Refine search
Actions for selected content:
48206 results in Zoology
Efficacy of a school-based education intervention on the consumption of fruits, vegetables and carbonated soft drinks among adolescents
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 02 October 2023, pp. 3112-3121
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Association of dietary intake with micronutrient deficiency in Indian school children: a cross-sectional study
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 02 October 2023, e104
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Food literacy and diet quality in young vegans, lacto-ovo vegetarians, pescatarians, flexitarians and omnivores
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 02 October 2023, pp. 3051-3061
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Characterisation of Indian gut microbiome for B-vitamin production and its comparison with Chinese cohort
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 4 / 28 February 2024
- Published online by Cambridge University Press:
- 02 October 2023, pp. 686-697
- Print publication:
- 28 February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Effects of front-of-package caffeine and sweetener disclaimers in Mexico: cross-sectional results from the 2020 International Food Policy Study
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 02 October 2023, pp. 3278-3290
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Fat-free mass may play a dominant role in the association between systolic blood pressure and body composition in children and adolescents
-
- Journal:
- British Journal of Nutrition / Volume 131 / Issue 4 / 28 February 2024
- Published online by Cambridge University Press:
- 29 September 2023, pp. 622-629
- Print publication:
- 28 February 2024
-
- Article
-
- You have access
- HTML
- Export citation
PHN volume 26 issue 10 Cover and Front matter
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. f1-f3
-
- Article
-
- You have access
- Open access
- Export citation
Household food insecurity in South Africa from 1999 to 2021: a metrics perspective
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. 2183-2199
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
PHN volume 26 issue 10 Cover and Back matter
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. b1
-
- Article
-
- You have access
- Open access
- Export citation
Feasibility of a food-based diabetes self-management education intervention for food insecure patients with type 2 diabetes: a convergent mixed methods study
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 28 September 2023, pp. 3100-3111
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Developing food-based dietary recommendations in the UK
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 27 September 2023, pp. 55-61
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The association of socio-demographic and environmental factors with stunting among under-five children in Hawassa City, Sidama National Regional State, Ethiopia – CORRIGENDUM
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 27 September 2023, e101
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Magnitude of undernutrition and its association with dietary diversity among older persons in Ethiopia: a systematic review and meta-analysis, 2023
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 26 September 2023, e102
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Are epigenetic mechanisms and nutrition effective in male and female infertility?
-
- Journal:
- Journal of Nutritional Science / Volume 12 / 2023
- Published online by Cambridge University Press:
- 26 September 2023, e103
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
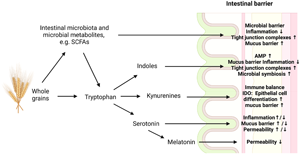
The effects of whole grain cereals on tryptophan metabolism and intestinal barrier function: underlying factors of health impact
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 26 September 2023, pp. 42-54
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Factors associated with eating rate: a systematic review and narrative synthesis informed by socio-ecological model
-
- Journal:
- Nutrition Research Reviews / Volume 37 / Issue 2 / December 2024
- Published online by Cambridge University Press:
- 26 September 2023, pp. 376-395
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Nutritional practices to manage menstrual cycle related symptoms: a systematic review
-
- Journal:
- Nutrition Research Reviews / Volume 37 / Issue 2 / December 2024
- Published online by Cambridge University Press:
- 25 September 2023, pp. 352-375
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Bringing down barriers to children’s healthy eating: a critical review of opportunities, within a complex food system
-
- Journal:
- Nutrition Research Reviews / Volume 37 / Issue 2 / December 2024
- Published online by Cambridge University Press:
- 25 September 2023, pp. 331-351
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Addressing food insecurity: what is the role of healthcare?
- Part of
-
- Journal:
- Proceedings of the Nutrition Society / Volume 83 / Issue 3 / September 2024
- Published online by Cambridge University Press:
- 25 September 2023, pp. 151-156
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The extent and nature of children’s involvement in food practice research: a scoping review of qualitative studies
-
- Journal:
- Public Health Nutrition / Volume 26 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 25 September 2023, pp. 2836-2848
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
