We present the serendipitous radio-continuum discovery of a likely Galactic supernova remnant (SNR) G305.4–2.2. This object displays a remarkable circular symmetry in shape, making it one of the most circular Galactic SNRs known. Nicknamed Teleios due to its symmetry, it was detected in the new Australian Square Kilometre Array Pathfinder (ASKAP) Evolutionary Map of the Universe (EMU) radio–continuum images with an angular size of 1 320 $^{\prime\prime}$
$^{\prime\prime}$ $\times$1 260
$\times$1 260 $^{\prime\prime}$ and PA = 0
$^{\prime\prime}$ and PA = 0 $^\circ$. While there is a hint of possible H
$^\circ$. While there is a hint of possible H $\alpha$ and gamma-ray emission, Teleios is exclusively seen at radio–continuum frequencies. Interestingly, Teleios is not only almost perfectly symmetric, but it also has one of the lowest surface brightnesses discovered among Galactic SNRs and a steep spectral index of
$\alpha$ and gamma-ray emission, Teleios is exclusively seen at radio–continuum frequencies. Interestingly, Teleios is not only almost perfectly symmetric, but it also has one of the lowest surface brightnesses discovered among Galactic SNRs and a steep spectral index of  $\alpha$=–0.6
$\alpha$=–0.6 $\pm$0.3. Our best estimates from Hi studies and the
$\pm$0.3. Our best estimates from Hi studies and the  $\Sigma$–D relation place Teleios as a type Ia SNR at a distance of either
$\Sigma$–D relation place Teleios as a type Ia SNR at a distance of either  $\sim$2.2 kpc (near-side) or
$\sim$2.2 kpc (near-side) or  $\sim$7.7 kpc (far-side). This indicates two possible scenarios, either a young (under 1 000 yr) or a somewhat older SNR (over 10 000 yr). With a corresponding diameter of 14/48 pc, our evolutionary studies place Teleios at the either early or late Sedov phase, depending on the distance/diameter estimate. However, our modelling also predicts X-ray emission, which we do not see in the present generation of eROSITA images. We also explored a type Iax explosion scenario that would point to a much closer distance of
$\sim$7.7 kpc (far-side). This indicates two possible scenarios, either a young (under 1 000 yr) or a somewhat older SNR (over 10 000 yr). With a corresponding diameter of 14/48 pc, our evolutionary studies place Teleios at the either early or late Sedov phase, depending on the distance/diameter estimate. However, our modelling also predicts X-ray emission, which we do not see in the present generation of eROSITA images. We also explored a type Iax explosion scenario that would point to a much closer distance of  $\lt$1 kpc and Teleios size of only
$\lt$1 kpc and Teleios size of only  $\sim$3.3 pc, which would be similar to the only known type Iax remnant SN1181. Unfortunately, all examined scenarios have their challenges, and no definitive Supernova (SN) origin type can be established at this stage. Remarkably, Teleios has retained its symmetrical shape as it aged even to such a diameter, suggesting expansion into a rarefied and isotropic ambient medium. The low radio surface brightness and the lack of pronounced polarisation can be explained by a high level of ambient rotation measure (RM), with the largest RM being observed at Teleios’s centre.
$\sim$3.3 pc, which would be similar to the only known type Iax remnant SN1181. Unfortunately, all examined scenarios have their challenges, and no definitive Supernova (SN) origin type can be established at this stage. Remarkably, Teleios has retained its symmetrical shape as it aged even to such a diameter, suggesting expansion into a rarefied and isotropic ambient medium. The low radio surface brightness and the lack of pronounced polarisation can be explained by a high level of ambient rotation measure (RM), with the largest RM being observed at Teleios’s centre.
Observations of the intracluster medium (ICM) in the outskirts of galaxy clusters reveal shocks associated with gas accretion from the cosmic web. Previous work based on non-radiative cosmological hydrodynamical simulations have defined the shock radius,  $r_{\text{shock}}$, using the ICM entropy,
$r_{\text{shock}}$, using the ICM entropy,  $K \propto T/{n_\mathrm{e}}^{2/3}$, where T and
$K \propto T/{n_\mathrm{e}}^{2/3}$, where T and  $n_{\text{e}}$ are the ICM temperature and electron density, respectively; the
$n_{\text{e}}$ are the ICM temperature and electron density, respectively; the  $r_{\text{shock}}$ is identified with either the radius at which K is a maximum or at which its logarithmic slope is a minimum. We investigate the relationship between
$r_{\text{shock}}$ is identified with either the radius at which K is a maximum or at which its logarithmic slope is a minimum. We investigate the relationship between  $r_{\text{shock}}$, which is driven by gravitational hydrodynamics and shocks, and the splashback radius,
$r_{\text{shock}}$, which is driven by gravitational hydrodynamics and shocks, and the splashback radius,  $r_{\text{splash}}$, which is driven by the gravitational dynamics of cluster stars and dark matter and is measured from their mass profile. Using 324 clusters from The Three Hundred project of cosmological galaxy formation simulations, we quantify statistically how
$r_{\text{splash}}$, which is driven by the gravitational dynamics of cluster stars and dark matter and is measured from their mass profile. Using 324 clusters from The Three Hundred project of cosmological galaxy formation simulations, we quantify statistically how  $r_{\text{shock}}$ relates to
$r_{\text{shock}}$ relates to  $r_{\text{splash}}$. Depending on our definition, we find that the median
$r_{\text{splash}}$. Depending on our definition, we find that the median  $r_{\text{shock}} \simeq 1.38 r_{\text{splash}} (2.58 R_{200})$ when K reaches its maximum and
$r_{\text{shock}} \simeq 1.38 r_{\text{splash}} (2.58 R_{200})$ when K reaches its maximum and  $r_{\text{shock}} \simeq 1.91 r_{\text{splash}} (3.54 R_{200})$ when its logarithmic slope is a minimum; the best-fit linear relation increases as
$r_{\text{shock}} \simeq 1.91 r_{\text{splash}} (3.54 R_{200})$ when its logarithmic slope is a minimum; the best-fit linear relation increases as  $r_{\text{shock}} \propto 0.65 r_{\text{splash}}$. We find that
$r_{\text{shock}} \propto 0.65 r_{\text{splash}}$. We find that  $r_{\text{shock}}/R_{200}$ and
$r_{\text{shock}}/R_{200}$ and  $r_{\text{splash}}/R_{200}$ anti-correlate with virial mass,
$r_{\text{splash}}/R_{200}$ anti-correlate with virial mass,  $M_{200}$, and recent mass accretion history, and
$M_{200}$, and recent mass accretion history, and  $r_{\text{shock}}/r_{\text{splash}}$ tends to be larger for clusters with higher recent accretion rates. We discuss prospects for measuring
$r_{\text{shock}}/r_{\text{splash}}$ tends to be larger for clusters with higher recent accretion rates. We discuss prospects for measuring  $r_{\text{shock}}$ observationally and how the relationship between
$r_{\text{shock}}$ observationally and how the relationship between  $r_{\text{shock}}$ and
$r_{\text{shock}}$ and  $r_{\text{splash}}$ can be used to improve constraints from radio, X-ray, and thermal Sunyaev-Zeldovich surveys that target the interface between the cosmic web and clusters.
$r_{\text{splash}}$ can be used to improve constraints from radio, X-ray, and thermal Sunyaev-Zeldovich surveys that target the interface between the cosmic web and clusters.
We present a re-discovery of G278.94+1.35a as possibly one of the largest known Galactic supernova remnants (SNRs) – that we name Diprotodon. While previously established as a Galactic SNR, Diprotodon is visible in our new Evolutionary Map of the Universe (EMU) and GaLactic and Extragalactic All-sky MWA (GLEAM) radio continuum images at an angular size of  $3{{{{.\!^\circ}}}}33\times3{{{{.\!^\circ}}}}23$, much larger than previously measured. At the previously suggested distance of 2.7 kpc, this implies a diameter of 157
$3{{{{.\!^\circ}}}}33\times3{{{{.\!^\circ}}}}23$, much larger than previously measured. At the previously suggested distance of 2.7 kpc, this implies a diameter of 157 $\times$152 pc. This size would qualify Diprotodon as the largest known SNR and pushes our estimates of SNR sizes to the upper limits. We investigate the environment in which the SNR is located and examine various scenarios that might explain such a large and relatively bright SNR appearance. We find that Diprotodon is most likely at a much closer distance of
$\times$152 pc. This size would qualify Diprotodon as the largest known SNR and pushes our estimates of SNR sizes to the upper limits. We investigate the environment in which the SNR is located and examine various scenarios that might explain such a large and relatively bright SNR appearance. We find that Diprotodon is most likely at a much closer distance of  $\sim$1 kpc, implying its diameter is 58
$\sim$1 kpc, implying its diameter is 58 $\times$56 pc and it is in the radiative evolutionary phase. We also present a new Fermi-LAT data analysis that confirms the angular extent of the SNR in gamma rays. The origin of the high-energy emission remains somewhat puzzling, and the scenarios we explore reveal new puzzles, given this unexpected and unique observation of a seemingly evolved SNR having a hard GeV spectrum with no breaks. We explore both leptonic and hadronic scenarios, as well as the possibility that the high-energy emission arises from the leftover particle population of a historic pulsar wind nebula.
$\times$56 pc and it is in the radiative evolutionary phase. We also present a new Fermi-LAT data analysis that confirms the angular extent of the SNR in gamma rays. The origin of the high-energy emission remains somewhat puzzling, and the scenarios we explore reveal new puzzles, given this unexpected and unique observation of a seemingly evolved SNR having a hard GeV spectrum with no breaks. We explore both leptonic and hadronic scenarios, as well as the possibility that the high-energy emission arises from the leftover particle population of a historic pulsar wind nebula.
Social connection is associated with better health, including reduced risk of dementia. Personality traits are also linked to cognitive outcomes; neuroticism is associated with increased risk of dementia. Personality traits and social connection are also associated with each other. Taken together, evidence suggests the potential impacts of neuroticism and social connection on cognitive outcomes may be linked. However, very few studies have simultaneously examined the relationships between personality, social connection and health.
We tested the association between neuroticism and cognitive measures while exploring the potential mediating roles of aspects of social connection (loneliness and social isolation).
We conducted a cross-sectional study with a secondary analysis of the Canadian Longitudinal Study on Aging (CLSA) Comprehensive Cohort, a sample of Canadians aged 45 to 85 years at baseline. We used only self-reported data collected at the first follow-up, between 2015 and 2018 (n= 27,765). We used structural equation modelling to assess the association between neuroticism (exposure) and six cognitive measures (Rey Auditory Verbal Learning Test immediate recall and delayed recall, Animal Fluency Test, Mental Alternation Test, Controlled Oral Word Association Test and Stroop Test interference ratio), with direct and indirect effects (through social isolation and loneliness). We included age, education and hearing in the models and stratified all analyses by sex, females (n= 14,133) and males (n=13,632).
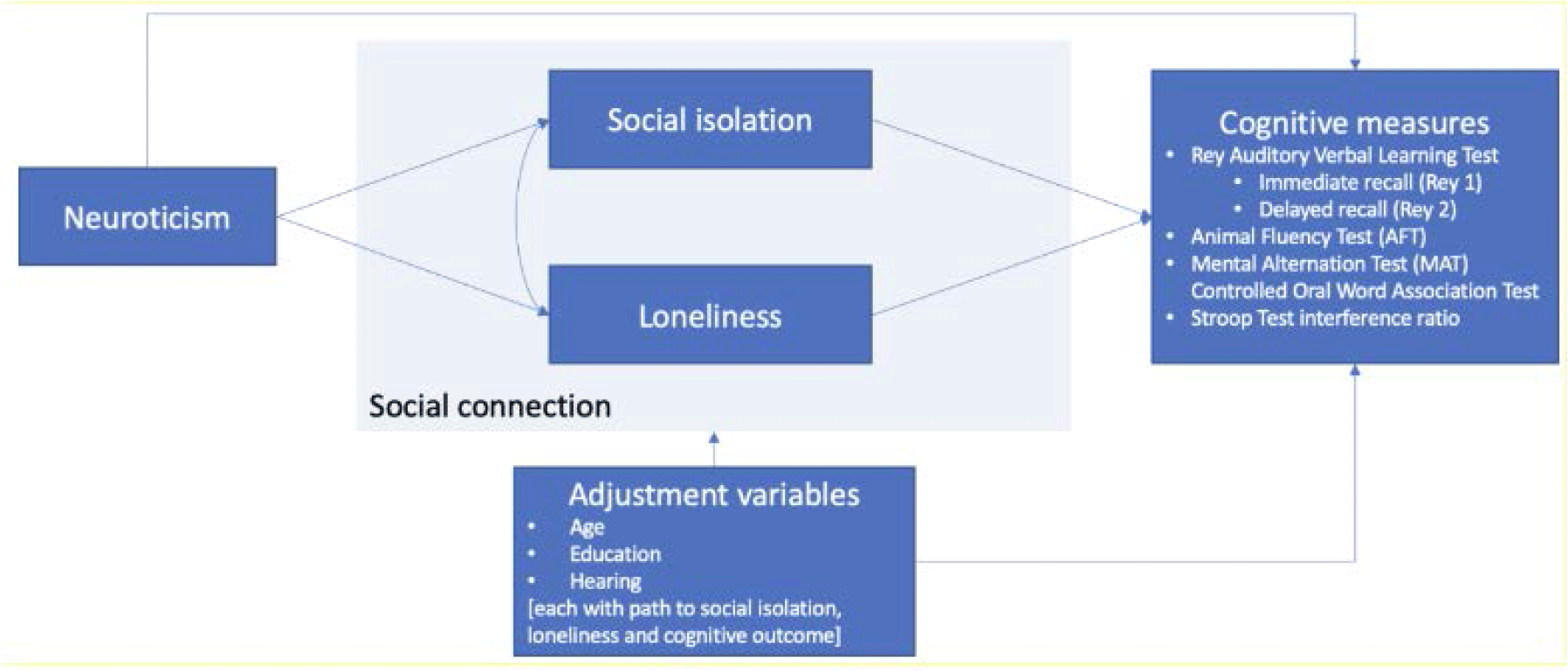
We found positive, statistically significant associations between neuroticism and social isolation (p<0.05) and loneliness (p<0.05), for both males and females. We also found inverse, statistically significant associations between neuroticism and all cognitive measures (p<0.05), except the Stroop Test interference ratio. In these models, there was consistent evidence of indirect effects (through social isolation and loneliness) and, in some cases, evidence of direct effects. We found sex differences in the model results.
Our findings suggest that the association between neuroticism and cognitive outcomes may be mediated by aspects of social connection and differ by sex. Understanding if and how modifiable risk factors mediate the association between personality and cognitive outcomes would help develop and target intervention strategies that improve social connection and brain health.
The remnant phase of a radio galaxy begins when the jets launched from an active galactic nucleus are switched off. To study the fraction of radio galaxies in a remnant phase, we take advantage of a  $8.31$ deg
$8.31$ deg $^2$ subregion of the GAMA 23 field which comprises of surveys covering the frequency range 0.1–9 GHz. We present a sample of 104 radio galaxies compiled from observations conducted by the Murchison Widefield Array (216 MHz), the Australia Square Kilometer Array Pathfinder (887 MHz), and the Australia Telescope Compact Array (5.5 GHz). We adopt an ‘absent radio core’ criterion to identify 10 radio galaxies showing no evidence for an active nucleus. We classify these as new candidate remnant radio galaxies. Seven of these objects still display compact emitting regions within the lobes at 5.5 GHz; at this frequency the emission is short-lived, implying a recent jet switch off. On the other hand, only three show evidence of aged lobe plasma by the presence of an ultra-steep-spectrum (
$^2$ subregion of the GAMA 23 field which comprises of surveys covering the frequency range 0.1–9 GHz. We present a sample of 104 radio galaxies compiled from observations conducted by the Murchison Widefield Array (216 MHz), the Australia Square Kilometer Array Pathfinder (887 MHz), and the Australia Telescope Compact Array (5.5 GHz). We adopt an ‘absent radio core’ criterion to identify 10 radio galaxies showing no evidence for an active nucleus. We classify these as new candidate remnant radio galaxies. Seven of these objects still display compact emitting regions within the lobes at 5.5 GHz; at this frequency the emission is short-lived, implying a recent jet switch off. On the other hand, only three show evidence of aged lobe plasma by the presence of an ultra-steep-spectrum ( $\alpha<-1.2$) and a diffuse, low surface brightness radio morphology. The predominant fraction of young remnants is consistent with a rapid fading during the remnant phase. Within our sample of radio galaxies, our observations constrain the remnant fraction to
$\alpha<-1.2$) and a diffuse, low surface brightness radio morphology. The predominant fraction of young remnants is consistent with a rapid fading during the remnant phase. Within our sample of radio galaxies, our observations constrain the remnant fraction to  $4\%\lesssim f_{\mathrm{rem}} \lesssim 10\%$; the lower limit comes from the limiting case in which all remnant candidates with hotspots are simply active radio galaxies with faint, undetected radio cores. Finally, we model the synchrotron spectrum arising from a hotspot to show they can persist for 5–10 Myr at 5.5 GHz after the jets switch of—radio emission arising from such hotspots can therefore be expected in an appreciable fraction of genuine remnants.
$4\%\lesssim f_{\mathrm{rem}} \lesssim 10\%$; the lower limit comes from the limiting case in which all remnant candidates with hotspots are simply active radio galaxies with faint, undetected radio cores. Finally, we model the synchrotron spectrum arising from a hotspot to show they can persist for 5–10 Myr at 5.5 GHz after the jets switch of—radio emission arising from such hotspots can therefore be expected in an appreciable fraction of genuine remnants.

