Refine search
Actions for selected content:
48214 results in Zoology
Exploring educational inequalities in hypertension control, salt knowledge and awareness, and patient advice: insights from the WHO STEPS surveys of adults from nine Eastern European and Central Asian countries
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue S1 / December 2023
- Published online by Cambridge University Press:
- 13 February 2023, pp. s20-s31
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Dietary behaviours and related lifestyles according to the presence or absence of skipping breakfast in Japanese adults: the JPHC-NEXT study
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 13 February 2023, pp. 1230-1237
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Associations between clinically diagnosed medical conditions and dietary supplement use: the US military dietary supplement use study
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 13 February 2023, pp. 1238-1253
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Maternal fish consumption and child neurodevelopment in Nutrition 1 Cohort: Seychelles Child Development Study
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 10 February 2023, pp. 1366-1372
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
What’s in a commercial meal kit? Structured review of Australian meal kits
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 09 February 2023, pp. 1284-1292
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Associations between sugar-sweetened beverages before and during pregnancy and offspring overweight/obesity in Japanese women: the TMM BirThree Cohort Study
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 09 February 2023, pp. 1222-1229
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Serum folate mediates the associations of MTHFR rs1801133 polymorphism with blood glucose levels and gestational diabetes mellitus in Chinese Han pregnant women
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 09 February 2023, pp. 1329-1337
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- HTML
- Export citation
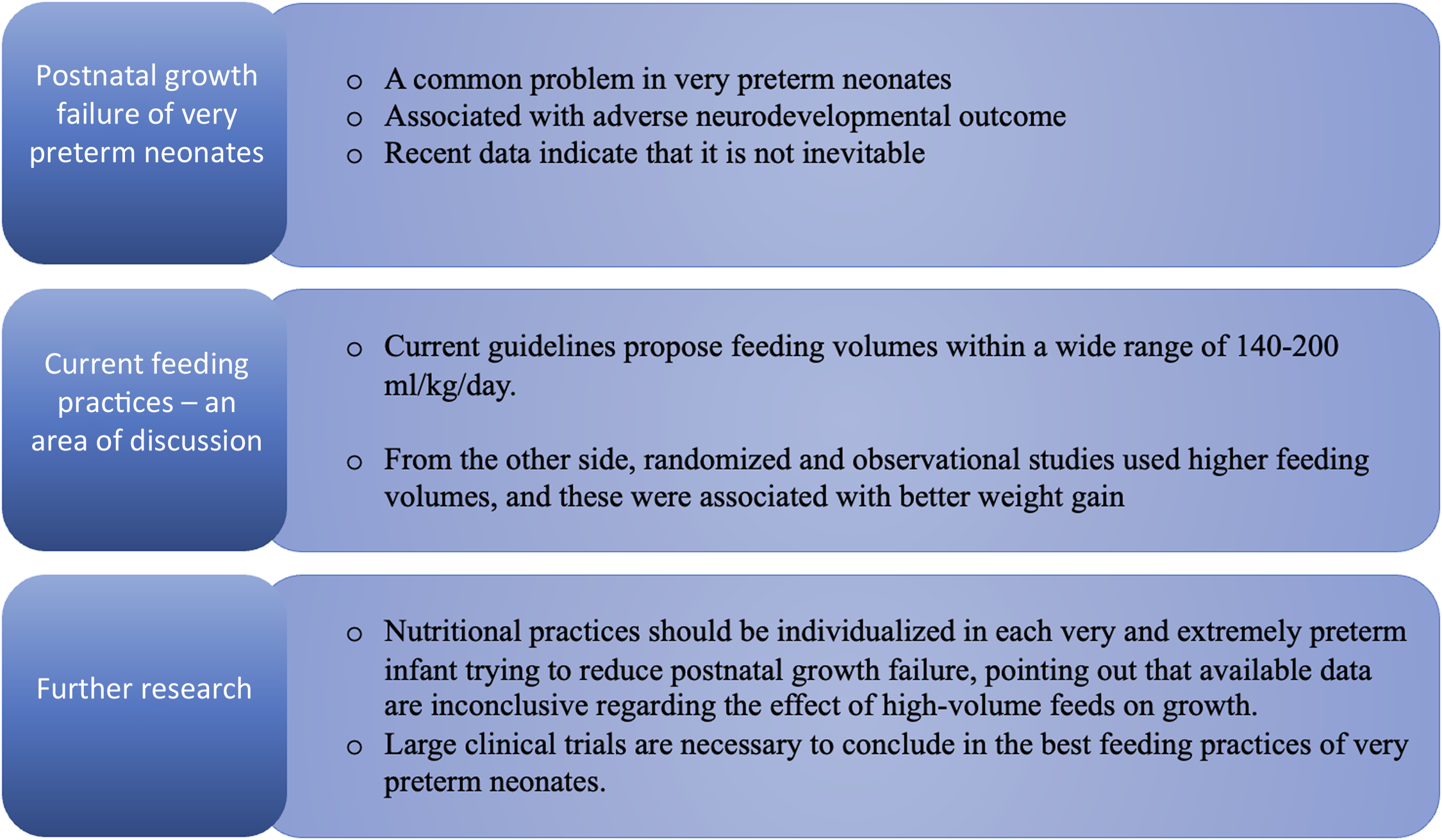
Are the current feeding volumes adequate for the growth of very preterm neonates?
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 09 February 2023, pp. 1338-1342
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Efficacy of technology-based personalised feedback on diet quality in young Australian adults: results for the advice, ideas and motivation for my eating (Aim4Me) randomised controlled trial
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 09 February 2023, pp. 1293-1305
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Vitamin D: determinants of status, indications for testing and knowledge in a convenience sample of Irish adults
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 7 / 14 October 2023
- Published online by Cambridge University Press:
- 09 February 2023, pp. 1144-1154
- Print publication:
- 14 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Rate, risk factors and estimated time to develop attrition after under-five children started moderate acute malnutrition treatment in Gubalafto, North East Ethiopia
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 08 February 2023, e15
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Caecal digestibility as an approximation of ileal protein digestibility evaluation in rats
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 08 February 2023, e18
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association between a priori and a posteriori dietary patterns and the risk of type 2 diabetes: a representative cohort study in Taiwan
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 08 February 2023, e16
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
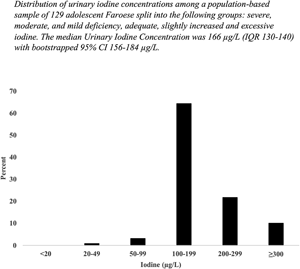
Iodine nutrition with North Atlantic living: the Faroese adolescents
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 08 February 2023, e17
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Achieving health through diet: a joint event of the Sabri Ülker Foundation and The Nutrition Society of UK and Ireland, May 2022
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 7 / 14 October 2023
- Published online by Cambridge University Press:
- 08 February 2023, pp. 1228-1238
- Print publication:
- 14 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A comparative, randomised MRI study of the physiological and appetitive responses to gelling (alginate) and non-gelling nasogastric tube feeds in healthy men
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 07 February 2023, pp. 1316-1328
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Serum levels of n-3 PUFA and colorectal cancer risk in Chinese population
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 7 / 14 October 2023
- Published online by Cambridge University Press:
- 07 February 2023, pp. 1239-1249
- Print publication:
- 14 October 2023
-
- Article
-
- You have access
- HTML
- Export citation
Dairy foods and cardiometabolic diseases: an update and a reassessment of the impact of SFA
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue 3 / September 2023
- Published online by Cambridge University Press:
- 06 February 2023, pp. 329-345
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Urinary iodine excretion and optimal time point for sampling when estimating 24-h urinary iodine
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 8 / 28 October 2023
- Published online by Cambridge University Press:
- 06 February 2023, pp. 1289-1297
- Print publication:
- 28 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development and validation of a quantitative food frequency questionnaire to assess free sugar intake among Sri Lankan preschool children
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 06 February 2023, e14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
