Refine listing
Actions for selected content:
1418034 results in Open Access
SSH volume 48 issue 1 Cover and Back matter
-
- Journal:
- Social Science History / Volume 48 / Issue 1 / Spring 2024
- Published online by Cambridge University Press:
- 06 March 2024, pp. b1-b2
- Print publication:
- Spring 2024
-
- Article
-
- You have access
- Export citation
JFQ volume 59 issue 1 Cover and Front matter
-
- Journal:
- Journal of Financial and Quantitative Analysis / Volume 59 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 14 February 2024, pp. f1-f4
- Print publication:
- February 2024
-
- Article
-
- You have access
- Export citation
Orders and Disorders of Marriage, Church, and Empire in Mid-Nineteenth-Century Ottoman Armenia
-
- Journal:
- International Journal of Middle East Studies / Volume 56 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 14 March 2024, pp. 75-90
- Print publication:
- February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
David Lehmann, After the Decolonial: Ethnicity, Gender and Social Justice in Latin America Polity, 2022, pp. xiv + 223
-
- Journal:
- Journal of Latin American Studies / Volume 56 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 12 March 2024, pp. 187-189
- Print publication:
- February 2024
-
- Article
- Export citation
Beckett’s Wasted Breath
-
- Journal:
- New Theatre Quarterly / Volume 40 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 13 February 2024, pp. 62-75
- Print publication:
- February 2024
-
- Article
-
- You have access
- Open access
- Export citation
SITI Training: Viewpoints and the Suzuki Method for Cross-Cultural Collaboration
-
- Journal:
- New Theatre Quarterly / Volume 40 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 13 February 2024, pp. 48-61
- Print publication:
- February 2024
-
- Article
- Export citation
POLICIES FOR INCLUSIVE GROWTH
-
- Journal:
- National Institute Economic Review / Volume 267 / Spring 2024
- Published online by Cambridge University Press:
- 29 April 2024, pp. 26-34
- Print publication:
- Spring 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
NMITE AND THE POLITICAL ECONOMY OF HIGHER EDUCATION: 2023 PARLIAMENTARY LECTURE
-
- Journal:
- National Institute Economic Review / Volume 267 / Spring 2024
- Published online by Cambridge University Press:
- 08 April 2025, pp. 66-73
- Print publication:
- Spring 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Effects of horizontal magnetic fields on turbulent Rayleigh–Bénard convection in a cuboid vessel with aspect ratio Γ = 5
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 31 January 2024, A24
-
- Article
- Export citation
-
Direct numerical simulations have been conducted to investigate turbulent Rayleigh– Bénard convection (RBC) of liquid metal in a cuboid vessel with aspect ratio
 $\varGamma =5$ under an imposed horizontal magnetic field. Flows with Prandtl number
$\varGamma =5$ under an imposed horizontal magnetic field. Flows with Prandtl number  $Pr=0.033$, Rayleigh numbers ranging up to
$Pr=0.033$, Rayleigh numbers ranging up to  $Ra\leq 10^{7}$, and Chandrasekhar numbers up to
$Ra\leq 10^{7}$, and Chandrasekhar numbers up to  $Q\leq 9 \times 10^6$ are considered. For weak magnetic fields, our findings reveal that a previously undiscovered decreasing region precedes the enhancement of heat transfer and kinetic energy. For moderate magnetic fields, we have reproduced the reversals of the large-scale flow, which are considered a reorganization process of the roll-like structures that were reported experimentally by Yanagisawa et al. (Phys. Rev. E, vol. 83, 2011, 036307). Nevertheless, the proposed approach of skewed-varicose instability has been substantiated as insufficient to elucidate fundamentally the phenomenon of flow reversal, an occurrence bearing a striking resemblance to the large-scale intermittency observed in magnetic channel flows. As we increase the magnetic field strength further, we observe that the energy dissipation of the system comes primarily from the viscous dissipation within the boundary layer. Consequently, the dependence of Reynolds number
$Q\leq 9 \times 10^6$ are considered. For weak magnetic fields, our findings reveal that a previously undiscovered decreasing region precedes the enhancement of heat transfer and kinetic energy. For moderate magnetic fields, we have reproduced the reversals of the large-scale flow, which are considered a reorganization process of the roll-like structures that were reported experimentally by Yanagisawa et al. (Phys. Rev. E, vol. 83, 2011, 036307). Nevertheless, the proposed approach of skewed-varicose instability has been substantiated as insufficient to elucidate fundamentally the phenomenon of flow reversal, an occurrence bearing a striking resemblance to the large-scale intermittency observed in magnetic channel flows. As we increase the magnetic field strength further, we observe that the energy dissipation of the system comes primarily from the viscous dissipation within the boundary layer. Consequently, the dependence of Reynolds number  $Re$ on
$Re$ on  $Q$ approaches a scaling as
$Q$ approaches a scaling as  $Re\,Pr/Ra^{2/3} \sim Q^{-1/3}$. At the same time, we find the law for the cutoff frequency that separates large quasi-two-dimensional scales from small three-dimensional ones in RBC flow, which scales with the interaction parameter as
$Re\,Pr/Ra^{2/3} \sim Q^{-1/3}$. At the same time, we find the law for the cutoff frequency that separates large quasi-two-dimensional scales from small three-dimensional ones in RBC flow, which scales with the interaction parameter as  ${\sim }N^{1/3}$.
${\sim }N^{1/3}$.








Mitigating Unemployment Stigma: Racialized Differences in Impression Management among Urban and Suburban Jobseekers
-
- Journal:
- Du Bois Review: Social Science Research on Race / Volume 21 / Issue 2 / Fall 2024
- Published online by Cambridge University Press:
- 31 January 2024, pp. 273-292
-
- Article
- Export citation
Effectiveness and predictors of group cognitive behaviour therapy outcome for generalised anxiety disorder in an out-patient hospital setting
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 52 / Issue 4 / July 2024
- Published online by Cambridge University Press:
- 31 January 2024, pp. 440-455
- Print publication:
- July 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The characteristics of the circular hydraulic jump and vortex structure
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 31 January 2024, A15
-
- Article
- Export citation
-
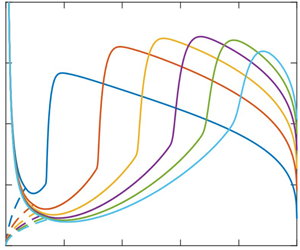
In an effort to capture the continuous hydraulic jump and flow structure for a jet impinging on a disk, we recently proposed a composite mean-field thin-film approach consisting of subdividing the flow domain into three distinct connected regions of increasing gravity strength (Wang et al., J. Fluid Mech., vol. 966, 2023, A15). In the present study, we further validate our approach, and examine the characteristics and structure of the circular jump and recirculation. The influence of the disk radius is found to be significant, especially in the subcritical region. Below a disk radius, the jump transits from type Ia to type 0 after the recirculation zone has faded. The supercritical flow and jump location are insensitive to the disk size, but the jump length and height as well as the vortex size are strongly affected, all decreasing with decreasing disk radius, exhibiting a maximum with the flow rate for a small disk. The jump is relatively steep with a strong recirculation zone for a high obstacle at the disk edge. Comparison against the Navier–Stokes solution of Askarizadeh et al. (Phys. Rev. Fluids, vol. 4, 2019, 114002; Intl J. Heat Mass Transfer, vol. 146, 2020, 118823) for the weak and intermediate surface tension suggests that the surface tension effect is unimportant for a high obstacle for a jump of type 0 or type Ia. The film thickness at the disk edge for a freely draining film is found to comprise, in addition to a static component (capillary length), a dynamic component:
 ${h_\infty }\sim {(Fr/{r_\infty })^{2/3}}$ that we establish by minimizing the Gibbs free energy at the disk edge, and, equivalently, is also the consequence of the flow becoming supercritical near the edge. By assuming negligible film slope and curvature at the leading edge of the jump and maximum height at the trailing edge, we show that the jump length is related to the jump radius as
${h_\infty }\sim {(Fr/{r_\infty })^{2/3}}$ that we establish by minimizing the Gibbs free energy at the disk edge, and, equivalently, is also the consequence of the flow becoming supercritical near the edge. By assuming negligible film slope and curvature at the leading edge of the jump and maximum height at the trailing edge, we show that the jump length is related to the jump radius as  ${L_J}\sim Re{(F{r^2}/{r_J}^5)^{1/3}}$. The vortex length follows the same behaviour. The energy loss and conjugate depth ratio exhibit a maximum with the flow rate, which we show to originate from the descending and ascending branches of the supercritical film thickness. The presence of the jump is not necessarily commensurate with that of a recirculation; the existence of the vortex closely depends on the upstream curvature and steepness of the jump. The surface separating the regions of existence/non-existence of the recirculation is given by the universal relation
${L_J}\sim Re{(F{r^2}/{r_J}^5)^{1/3}}$. The vortex length follows the same behaviour. The energy loss and conjugate depth ratio exhibit a maximum with the flow rate, which we show to originate from the descending and ascending branches of the supercritical film thickness. The presence of the jump is not necessarily commensurate with that of a recirculation; the existence of the vortex closely depends on the upstream curvature and steepness of the jump. The surface separating the regions of existence/non-existence of the recirculation is given by the universal relation  $R{e^{10/3}}F{r^2} = 9r_\infty ^9/50$. The jump can be washed off the edge of the disk, particularly at low viscosity and small disk size. The flow in the supercritical region remains insensitive to the change in gravity level and disk size but is greatly affected by viscosity.
$R{e^{10/3}}F{r^2} = 9r_\infty ^9/50$. The jump can be washed off the edge of the disk, particularly at low viscosity and small disk size. The flow in the supercritical region remains insensitive to the change in gravity level and disk size but is greatly affected by viscosity.



Travelling Barricades: Transnational Networks, Diffusion and the Dynamics of 1980s Squatter Conflicts in Western Europe – CORRIGENDUM
-
- Journal:
- Contemporary European History / Volume 33 / Issue 2 / May 2024
- Published online by Cambridge University Press:
- 31 January 2024, p. 809
- Print publication:
- May 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Flows with free boundaries and hydrodynamic singularities
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 31 January 2024, A23
-
- Article
- Export citation
Arazyme secreted by Serratia proteamaculans: current understanding in animal husbandry – CORRIGENDUM
-
- Journal:
- The Journal of Agricultural Science / Volume 161 / Issue 5 / October 2023
- Published online by Cambridge University Press:
- 31 January 2024, p. 703
-
- Article
-
- You have access
- HTML
- Export citation
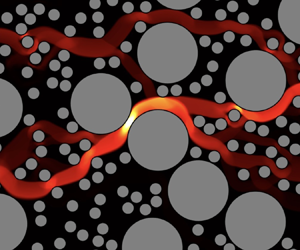
Yielding to percolation: a universal scale
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 31 January 2024, A14
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Path instability of deformable bubbles rising in Newtonian liquids: a linear study
-
- Journal:
- Journal of Fluid Mechanics / Volume 980 / 10 February 2024
- Published online by Cambridge University Press:
- 31 January 2024, A19
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Thanks to Reviewers
-
- Journal:
- The Cognitive Behaviour Therapist / Volume 17 / 2024
- Published online by Cambridge University Press:
- 31 January 2024, e2
-
- Article
-
- You have access
- HTML
- Export citation
