Refine search
Actions for selected content:
48214 results in Zoology
Factors associated with fruit and vegetable consumption among Burmese refugees
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 06 February 2023, pp. 1264-1270
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association of diet quality during pregnancy with maternal glucose metabolism in Chinese women
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 6 / 28 September 2023
- Published online by Cambridge University Press:
- 06 February 2023, pp. 958-965
- Print publication:
- 28 September 2023
-
- Article
-
- You have access
- HTML
- Export citation
Hydrolysed proteins in infant formula and child neurodevelopment up to the age of 3·5 years: the nationwide Étude Longitudinale Française depuis l’Enfance (ELFE) birth cohort
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 7 / 14 October 2023
- Published online by Cambridge University Press:
- 06 February 2023, pp. 1167-1178
- Print publication:
- 14 October 2023
-
- Article
-
- You have access
- HTML
- Export citation
Anthropometric criteria for best-identifying children at high risk of mortality: a pooled analysis of twelve cohorts
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 03 February 2023, pp. 803-819
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Child food portion sizes in the home environment: how do parents decide?
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue 3 / September 2023
- Published online by Cambridge University Press:
- 02 February 2023, pp. 386-393
-
- Article
-
- You have access
- HTML
- Export citation
Addressing inequalities and improving maternal and infant outcomes: the potential power of nutritional interventions across the reproductive cycle
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue 3 / September 2023
- Published online by Cambridge University Press:
- 02 February 2023, pp. 241-252
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
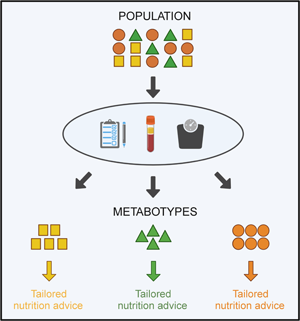
Metabotyping: a tool for identifying subgroups for tailored nutrition advice
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue 2 / May 2023
- Published online by Cambridge University Press:
- 02 February 2023, pp. 130-141
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
BJN volume 129 issue 4 Cover and Back matter
-
- Journal:
- British Journal of Nutrition / Volume 129 / Issue 4 / 28 February 2023
- Published online by Cambridge University Press:
- 02 February 2023, pp. b1-b2
- Print publication:
- 28 February 2023
-
- Article
-
- You have access
- Export citation
BJN volume 129 issue 4 Cover and Front matter
-
- Journal:
- British Journal of Nutrition / Volume 129 / Issue 4 / 28 February 2023
- Published online by Cambridge University Press:
- 02 February 2023, pp. f1-f2
- Print publication:
- 28 February 2023
-
- Article
-
- You have access
- Export citation
Prognostic value of different anthropometric indices over different measurement intervals to predict mortality in 6–59-month-old children
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 01 February 2023, pp. 1210-1221
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association between total dietary antioxidant capacity and food groups and incidence of depression in a cohort of Brazilian graduates (CUME Project)
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 7 / 14 October 2023
- Published online by Cambridge University Press:
- 01 February 2023, pp. 1155-1166
- Print publication:
- 14 October 2023
-
- Article
-
- You have access
- HTML
- Export citation
Content analysis of on-package formula labelling in Great Britain: use of marketing messages on infant, follow-on, growing-up and specialist formula
- Part of
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 8 / August 2023
- Published online by Cambridge University Press:
- 30 January 2023, pp. 1696-1705
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A peer support dietary change intervention for encouraging adoption and maintenance of the Mediterranean diet in a non-Mediterranean population (TEAM-MED): lessons learned and suggested improvements
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 30 January 2023, e13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development and evaluation of the Food Bank Health and Nutrition Assessment
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 30 January 2023, pp. 738-747
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Understanding weight status and dietary intakes among Australian school children by remoteness: a cross-sectional study
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 30 January 2023, pp. 1185-1193
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Better understanding determinants of dietary guideline adherence among Dutch adults with varying socio-economic backgrounds through a mixed-methods exploration
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 26 January 2023, pp. 1172-1184
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Comparison and convergent validity of five Mediterranean dietary indexes applied to Brazilian adults and older adults: data from a population-based study (2015 ISA-Nutrition)
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 26 January 2023, e12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Longitudinal concordance of body composition and anthropometric assessment by a novel smartphone application across a 12-week self-managed weight loss intervention
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 7 / 14 October 2023
- Published online by Cambridge University Press:
- 26 January 2023, pp. 1260-1266
- Print publication:
- 14 October 2023
-
- Article
-
- You have access
- HTML
- Export citation
Effectiveness of interactive technology-assisted interventions on promoting healthy food choices: a scoping review and meta-analysis
-
- Journal:
- British Journal of Nutrition / Volume 130 / Issue 7 / 14 October 2023
- Published online by Cambridge University Press:
- 25 January 2023, pp. 1250-1259
- Print publication:
- 14 October 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
BJN volume 129 issue 3 Cover and Front matter
-
- Journal:
- British Journal of Nutrition / Volume 129 / Issue 3 / 14 February 2023
- Published online by Cambridge University Press:
- 25 January 2023, pp. f1-f2
- Print publication:
- 14 February 2023
-
- Article
-
- You have access
- Export citation
