ire-1α signalling pathway
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 2 / 28 January 2024
- Published online by Cambridge University Press:
- 29 August 2023, pp. 202-213
- Print publication:
- 28 January 2024
-
- Article
-
- You have access
- HTML
- Export citation
The impact of fish oil and/or probiotics on serum fatty acids and the interaction with low-grade inflammation in pregnant women with overweight and obesity: secondary analysis of a randomised controlled trial
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 2 / 28 January 2024
- Published online by Cambridge University Press:
- 29 August 2023, pp. 296-311
- Print publication:
- 28 January 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The use of breast milk iodine concentration in the first week of lactation as a biomarker of iodine status in breast-feeding women
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 2 / 28 January 2024
- Published online by Cambridge University Press:
- 29 August 2023, pp. 286-295
- Print publication:
- 28 January 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Effects of branched-chain amino acids supplementation on patients undergoing hepatic intervention: a meta-analysis of randomised controlled trials
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 2 / 28 January 2024
- Published online by Cambridge University Press:
- 29 August 2023, pp. 276-285
- Print publication:
- 28 January 2024
-
- Article
-
- You have access
- HTML
- Export citation
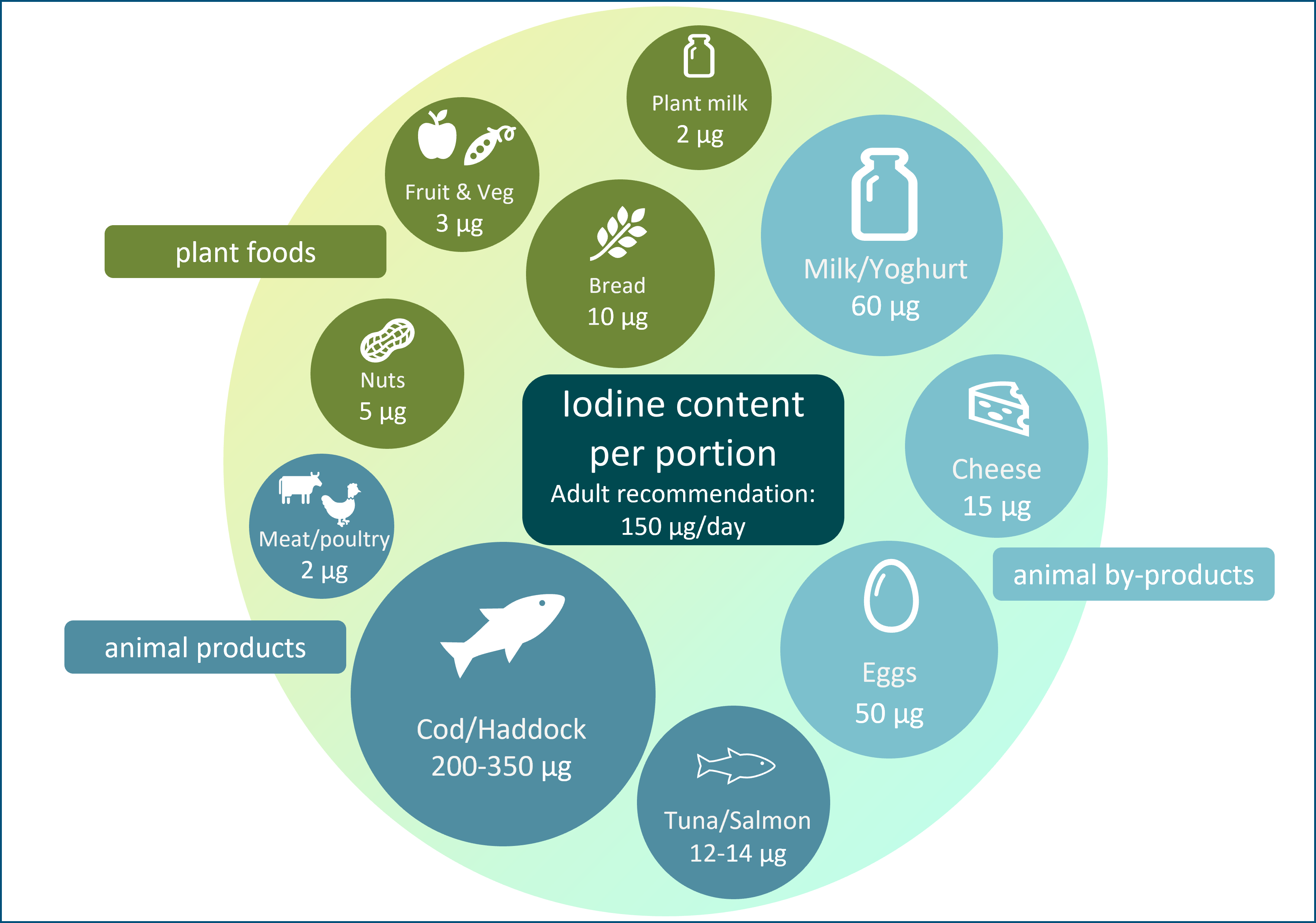
Iodine and plant-based diets: a narrative review and calculation of iodine content
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 2 / 28 January 2024
- Published online by Cambridge University Press:
- 25 August 2023, pp. 265-275
- Print publication:
- 28 January 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development of an initiatives package to increase children’s vegetable intake in long day care centres using the Multiphase Optimisation Strategy (MOST) randomised factorial experiment
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 25 August 2023, pp. 3062-3075
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Interventions to prevent obesity in Latinx children birth to 6 years globally: a systematic review
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 25 August 2023, pp. 2498-2513
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The contribution of Australian fathers in getting food on the table among families with young children
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 25 August 2023, pp. 2826-2835
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
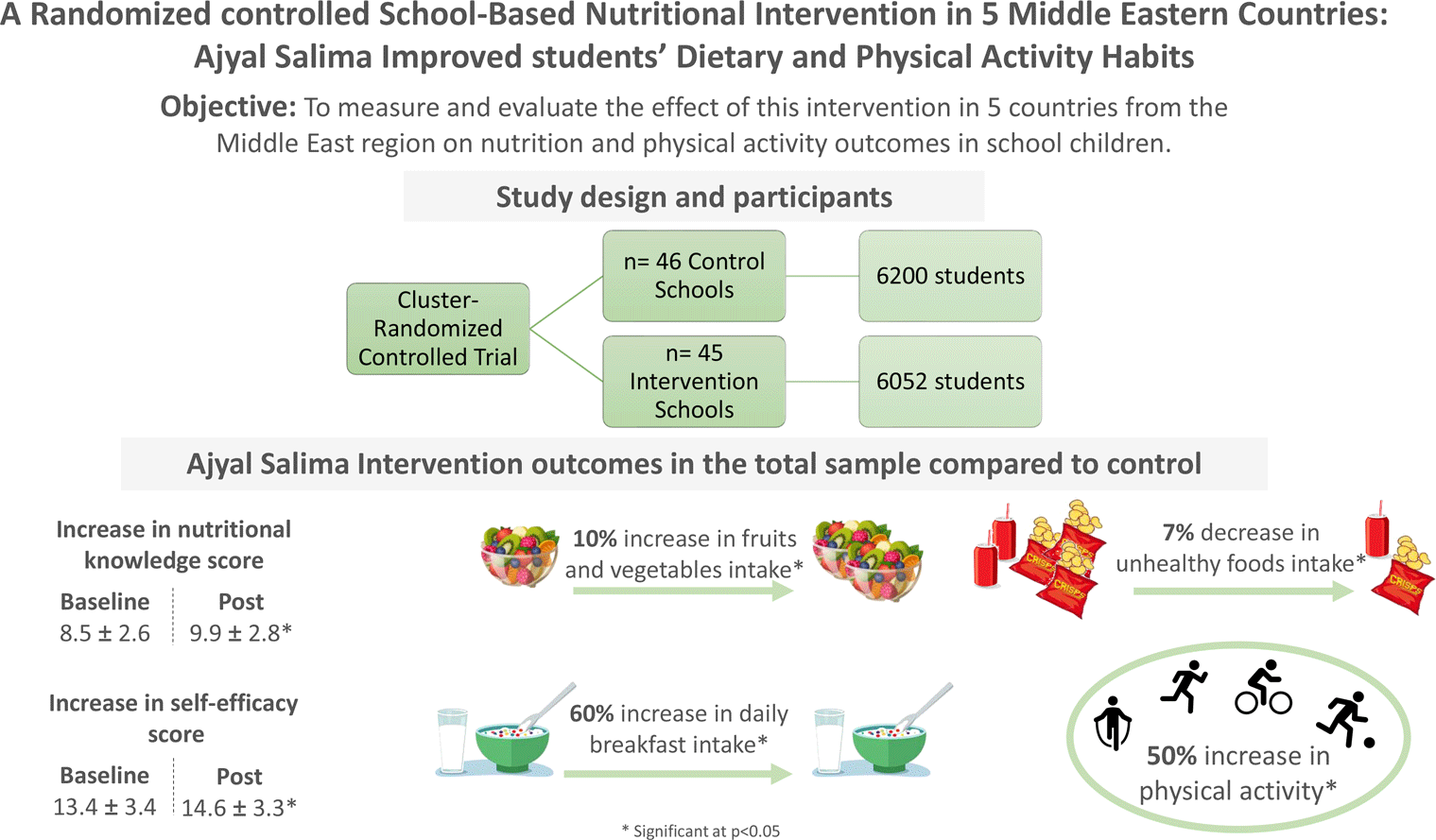
A randomised controlled school-based nutritional intervention in five Middle Eastern countries: Ajyal Salima improved students’ dietary and physical activity habits
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 25 August 2023, pp. 2036-2047
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Behavioural strategies to reduce obesity among lower socio-economic adults living in high-income countries: a Grades of Recommendation, Assessment, Development and Evaluation-assessed systematic review and meta-analysis of randomised controlled trials
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 3 / 14 February 2024
- Published online by Cambridge University Press:
- 25 August 2023, pp. 544-552
- Print publication:
- 14 February 2024
-
- Article
-
- You have access
- HTML
- Export citation
Nutrition literacy status and its association with adherence to the Mediterranean diet, anthropometric parameters and lifestyle behaviours among early adolescents
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 25 August 2023, pp. 2108-2117
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
How effective were government food box schemes for those who were shielding during the first wave of the COVID-19 pandemic in the United Kingdom? Local and national stakeholder perspectives
- Part of
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 25 August 2023, pp. 3247-3255
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
