Refine search
Actions for selected content:
48206 results in Zoology
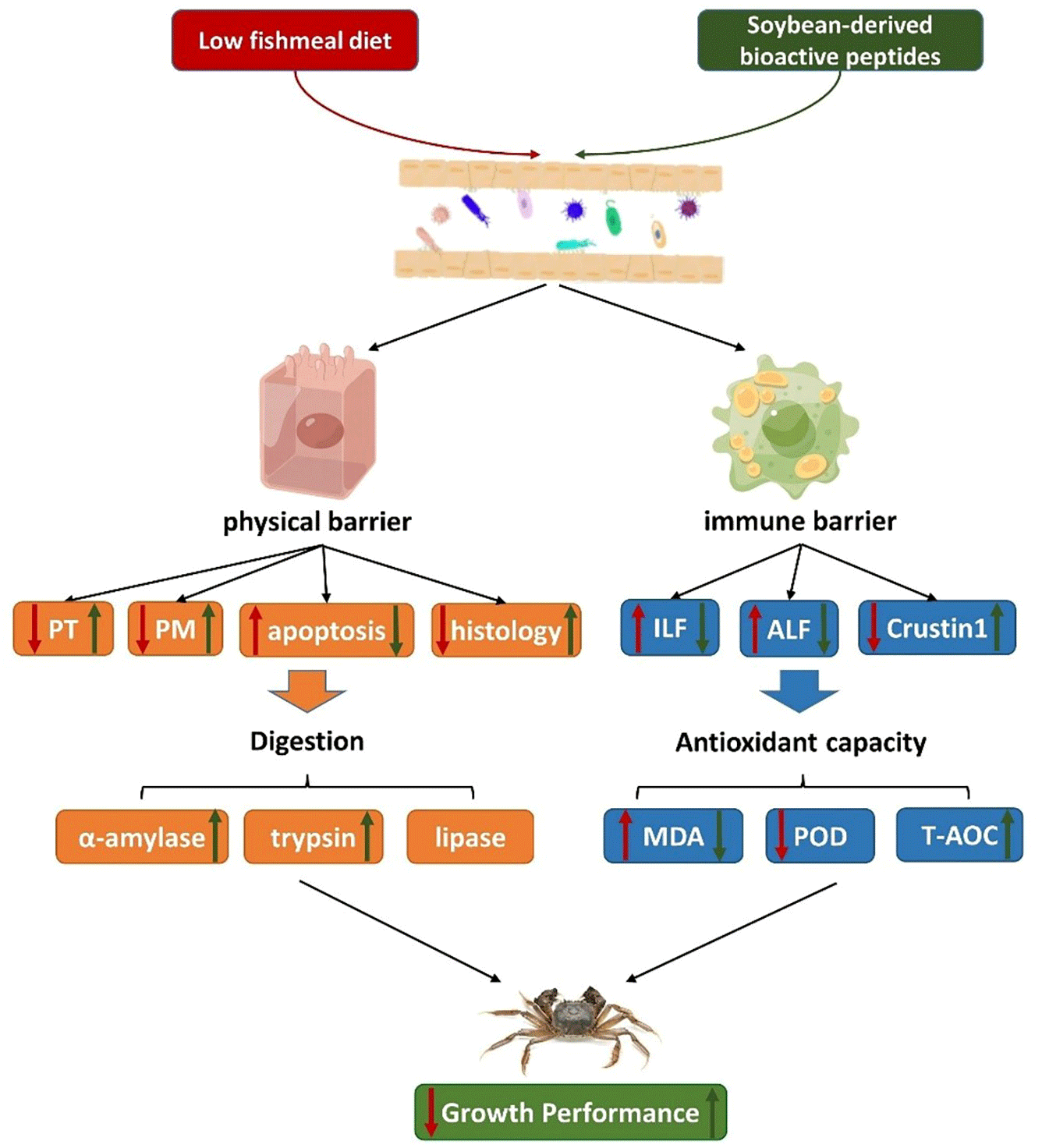
Promotion of improved intestinal barrier health by soybean-derived bioactive peptides in Chinese mitten crab (Eriocheir sinensis) fed a low fishmeal diet
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 6 / 28 March 2024
- Published online by Cambridge University Press:
- 27 October 2023, pp. 974-986
- Print publication:
- 28 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
Time-resolved concentrations of serum amino acids, one-carbon metabolites and B-vitamin biomarkers during the postprandial and fasting state: the Postprandial Metabolism in Healthy Young Adults (PoMet) Study
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 27 October 2023, pp. 786-800
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Clinical impacts of n-3 fatty acids supplementation on depression symptoms: an umbrella review of meta-analyses
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 27 October 2023, pp. 841-850
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
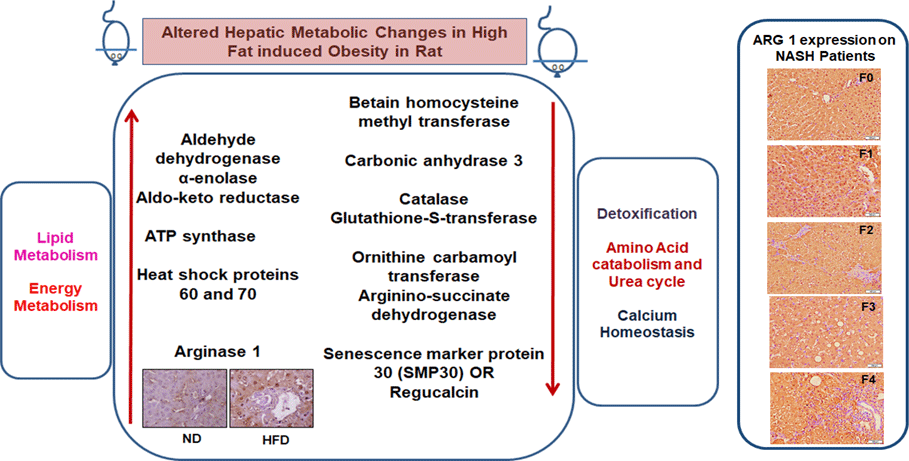
Early hepatic proteomic signatures reveal metabolic changes in high-fat-induced obesity in rats
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 27 October 2023, pp. 773-785
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
Parental support for free school lunches in Australian primary schools: associated factors and perceived barriers
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 26 October 2023, pp. 3320-3330
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
How effective is public health policy in Scotland on vitamin D deficiency during pregnancy?
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 26 October 2023, pp. 3311-3319
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nutritional, environmental and economic impacts of ultra-processed food consumption in Australia
- Part of
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 26 October 2023, pp. 3359-3369
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Associations of free, bioavailable and total 25-hydroxyvitamin D with neonatal birth anthropometry and calcium homoeostasis in mother–child pairs in a sunny Mediterranean region
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 26 October 2023, pp. 801-808
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nutritional and health benefits and risks of plant-based substitute foods
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 1 / February 2025
- Published online by Cambridge University Press:
- 26 October 2023, pp. 110-123
-
- Article
-
- You have access
- HTML
- Export citation
The kinetics of amino acid disappearance in the small intestine is related to the extent of amino acids absorbed in growing pigs
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 26 October 2023, pp. 762-772
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The impact of botanical fermented foods on metabolic syndrome and type 2 diabetes: a systematic review of randomised controlled trials
-
- Journal:
- Nutrition Research Reviews / Volume 37 / Issue 2 / December 2024
- Published online by Cambridge University Press:
- 26 October 2023, pp. 396-415
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An investigation into the preparation of powdered infant formula in households in Ireland – CORRIGENDUM
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue 3 / September 2024
- Published online by Cambridge University Press:
- 26 October 2023, p. 218
-
- Article
-
- You have access
- HTML
- Export citation

Living with obesity in Ireland: determinants, policy and future perspectives
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue 2 / May 2024
- Published online by Cambridge University Press:
- 26 October 2023, pp. 82-94
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Selenium status and its determinants in very old adults: insights from the Newcastle 85+ Study
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 25 October 2023, pp. 901-910
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring high-protein diets in the context of cardiac rehabilitation
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 84 / Issue 1 / February 2025
- Published online by Cambridge University Press:
- 25 October 2023, pp. 75-86
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Fish oil minimises feed intake and improves insulin sensitivity in Zucker fa/fa rats
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 25 October 2023, pp. 749-761
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
A comparative analysis of nutrition-related assessment criteria and associated nutrition performance scores of food companies across three prominent corporate sustainability assessment tools
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 23 October 2023, pp. 2677-2690
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Provision of dietary education in UK-based cardiac rehabilitation: a cross-sectional survey conducted in conjunction with the British Association for Cardiovascular Prevention and Rehabilitation
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 23 October 2023, pp. 880-893
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association between nut consumption and low muscle strength among Korean adults
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 5 / 14 March 2024
- Published online by Cambridge University Press:
- 23 October 2023, pp. 894-900
- Print publication:
- 14 March 2024
-
- Article
-
- You have access
- HTML
- Export citation
Effect of probiotics on postmenopausal bone health: a preclinical meta-analysis
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 4 / 28 February 2024
- Published online by Cambridge University Press:
- 23 October 2023, pp. 567-580
- Print publication:
- 28 February 2024
-
- Article
-
- You have access
- HTML
- Export citation
