Refine listing
Actions for selected content:
1419572 results in Open Access
Preliminary Report on Symptoms of Anxiety, Depression, and PTSD Following Severe Flooding in Brazil: A Longitudinal Perspective
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 19 / 2025
- Published online by Cambridge University Press:
- 16 July 2025, e189
-
- Article
- Export citation
Flow-induced vibration of a cylinder subjected to proximity interference by a downstream-cylinder
-
- Journal:
- Journal of Fluid Mechanics / Volume 1015 / 25 July 2025
- Published online by Cambridge University Press:
- 16 July 2025, A16
-
- Article
- Export citation
-
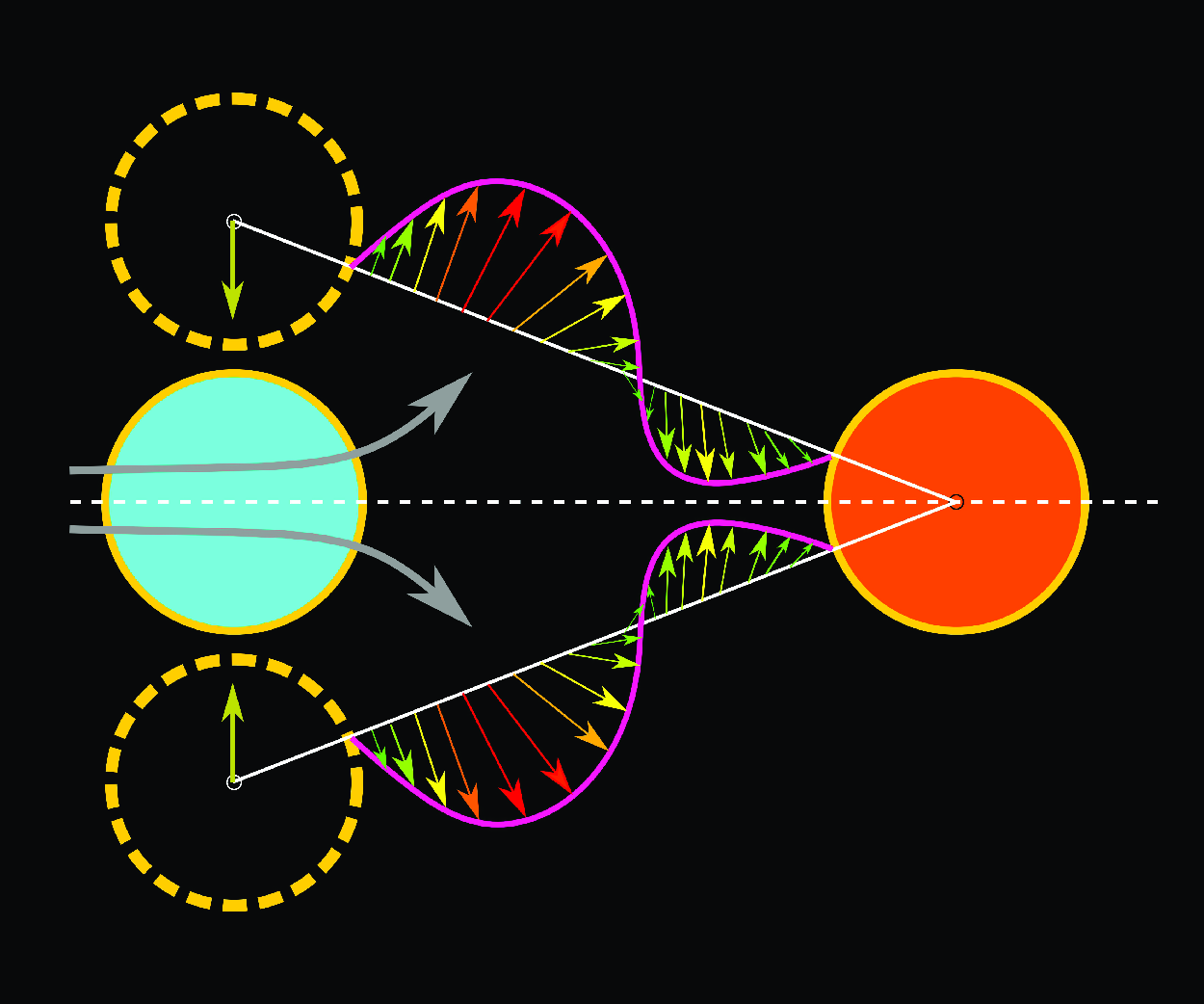
A numerical study is presented on flow-induced vibration of a circular cylinder, under the effect of a downstream stationary cylinder-induced proximity interference. The interference-induced various types of gap-flow regimes and characteristics of vibration and gap-flow rate
 $Q^*_g$ are presented, by considering various non-dimensional gaps
$Q^*_g$ are presented, by considering various non-dimensional gaps  $G^* = 0.1{-}2.5$ and reduced velocities
$G^* = 0.1{-}2.5$ and reduced velocities  $U^* = 3{-}20$ at a constant Reynolds number
$U^* = 3{-}20$ at a constant Reynolds number  $Re = 100$, mass ratio
$Re = 100$, mass ratio  $m^*= 2$ and damping ratio
$m^*= 2$ and damping ratio  $\zeta = 0.005$. Decreasing
$\zeta = 0.005$. Decreasing  $G^*$ or increasing proximity leads to the four gap-flow regimes: bi-directional gap flow at
$G^*$ or increasing proximity leads to the four gap-flow regimes: bi-directional gap flow at  $G^* \geqslant 1.0$, uni-directional non-orthogonal gap flow at
$G^* \geqslant 1.0$, uni-directional non-orthogonal gap flow at  $G^* = 1.5{-}1.0$, uni-directional orthogonal gap flow at
$G^* = 1.5{-}1.0$, uni-directional orthogonal gap flow at  $G^* \leqslant 0.5$ and uni-directional one-sided gap flow at
$G^* \leqslant 0.5$ and uni-directional one-sided gap flow at  $G^* \leqslant 0.3$. Further, the respective regimes at larger
$G^* \leqslant 0.3$. Further, the respective regimes at larger  $U^*$ are associated with proximity-induced modified vortex-induced vibration (PImVIV), proximity-induced galloping (PIG), transitional PImVIV–PIG, and proximity-induced staggered vibration (PISV). Quantitative presentation of maximum gap-flow rate
$U^*$ are associated with proximity-induced modified vortex-induced vibration (PImVIV), proximity-induced galloping (PIG), transitional PImVIV–PIG, and proximity-induced staggered vibration (PISV). Quantitative presentation of maximum gap-flow rate  $Q^*_{{g,max}}$, phase
$Q^*_{{g,max}}$, phase  $ \phi _g$ (between
$ \phi _g$ (between  $Q^*_{g}$ and displacement
$Q^*_{g}$ and displacement  $y^*$) and phase portraits (
$y^*$) and phase portraits ( $Q^*_{g}$ versus
$Q^*_{g}$ versus  $y^*$) provides clear demarcation between the various gap-flow regimes. Flow mechanisms are presented for the PImVIV, PIG and PISV responses. For the PIG, the mechanism is presented for the first time on generation of galloping instability, asymptotically increasing
$y^*$) provides clear demarcation between the various gap-flow regimes. Flow mechanisms are presented for the PImVIV, PIG and PISV responses. For the PIG, the mechanism is presented for the first time on generation of galloping instability, asymptotically increasing  $A^*$ and existence of optimum gap
$A^*$ and existence of optimum gap  $G^* = 0.5$ for the maximum amplitude. This work is significant as it provides new insights into the proximity interference-induced gap-flow dynamics between two cylinders, associated flow mechanism for both vibration mitigation and enhancement and promising potential applications for energy harvesting.
$G^* = 0.5$ for the maximum amplitude. This work is significant as it provides new insights into the proximity interference-induced gap-flow dynamics between two cylinders, associated flow mechanism for both vibration mitigation and enhancement and promising potential applications for energy harvesting.




















Modified design of sub-reflector with dielectric cylindrical keeper to enhance gain in axially displaced ellipse reflector with dual polarization
-
- Journal:
- International Journal of Microwave and Wireless Technologies / Volume 17 / Issue 4 / May 2025
- Published online by Cambridge University Press:
- 16 July 2025, pp. 613-619
-
- Article
- Export citation
How large-scale flow structures affect particle transport in wall turbulence
-
- Journal:
- Journal of Fluid Mechanics / Volume 1015 / 25 July 2025
- Published online by Cambridge University Press:
- 16 July 2025, A23
-
- Article
- Export citation
-
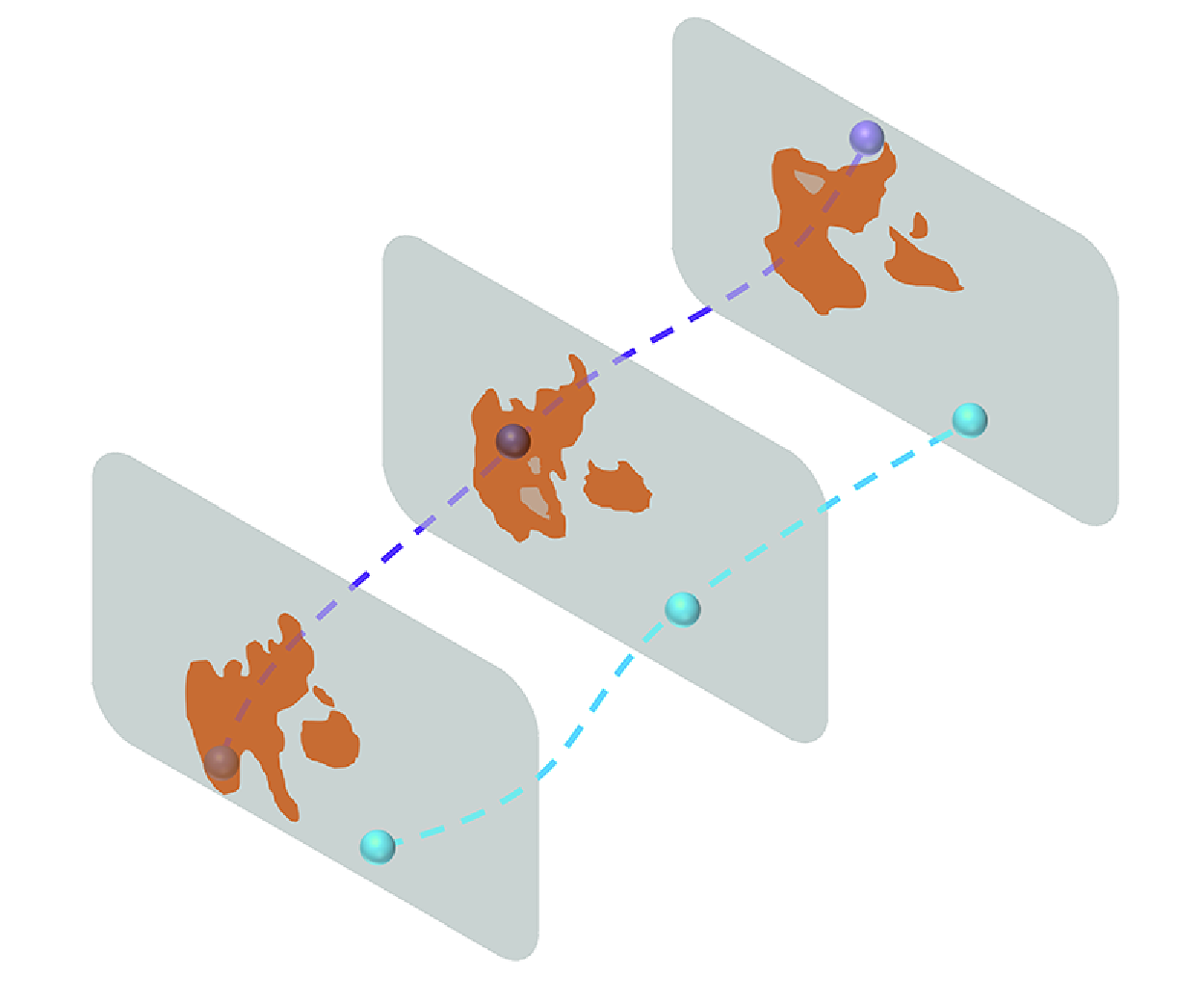
This study investigates the transport of particles in turbulent channel flow with friction Reynolds number
 $Re_\tau = 1000$ by direct numerical simulation. We focus on how large-scale flow structures, namely the
$Re_\tau = 1000$ by direct numerical simulation. We focus on how large-scale flow structures, namely the  $Qs$ structures (Lozano-Durán et al. 2012, J. Fluid Mech., vol. 694, pp. 100–130), affect the wall-normal transport of particles. Despite occupying less than
$Qs$ structures (Lozano-Durán et al. 2012, J. Fluid Mech., vol. 694, pp. 100–130), affect the wall-normal transport of particles. Despite occupying less than  $10\,\%$ of the physical domain, our results highlight the critical role played by
$10\,\%$ of the physical domain, our results highlight the critical role played by  $Qs$ structures in the particle transport, namely that the particle number and momentum flux inside the
$Qs$ structures in the particle transport, namely that the particle number and momentum flux inside the  $Qs$ structures are substantially higher than outside. The fraction of particle wall-normal momentum flux inside
$Qs$ structures are substantially higher than outside. The fraction of particle wall-normal momentum flux inside  $Qs$ structures is considerably larger than their volume fraction, suggesting highly efficient transport inside the
$Qs$ structures is considerably larger than their volume fraction, suggesting highly efficient transport inside the  $Qs$ structures. This prominent role played by
$Qs$ structures. This prominent role played by  $Qs$ structures in the transport of inertial particles is more effective by diminishing the inertia of particles. Notably, the long-distance transport of particles in the wall-normal direction is driven primarily by the continuous effect of
$Qs$ structures in the transport of inertial particles is more effective by diminishing the inertia of particles. Notably, the long-distance transport of particles in the wall-normal direction is driven primarily by the continuous effect of  $Qs$ structures. In summary, our findings advance the understanding of the effects of
$Qs$ structures. In summary, our findings advance the understanding of the effects of  $Qs$ structures on particle transport, and demonstrate their significant role in the process.
$Qs$ structures on particle transport, and demonstrate their significant role in the process.










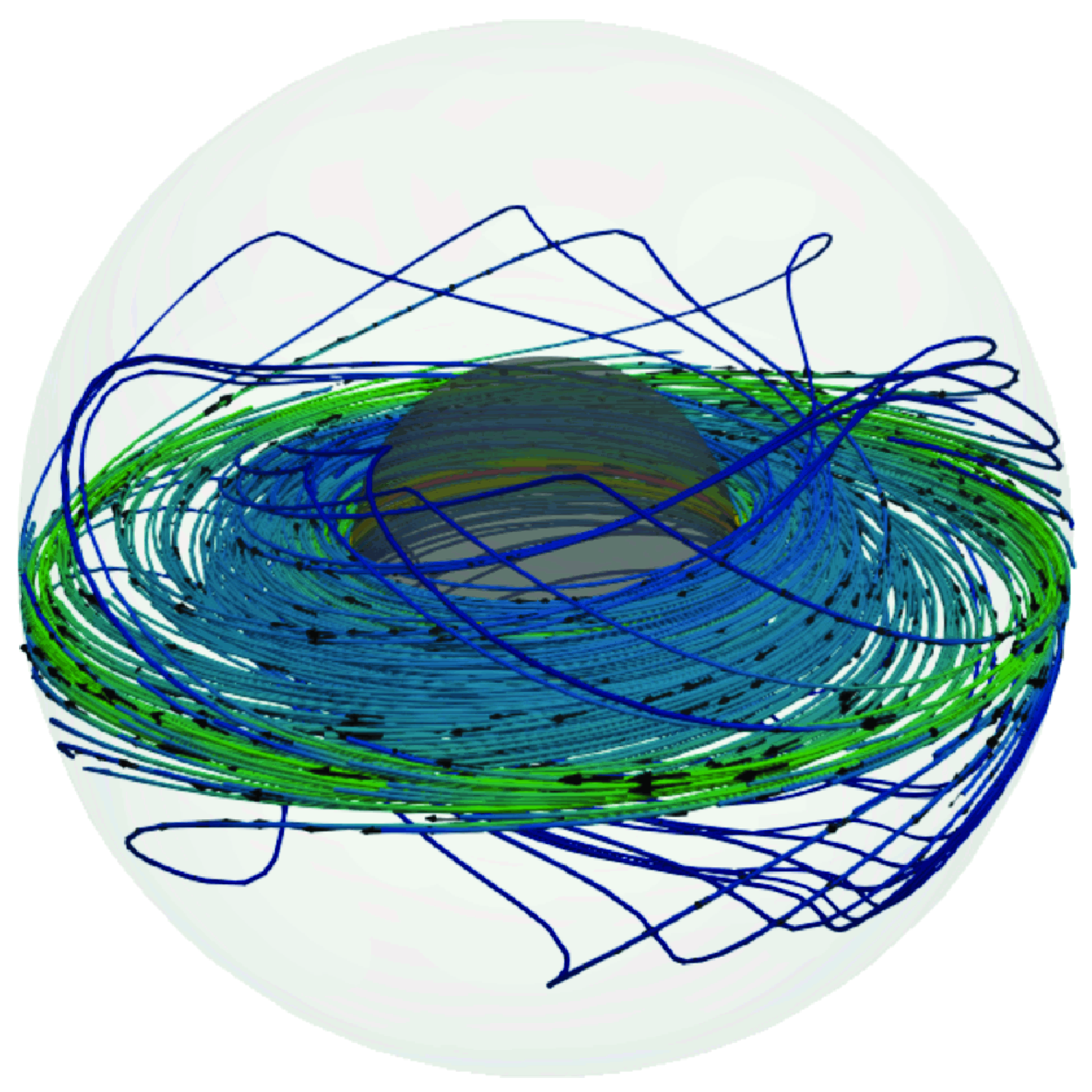
Electromagnetically driven magnetized spherical Couette flow
-
- Journal:
- Journal of Fluid Mechanics / Volume 1015 / 25 July 2025
- Published online by Cambridge University Press:
- 16 July 2025, A25
-
- Article
- Export citation
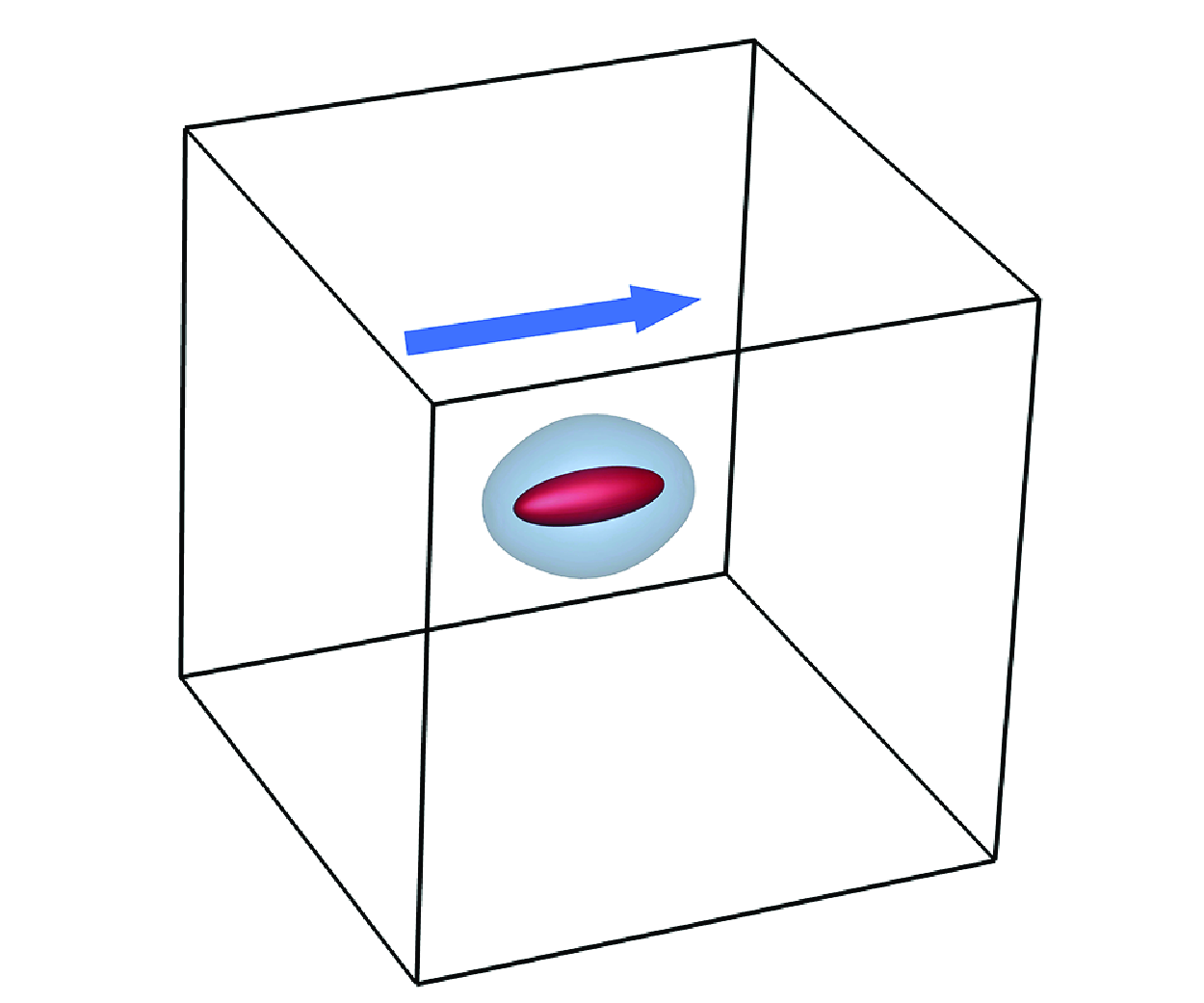
Swimming and mixing of an ellipsoidal squirmer in a viscoplastic fluid
-
- Journal:
- Journal of Fluid Mechanics / Volume 1015 / 25 July 2025
- Published online by Cambridge University Press:
- 16 July 2025, A12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
John James Quinn. Majority State Ownership of Oil and Mining Sectors in Africa: The Resource Curse Undermined. London: Routledge, 2024. xiv + 186 pp. $200.00. Hardback. ISBN: 9781138390331.
-
- Journal:
- African Studies Review , First View
- Published online by Cambridge University Press:
- 16 July 2025, pp. 1-2
-
- Article
-
- You have access
- HTML
- Export citation
“A Bold Experiment in the Technique of Administration”: Nutrition Science and Development in the Gambia, 1946–50
-
- Journal:
- Journal of British Studies / Volume 64 / 2025
- Published online by Cambridge University Press:
- 16 July 2025, e16
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Supreme Prejudice: Examining the Supreme Court’s Racial & Criminal Biases
-
- Journal:
- Journal of Race, Ethnicity and Politics / Volume 10 / Issue 3 / November 2025
- Published online by Cambridge University Press:
- 16 July 2025, pp. 791-813
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Gender and Australian school leaders’ experiences of workplace violence by students, parents, and colleagues
- Part of
-
- Journal:
- The Economic and Labour Relations Review ,
- Published online by Cambridge University Press:
- 16 July 2025, pp. 1-20
-
- Article
-
- You have access
- Open access
- HTML
- Export citation

Revisiting the hydrodynamic modulation of short surface waves by longer waves
-
- Journal:
- Journal of Fluid Mechanics / Volume 1015 / 25 July 2025
- Published online by Cambridge University Press:
- 16 July 2025, A20
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
Hydrodynamic modulation of short ocean surface waves by longer ambient waves significantly influences remote sensing, interpretation of in situ wave measurements and numerical wave forecasting. This paper revisits the wave crest and action conservation laws and derives steady, nonlinear, analytical solutions for the change of short-wave wavenumber, action and gravitational acceleration due to the presence of longer waves. We validate the analytical solutions with numerical solutions of the full crest and action conservation equations. The nonlinear analytical solutions of short-wave wavenumber, amplitude and steepness modulation significantly deviate from the linear analytical solutions of Longuet-Higgins & Stewart (1960 J. Fluid Mech. vol. 8, no. 4, pp. 565–583) and are similar to the nonlinear numerical solutions by Longuet-Higgins (1987 J. Fluid Mech. vol. 177, pp. 293–306) and Zhang & Melville (1990 J. Fluid Mech. vol. 214, pp. 321–346). The short-wave steepness modulation is attributed 5/8 to wavenumber, 1/4 due to wave action and 1/8 due to effective gravity. Examining the homogeneity and stationarity requirements for the conservation of wave action reveals that stationarity is a stronger requirement and is generally not satisfied for very steep long waves. We examine the results of Peureux et al. (2021 J. Geophys. Res.: Oceans vol. 126, no. 1, e2020JC016735) who found through numerical simulations that the short-wave modulation grows unsteadily with each long-wave passage. We show that this unsteady growth only occurs for homogeneous initial conditions as a special case and not generally. The proposed steady solutions are a good approximation of the nonlinear crest-action conservation solutions in long-wave steepness
 $\lesssim 0.2$. Except for a subset of initial conditions, the solutions to the nonlinearised crest-action conservation equations are mostly steady in the reference frame of the long waves.
$\lesssim 0.2$. Except for a subset of initial conditions, the solutions to the nonlinearised crest-action conservation equations are mostly steady in the reference frame of the long waves.

Bucking the Buck: US Financial Sanctions & the International Backlash against the Dollar. By Daniel McDowell. New York: Oxford University Press, 2023. 238p.
-
- Journal:
- Perspectives on Politics / Volume 23 / Issue 3 / September 2025
- Published online by Cambridge University Press:
- 16 July 2025, pp. 1196-1197
- Print publication:
- September 2025
-
- Article
- Export citation

Streaming and diffusion in the cochlea
-
- Journal:
- Journal of Fluid Mechanics / Volume 1015 / 25 July 2025
- Published online by Cambridge University Press:
- 16 July 2025, A15
-
- Article
- Export citation
The Collaborative Innovation Effect of ESG Signals: Integrating Signaling and Trust Theories
-
- Journal:
- Management and Organization Review / Volume 21 / Issue 1 / February 2025
- Published online by Cambridge University Press:
- 15 July 2025, pp. 73-101
-
- Article
- Export citation
MOR volume 21 issue 1 Cover and Front matter
-
- Journal:
- Management and Organization Review / Volume 21 / Issue 1 / February 2025
- Published online by Cambridge University Press:
- 15 July 2025, pp. f1-f3
-
- Article
-
- You have access
- Export citation
DEGENERATIONS OF ORBIFOLD CURVES AS NONCOMMUTATIVE VARIETIES
- Part of
-
- Journal:
- Nagoya Mathematical Journal , First View
- Published online by Cambridge University Press:
- 15 July 2025, pp. 1-19
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An Exploratory 12-Month Observational Study of Adults with Spinal Muscular Atrophy: Learning From Our Tools
-
- Journal:
- Canadian Journal of Neurological Sciences , First View
- Published online by Cambridge University Press:
- 15 July 2025, pp. 1-10
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Complications of Middle Meningeal Artery Embolization for Chronic Subdural Hematoma: A Systematic Literature Review
-
- Journal:
- Canadian Journal of Neurological Sciences , First View
- Published online by Cambridge University Press:
- 15 July 2025, pp. 1-11
-
- Article
- Export citation

Excavating Alcatrazes, Santiago Island, Cape Verde: early colonial impacts on land, people and material culture
-
- Journal:
- Antiquity , First View
- Published online by Cambridge University Press:
- 15 July 2025, pp. 1-9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Genetic variation and population structure of Haemonchus contortus: an in-silico analysis
-
- Journal:
- Journal of Helminthology / Volume 99 / 2025
- Published online by Cambridge University Press:
- 15 July 2025, e78
-
- Article
- Export citation
