Refine search
Actions for selected content:
48204 results in Zoology
Several meta-analyses missing from an umbrella review of n-3 fatty acids on depression symptoms: comments concerning Lu et al.
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 9 / 14 November 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1182-1183
- Print publication:
- 14 November 2024
-
- Article
-
- You have access
- HTML
- Export citation
Improving diets and multimorbidity prevention
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 4 / December 2025
- Published online by Cambridge University Press:
- 11 November 2024, pp. 390-397
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring the impact of caloric restriction on molecular mechanisms of liver damage induced by sucrose intake in the drinking water
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 12 / 28 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1562-1574
- Print publication:
- 28 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
The potential of autonomous delivery services to increase fast-food consumption
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 11 November 2024, e246
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Anaemia prevalence, its determinants and profile of micronutrient status among rural school adolescent girls aged 14–19 years: a cross-sectional study in Nagpur district, Maharashtra, India
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 11 November 2024, e248
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Associations between iron status and psychosocial wellbeing among pregnant women in Cape Coast, Ghana: a longitudinal study
-
- Journal:
- Public Health Nutrition / Accepted manuscript
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1-29
-
- Article
-
- You have access
- Open access
- Export citation
Temporal patterns of energy intake and physical activity and cross-sectional associations with body weight status in children and adolescents: results from the Portuguese National Food, Nutrition and Physical Activity Survey 2015–2016
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 12 / 28 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1684-1697
- Print publication:
- 28 December 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Comparison of BMI, triponderal mass index and paediatric body adiposity index for predicting body fat and screening obesity in preschool children
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1466-1473
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Estimating food consumption, micronutrient intake and the contribution of large-scale food fortification to micronutrient adequacy in Tanzania
- Part of
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 11 November 2024, e230
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Coffee consumption with different additives and types, genetic variation in caffeine metabolism and new-onset acute kidney injury
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 12 / 28 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1645-1653
- Print publication:
- 28 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Associations of the serum n-6 PUFA concentrations with exercise-induced myocardial ischaemia in middle-aged and older men
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1522-1529
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Probiotics’ supplementation alleviates disease severity and improves postural balance by repairing intestinal leak in patients suffering from osteoarthritis: a double-blinded clinical trial
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 12 / 28 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1602-1610
- Print publication:
- 28 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Associations of linear growth with body composition of perinatally HIV-infected African adolescents
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 12 / 28 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1593-1601
- Print publication:
- 28 December 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Long-term effect of eating duration on all-cause mortality under different energy intake and physical activity levels
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 11 November 2024, pp. 1513-1521
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Reactive oxygen species in age-related musculoskeletal decline: implications for nutritional intervention
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 4 / December 2025
- Published online by Cambridge University Press:
- 08 November 2024, pp. 356-364
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nutritional status of Saudi obese patients undergoing laparoscopic sleeve gastrectomy, one-year follow-up study
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 08 November 2024, pp. 1454-1465
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
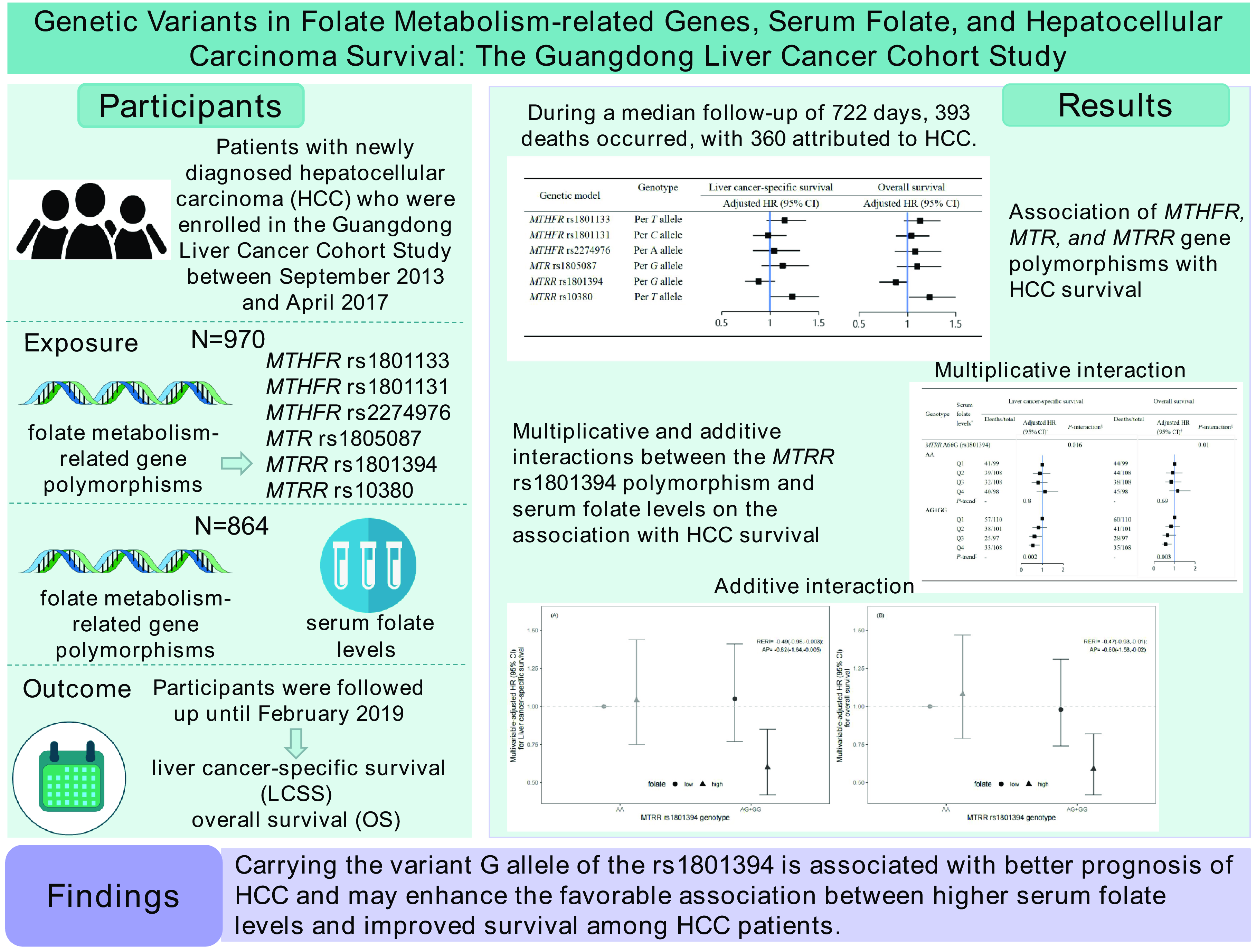
Genetic variants in folate metabolism-related genes, serum folate and hepatocellular carcinoma survival: the Guangdong Liver Cancer Cohort study
-
- Journal:
- British Journal of Nutrition / Volume 132 / Issue 11 / 14 December 2024
- Published online by Cambridge University Press:
- 07 November 2024, pp. 1411-1422
- Print publication:
- 14 December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Why health systems cannot fix problems caused by food systems: a call to integrate accountability for obesity into food systems policy
- Part of
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 07 November 2024, e228
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Evaluating the roles of food matrix, lipid micronutrients and bioactives in controlling postprandial hypertriglyceridaemia and inflammation
-
- Journal:
- Nutrition Research Reviews / Volume 38 / Issue 2 / December 2025
- Published online by Cambridge University Press:
- 07 November 2024, pp. 481-494
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prevalence of and factors associated with overweight and obesity in patients with severe mental disorders in Shenzhen: results from the urban Chinese population
-
- Journal:
- Public Health Nutrition / Volume 27 / Issue 1 / 2024
- Published online by Cambridge University Press:
- 07 November 2024, e227
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
