Refine search
Actions for selected content:
48214 results in Zoology
The effects of beetroot and nitrate supplementation on body composition: a GRADE-assessed systematic review and meta-analysis
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. 1343-1356
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- HTML
- Export citation
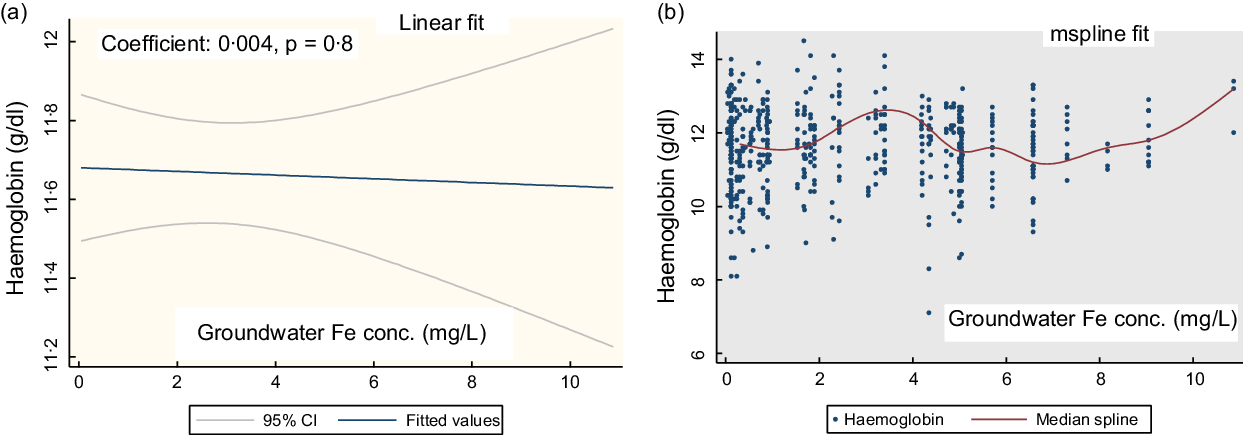
Behind the scene of the prevalence of anaemia: an extended way of reporting
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. 1115-1124
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Ecological system theory and community participation to promote healthy food environments for obesity and non-communicable diseases prevention among school-age children
- Part of
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. 1488-1500
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
PHN volume 26 issue 3 Cover and Back matter
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 3 / March 2023
- Published online by Cambridge University Press:
- 27 February 2023, p. b1
-
- Article
-
- You have access
- Open access
- Export citation
PHN volume 26 issue 3 Cover and Front matter
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 3 / March 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. f1-f3
-
- Article
-
- You have access
- Open access
- Export citation
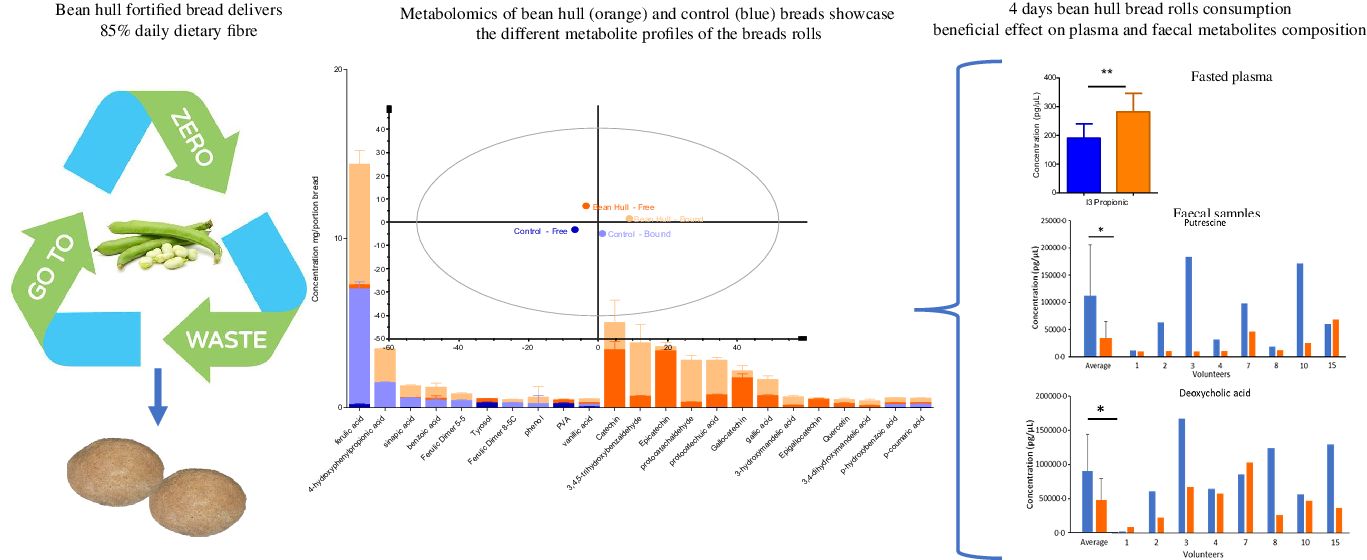
Habitual consumption of high-fibre bread fortified with bean hulls increased plasma indole-3-propionic concentration and decreased putrescine and deoxycholic acid faecal concentrations in healthy volunteers
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 9 / 14 November 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. 1521-1536
- Print publication:
- 14 November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
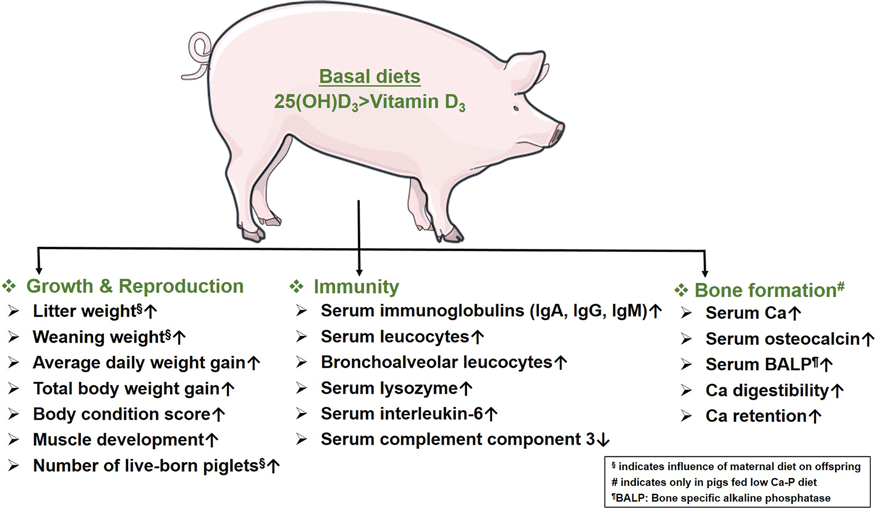
Efficacy of dietary vitamin D3 and 25(OH)D3 on reproductive capacities, growth performance, immunity and bone development in pigs
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. 1298-1307
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Operationalising multi-sectoral food- and nutrition-related policies to curb the rise in obesity in Ghana
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 27 February 2023, pp. 3230-3238
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Spatial distribution of stunting and wasting in 6–59 months children in Nepal: analysis using a Bayesian distributional bivariate probit model
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 23 February 2023, e25
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
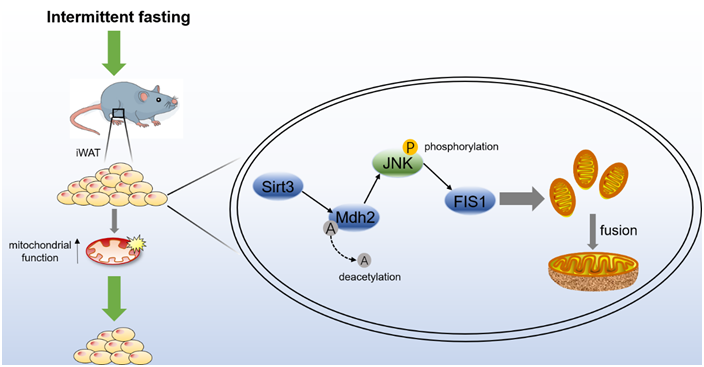
Intermittent fasting promotes adipocyte mitochondrial fusion through Sirt3-mediated deacetylation of Mdh2
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 9 / 14 November 2023
- Published online by Cambridge University Press:
- 23 February 2023, pp. 1473-1486
- Print publication:
- 14 November 2023
-
- Article
-
- You have access
- HTML
- Export citation
Experiences with energy drink consumption among Norwegian adolescents
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 23 February 2023, e30
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Efficacy of vitamin D supplementation in reducing body mass index and lipid profile in healthy young adults in Colombia: a pilot randomised controlled clinical trial
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 22 February 2023, e29
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Letter to the Editor of the Journal of Nutritional Science
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 21 February 2023, e26
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Intake and sources of dietary fibre and dietary fibre fractions in Finnish children
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 21 February 2023, pp. 1416-1426
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Response to letters provided from Marko Kerac, Marie McGrath, James A Berkley, Carlos S Grijalva-Eternod, Natasha Lelijveld, Martha Mwangome, and Eleanor Rogers (Manuscript ID JNS-LE-22-0110)
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 21 February 2023, e27
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Validation of the 2 × 24 h recall method and a 7-d web-based food diary against doubly labelled water in Danish adults
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 21 February 2023, pp. 1444-1457
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
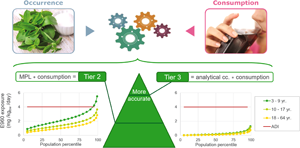
Tiered dietary exposure assessment of steviol glycosides in the Belgian population
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 21 February 2023, e28
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nutritional quality of children’s menus in restaurants: does cuisine type matter?
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 20 February 2023, pp. 1451-1455
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Ultra-processed foods: a concept in need of revision to avoid targeting healthful and sustainable plant-based foods
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 20 February 2023, pp. 1471-1472
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association between legume consumption and the intake of other foods and nutrients in the Finnish adult population
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 20 February 2023, pp. 1458-1468
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- HTML
- Export citation
