Refine search
Actions for selected content:
48206 results in Zoology
A comparison of total cost estimates between exclusive breast-feeding and breast milk substitute usage in humanitarian contexts
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 03 November 2023, pp. 3162-3172
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Trimethylamine increases intestinal fatty acid absorption: in vitro studies in a Caco-2 cell culture system
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 03 November 2023, e108
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Effects of a front-of-package disclosure on accuracy in assessing children’s drink ingredients: two randomised controlled experiments with US caregivers of young children
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 01 November 2023, pp. 2790-2801
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Interventions to improve the nutritional status of children under 5 years in Ethiopia: a systematic review
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 3147-3161
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Evaluation of food purchasing in the Brazilian School Feeding Programme: feasibility of the requirements and recommendations
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 3331-3342
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Parents’ experiences of infant and young child feeding during the COVID-19 pandemic in Ireland
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 2652-2662
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring feasibility and acceptability of an integrated urban gardens and peer nutritional counselling intervention for people with HIV in the Dominican Republic
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 3134-3146
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Harnessing the power on our plates: sustainable dietary patterns for public and planetary health
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 82 / Issue 4 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 437-453
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
How healthy and affordable are foods and beverages sold in school canteens? A cross-sectional study comparing menus from Victorian primary schools – ERRATUM
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, p. 3379
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Sleep deprivation in development of obesity, effects on appetite regulation, energy metabolism, and dietary choices
-
- Journal:
- Nutrition Research Reviews / Volume 38 / Issue 1 / June 2025
- Published online by Cambridge University Press:
- 31 October 2023, pp. 4-24
-
- Article
- Export citation
Dietary chenodeoxycholic acid attenuates high-fat diet-induced growth retardation, lipid accumulation and bile acid metabolism disorder in the liver of yellow catfish Pelteobagrus fulvidraco
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 6 / 28 March 2024
- Published online by Cambridge University Press:
- 31 October 2023, pp. 921-934
- Print publication:
- 28 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
Consumption of foods with the highest nutritional quality, and the lowest greenhouse gas emissions and price, differs between socio-economic groups in the UK population
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 3370-3378
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Social and ecological disparities in anaemia among adolescent girls 15–19 years old in Nepal
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 2973-2981
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Development and internal validation of the SMILE-FSS: a Free Sugars Screener for Australian children aged 2 and 5 years
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 31 October 2023, pp. 2691-2703
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association of the timing of evening eating with BMI Z-score and waist-to-height ratio among preschool-aged children in Finland
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 31 October 2023, pp. 911-920
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
Joint effects between cadmium exposure and dietary antioxidant quality score on osteoporosis and bone mineral density
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 6 / 28 March 2024
- Published online by Cambridge University Press:
- 31 October 2023, pp. 956-963
- Print publication:
- 28 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
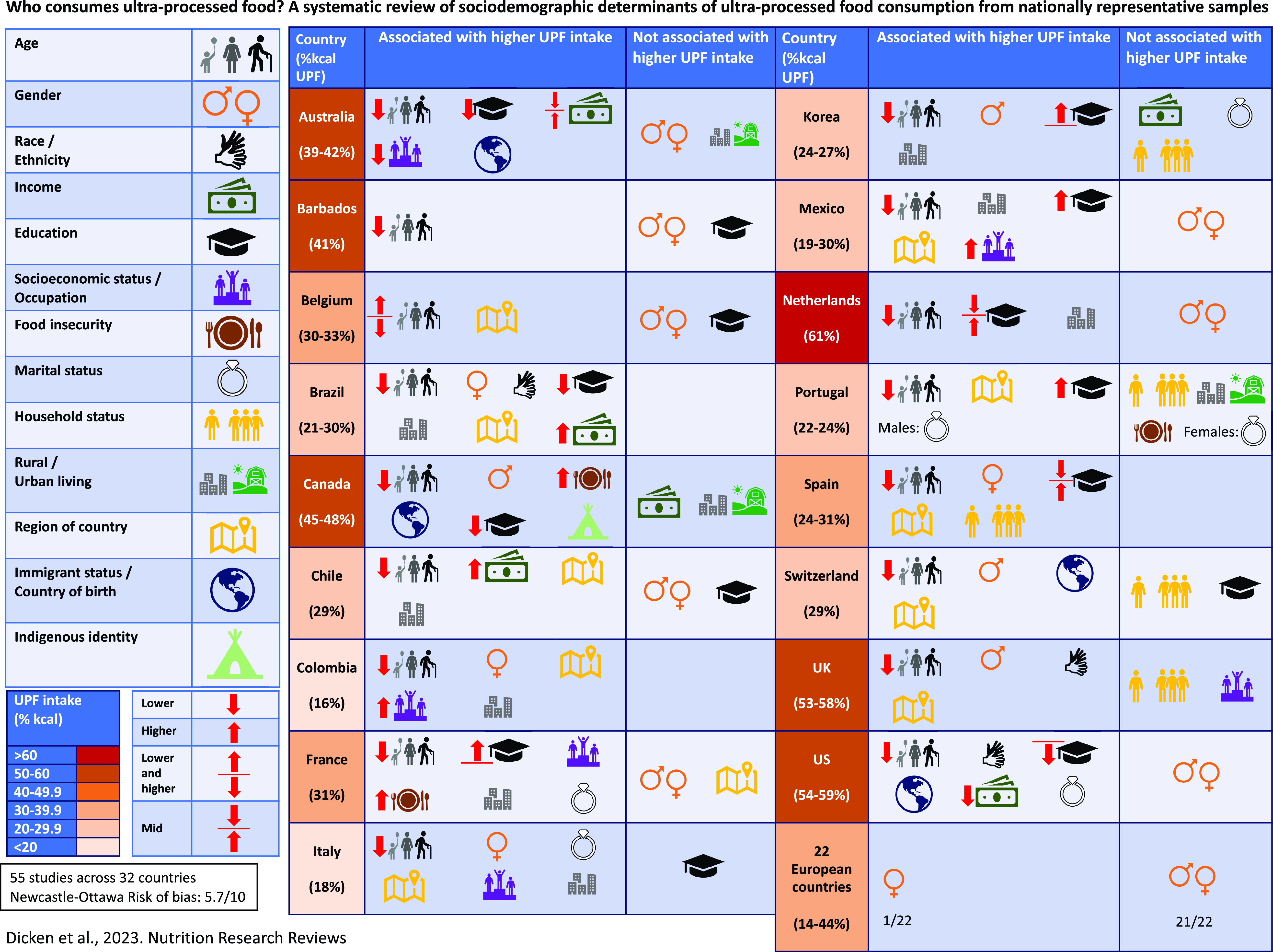
Who consumes ultra-processed food? A systematic review of sociodemographic determinants of ultra-processed food consumption from nationally representative samples
- Part of
-
- Journal:
- Nutrition Research Reviews / Volume 37 / Issue 2 / December 2024
- Published online by Cambridge University Press:
- 31 October 2023, pp. 416-456
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Trends and long-term variation explaining nutritional determinants of child linear growth: analysis of Bangladesh Demographic and Health Surveys 1996–2018
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 27 October 2023, pp. 2758-2770
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nutrition and immunity: lessons from coronavirus disease-2019
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 1 / February 2025
- Published online by Cambridge University Press:
- 27 October 2023, pp. 8-23
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring the feasibility of using evidence-based feeding practices to promote children’s healthy eating in holiday clubs
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 27 October 2023, pp. 2868-2881
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
